Download presentation
Presentation is loading. Please wait.

1
SPOTLIGHT ON MENTAL HEALTH Yelizaveta Sher, M.D. Department of Psychosomatic Medicine Meg Dvorak, LCSW Adult CF Social Worker

2
TIDES: The International Depression Epidemiological Study 154 cystic fibrosis centers in 9 countries (Europe & US) 6,088 patients w/ CF (12 yo & up), and 4,102 caregivers of children w/ CF, birth-18 yo ↑depression in 10% of adolescents, 19% of adults, 37% of mothers and 31% of fathers. ↑ anxiety in 22% of adolescents, 32% of adults, 48% of mothers and 36% of fathers. Elevations 2–3 times ↑ those of community samples. Quittner AL, Goldbeck L, Abbott J, et al. Thorax 2014

3
Cystic Fibrosis & Mental Health Psychological distress in CF is associated with: ↓pulmonary function ↑ hospitalizations ↑ healthcare costs ↓ health-related quality of life Study comparing adolescents with CF & depression vs no dep: Those who were depressed were 3X more likely to be hospitalized for a pulmonary exacerbation, and incurred ↑healthcare costs over 2 years Quittner AL, Goldbeck L, Abbott J, et al. Thorax 2014

4
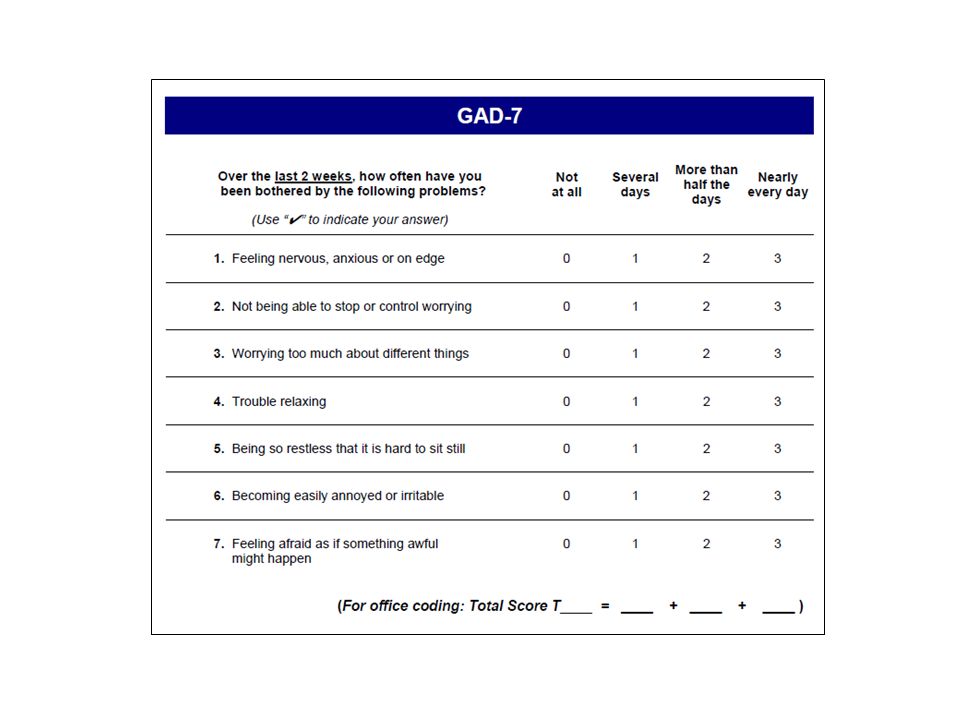
CFF and ECFS International Committee on Mental Health in CF (ICMH) Guidelines Prevention: – Ongoing education & preventative, supportive interventions – Behavioral approaches be used to reduce the risk of distress Screening – Annual screening for adolescents and adults with CF (ages 12–adulthood) with PHQ-9 and GAD-7 – Annual screening of caregivers of children and adolescents – Screening of children (<12) if one caregiver is depressed or there is concern Quittner A et al, Thorax 2015
 Guidelines Prevention: – Ongoing education & preventative, supportive interventions – Behavioral approaches be used to reduce the risk of distress Screening – Annual screening for adolescents and adults with CF (ages 12–adulthood) with PHQ-9 and GAD-7 – Annual screening of caregivers of children and adolescents – Screening of children (<12) if one caregiver is depressed or there is concern Quittner A et al, Thorax 2015")
5
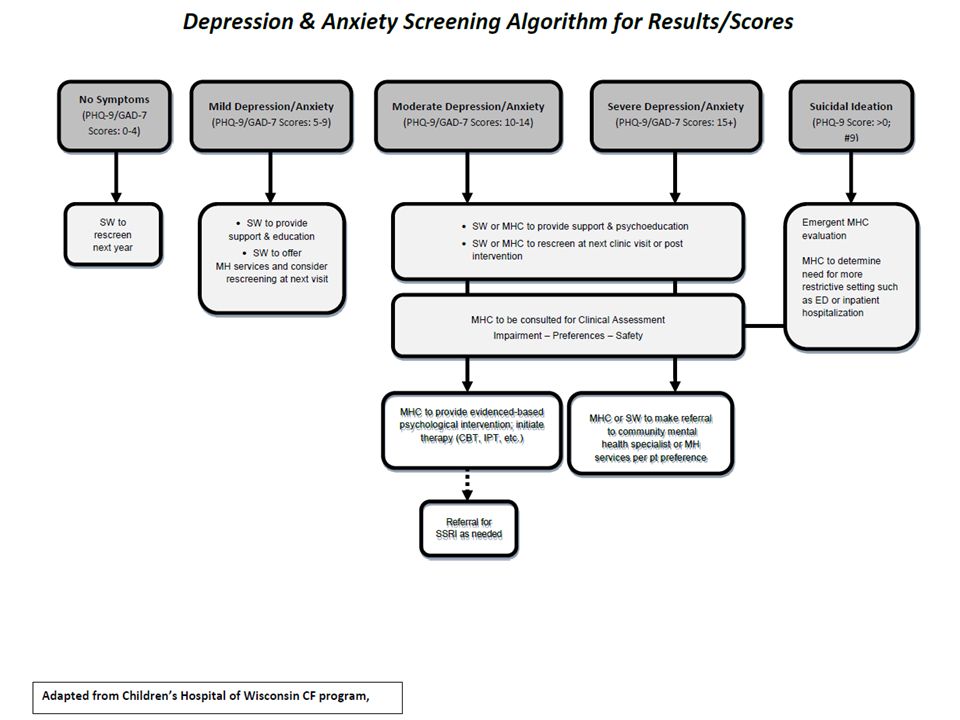
CFF and ECFS International Committee on Mental Health in CF (ICMH) Guidelines Clinical Assessment/Intervention: – Clinically evaluate elevated scores and refer to PCP/MH as needed – Use flexible, stepped care model of clinical intervention – Based on severity and availability, use evidence- based psychological interventions and/or pharmacotherapy Quittner A et al, Thorax 2015
 Guidelines Clinical Assessment/Intervention: – Clinically evaluate elevated scores and refer to PCP/MH as needed – Use flexible, stepped care model of clinical intervention – Based on severity and availability, use evidence- based psychological interventions and/or pharmacotherapy Quittner A et al, Thorax 2015")
6
Depression Dysthymia Depression 2/2 Medical Illness Bipolar Disorder, Depressed Adjustment Disorder w/ Depressed Mood MDD Substance- Induced Mood Disorder Demoralization Normal Reaction to Stress

7
Depression Dysthymia Depression 2/2 Medical Illness Bipolar Disorder, Depressed Adjustment disorder w/ depressed mood MDD Substance- Induced Mood Disorder Demoralization Normal Reaction to Stress 5 + symptoms x 2 weeks: depressed mood ↓ interest/pleasure Changes in appetite and/or sleep psychomotor changes low energy worthlessness or guilt ↓concentration thoughts of death, suicidal ideations, attempt

8
Depression Dysthymia Depression 2/2 Medical Illness Bipolar Disorder, Depressed Adjustment Disorder w/ Depressed Mood MDD Substance- Induced Mood Disorder Demoralization Normal Reaction to Stress Symptoms within 3 months of the stressor onset Marked distress in excess of expected and significant impairment in functioning Sxs do not persist 6 months after stressor termination

9
Depression Dysthymia Depression 2/2 Medical Illness Bipolar Disorder, Depressed Adjustment Disorder w/ Depressed Mood MDD Substance- Induced Mood Disorder Demoralization Normal Reaction to Stress Episodes of mania or hypomania in addition to depressed episodes Depression may be characterized by hypersomnia, hyperphagia, mood reactivity Very different treatment from unipolar depression

10
Anxiety PTSD Medications: Steroids Albuterol Thyroid meds Stimulants Theophylline Medical Conditions: Hypoxia Metabolic Infection Tumor Adjustment do w/ anxious mood GAD Panic Disorder Phobias OCD American Psychiatric Association, 2013, DSM 5

11
Anxiety PTSD Medications: Steroids Albuterol Thyroid meds Stimulants Theophylline Medical Conditions: Hypoxia Metabolic Infection Tumor Adjustment do w/ anxious mood GAD Panic Disorder Phobias OCD Excessive anxiety and worry x 6 months about few things Associated with 3+: Restlessness Easily fatigued Diff concentrating Irritability Muscle tension Sleep disturbance Impairment Not due to effects of substance or illness American Psychiatric Association, 2013, DSM 5

12
Anxiety PTSD Medications: Steroids Albuterol Thyroid meds Stimulants Theophylline Medical Conditions: Hypoxia Metabolic Infection Tumor Adjustment do w/ anxious mood GAD Panic Disorder Phobias OCD Presence of obsessions, compulsions or both Obsessions – recurrent thoughts, urges, images Compulsions – repetitive behaviors in response to obsession to decrease anxiety Time-consuming or cause sign distress (1+ hr/day) Not due to effects of substance or medical illness American Psychiatric Association, 2013, DSM 5
 Not due to effects of substance or medical illness American Psychiatric Association, 2013, DSM 5")
13
Anxiety PTSD Medications: Steroids Albuterol Thyroid meds Stimulants Theophylline Medical Conditions: Hypoxia Metabolic Infection Tumor Adjustment do w/ anxious mood GAD Panic Disorder Phobias OCD Recurrent unexpected panic attacks AND Attack(s) followed by 1 month of 1+ of following: Persistent concern about having additional attacks Worry about the implications of the attack Significant change in behavior related to the attacks +/- Agoraphobia Impairment Not due to effects of substance or illness American Psychiatric Association, 2013, DSM 5
 followed by 1 month of 1+ of following: Persistent concern about having additional attacks Worry about the implications of the attack Significant change in behavior related to the attacks +/- Agoraphobia Impairment Not due to effects of substance or illness American Psychiatric Association, 2013, DSM 5")
14
Anxiety PTSD Medications: Steroids Albuterol Thyroid meds Stimulants Theophylline Medical Conditions: Hypoxia Metabolic Infection Tumor Adjustment do w/ anxious mood GAD Panic Disorder Phobias OCD A. Exposure to actual/threatened death, serious injury or sexual violence B. Intrusion Sxs Intrusive thoughts Nightmares Flashbacks Psychological and/or physiologic distress with reminders C. Avoidance of stimuli and numbing D. Negative alterations in mood and cognitions E. Changes in arousal and reactivity F. Lasts for > 1 month American Psychiatric Association, 2013, DSM 5

15
Diet Exercise Physical health Support Psychotherapy Medications Treatment

16
Psychodynamic Therapy – Understanding of how one’s past shapes today Motivational Interviewing – Patient-focused; eliciting talk of change from the patient Cognitive Behavioral Therapy – relationship between thoughts, emotions, and behaviors Interpersonal Therapy – social support; changes in role functioning ; resolution of grief Existential Psychotherapy – Meaning of life; dealing with death and grief Mindfulness – Staying in the moment; focus on now Supportive Psychotherapy – Active listening; problem solving Treatment: Psychotherapy

17
Pharmacotherapy MAOIs TCAs SSRIs SNRIs Atypicals: mirtazapine, buproprion, vilazodone Augmentors: lithium, thyroid, aripiprazole

18
Percent of Patients 18 Years and Older with Depression,2005-2014

19
Percent of Patients 18 Years and Older with Depression in 2014,by Center

22
Adult Mental Health Coordinator 3 year grant through CFF Faculty psychiatrist embedded in CF clinic Expertise in CF, lung txp, psychosomatic medicine Work closely with LCSW to improve screening process

23
Bridging the Mental Health Gap Access to MH services now MH screening, referral MH system broken Medi-Cal, GHPP Private insurance Patients – Depression as barrier – CF as barrier Providers – Expensive – Don’t take insurance Improvements with MHC Services embedded in CF clinic Evidenced based interventions in your clinic appointment * Access to medications Increased focus on MH Improved data tracking for research and QI Psychiatrist with CF expertise

Similar presentations




















 Excessive anxiety & worry (apprehensive expectation) occuring more days than.>")
