Download presentation
Presentation is loading. Please wait.

1
中枢神经系统血管炎 James Jinxing Wang, MD, PhD Clinical Assistant Professor University of TN Memphis, TN jjxwang@yahoo.com

7
Classification of CNS vasculitis INFECTIOUS VASCULITIS -- Spirochetal (syphilis) -- Mycobacterial -- Fungal -- Rickettsial -- Bacterial (purulent) meningitis -- Viral -- Other organisms NECROTIZING VASCULITIDES -- Classic polyarteritis nodosa -- Wegener’s granulomatosis -- Allergic Angitis and granulomatosis (Churg- Strauss) -- Necrotizing systemic vasculitis-overlap syndrome -- Lymphomatoid granulomatosis VASCULITIS ASSOCIATED WITH COLLAGEN VASCULAR DISEASES -- Systemic lupus erythematosus -- Rheumatoid arthritis -- Scleroderma -- Sjogren’s syndrome GIANT CELL ARTERITIDES -- Takayasu’s arteritis -- Temporal (cranial) arteritis VASCULITIS ASSOCIATED WITH OTHER SYSTEMIC DISEASES -- Behcet’s disease -- Ulcerative colitis -- Sarcoidosis -- Relapsing polychondritis -- Kohlmeier-Degos disease HYPERSENSITIVITY VASCULITIDES -- Henoch-Schonlein purpura -- Drug-induced vasculitides -- Chemical vasculitides -- Essential mixed cryoglobulinemia MISCELLANEOUS -- Vasculitis associated with neoplasia -- Vasculitis associated with radiation -- Cogan’s syndrome -- Dermatomyositis-polymyositis -- X-linked lymphoproliferative syndrome -- Thromboangiitis obliterans -- Kawasaki syndrome PRIMARY CNS VASCULITIS
 -- Mycobacterial -- Fungal -- Rickettsial -- Bacterial (purulent) meningitis -- Viral -- Other organisms NECROTIZING VASCULITIDES -- Classic polyarteritis nodosa -- Wegener’s granulomatosis -- Allergic Angitis and granulomatosis (Churg- Strauss) -- Necrotizing systemic vasculitis-overlap syndrome -- Lymphomatoid granulomatosis VASCULITIS ASSOCIATED WITH COLLAGEN VASCULAR DISEASES -- Systemic lupus erythematosus -- Rheumatoid arthritis -- Scleroderma -- Sjogren’s syndrome GIANT CELL ARTERITIDES -- Takayasu’s arteritis -- Temporal (cranial) arteritis VASCULITIS ASSOCIATED WITH OTHER SYSTEMIC DISEASES -- Behcet’s disease -- Ulcerative colitis -- Sarcoidosis -- Relapsing polychondritis -- Kohlmeier-Degos disease HYPERSENSITIVITY VASCULITIDES -- Henoch-Schonlein purpura -- Drug-induced vasculitides -- Chemical vasculitides -- Essential mixed cryoglobulinemia MISCELLANEOUS -- Vasculitis associated with neoplasia -- Vasculitis associated with radiation -- Cogan’s syndrome -- Dermatomyositis-polymyositis -- X-linked lymphoproliferative syndrome -- Thromboangiitis obliterans -- Kawasaki syndrome PRIMARY CNS VASCULITIS")
8
History b 1922 Harbitz’s first report. b 1959 Gravioto and Feigin’s extensive autopsy descriptions b 1970s Primary CNS angiitis, Granulomatous angiitis of the CNS, isolated CNS angiitis. b 1980s High dose steroid and Cyclophosphamide started. b Prognosis is very poor without treatment. Mortality is almost 100% without treatment

9
Pathology of the isolated CNS vasculitis The essential feature is a giant cell, granulomatous inflammation of the small arteries and veins, which exhibits a nearly constant affinity for the vessels of the leptomeninges and the branches that arise from them to penetrate the cortex. The size is 2-300 micron.

10
Animal Models b Intrvanous injection of Mycoplasma b gallisepticum in turkeys produced similar b damage as human vasculitis.

13
Clinical Presentation AUTOPSYBIOPSY SYMPTOMS OR CASES CASES SIGNS (N = 45) (N = 26) SIGNS (N = 45) (N = 26)_____________________________________________________________________ Altered mentation 3976%1142% Headache 29641350 Hemiparesis 20441142 Stupor or coma 1942 415 Dysphasia 14311142 Seizures 1329 831 “Eye signs”1533 312 Paraparesis1124 415 Ataxia 818 935 Fever 818` 312 Papilledema 920 1 4 Weight Loss 818 0 0
 (N = 26) SIGNS (N = 45) (N = 26)_____________________________________________________________________ Altered mentation 3976%1142% Headache Hemiparesis Stupor or coma Dysphasia Seizures Eye signs Paraparesis Ataxia Fever 818` 312 Papilledema Weight Loss")
14
Diagnostic Testing-1 Labs: CBC Anti-BM abs, ANCA, ACE, SSA, SSB, FANA, RF, Cryoglobulin, etc ESR, C-reactive protein Normal ESR for man is age/2, for women is (age +10)/2. Corrected ESR = ESR – (standard Hct-actual Hct) x 1.75. Standard Hct is 45 for man, 42 for women.
 x Standard Hct is 45 for man, 42 for women..")
15
Initial ESR (n=47) Less than 20 mm/hr 22 47% 21-40 14 30% 41-60 7 15% 61-80 3 6% >81 1 2%
 Less than 20 mm/hr 22 47% % % % >81 1 2%")
16
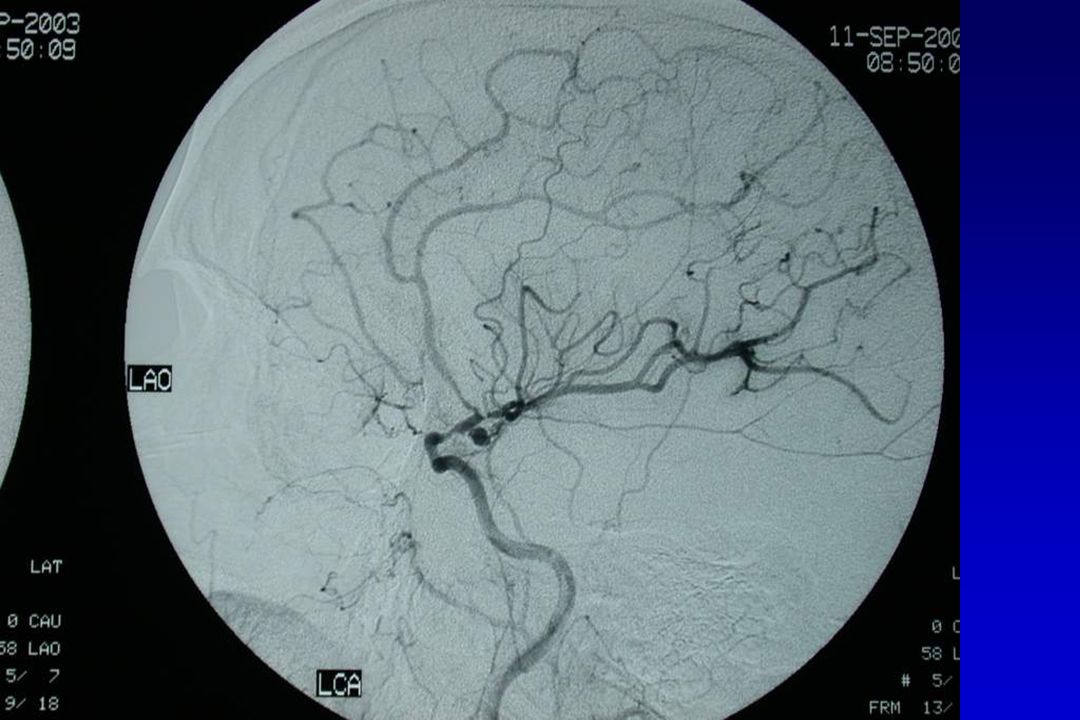
Diagnostic studies for CNS vasculitis TESTSENSITIVITY ESTIMATED SPECIFICITY CT33-50% Data not available (even lbiopsy-proven cases) no pathognomonic findings MRI50-100% Data not available (It approaches 100% in histo- no patholognomonic findings logically confirmed cases, and is lowest in those diagnosed only by angiography) ANGI-30-100% 22% ography(It is less than 40% in Assessed in only one study but histologically confirmed may be higher if vasculitis is cases, and 100% in reports secondary to other causes are not supported by histology) excluded) BIOPSY75% 80% (The negativity can be due The same pattern of inflammation to the patchy nature of the can be due to other causes disease and small tissue sample
 no pathognomonic findings MRI50-100% Data not available (It approaches 100% in histo- no patholognomonic findings logically confirmed cases, and is lowest in those diagnosed only by angiography) ANGI % 22% ography(It is less than 40% in Assessed in only one study but histologically confirmed may be higher if vasculitis is cases, and 100% in reports secondary to other causes are not supported by histology) excluded) BIOPSY75% 80% (The negativity can be due The same pattern of inflammation to the patchy nature of the can be due to other causes disease and small tissue sample")
17
Biller “VASCULITIS” Look-Alikes on Cerebral Angiography ____________________________________________ CONDITIONAUTHOR(S) ___________________________________________________________ Neoplastic angioendotheliosis Witt et al. Spasm after subarachnoid hemnorrhageFerris and Levine AtherosclerosisFerris and Levine Oral contraceptive use Irey et al. Hypertension with pheochromocytomaALrmstrong and Hayes, Postpartum Garner et al. Eclampsia Trommer, Homer, and MigraineSchon and Harrison Postcoital headache (?)Kapoor, Kendall, TraumaSuwanwela and Surgical manipulation of intracranial arteriesKhodadad “Reversible cerebral segmental vasoconstriction”Call et al. Sumatriptan and isometheptane
Kapoor, Kendall, TraumaSuwanwela and Surgical manipulation of intracranial arteriesKhodadad Reversible cerebral segmental vasoconstriction Call et al. Sumatriptan and isometheptane.")
18
Diagnostic Testing-3 b CSF: Very sensitive, but not specific b 90% abnormal

19
Differential Diagnosis b 1. CVA b 2. MS b 3. Infection b 4. Tumor b 5. Specific / systemic vasculitis b 6. Toxic b 7. Leukodystrophy b 8. MERRF, MELAS b 9. Hypertensive encephalopathy

21
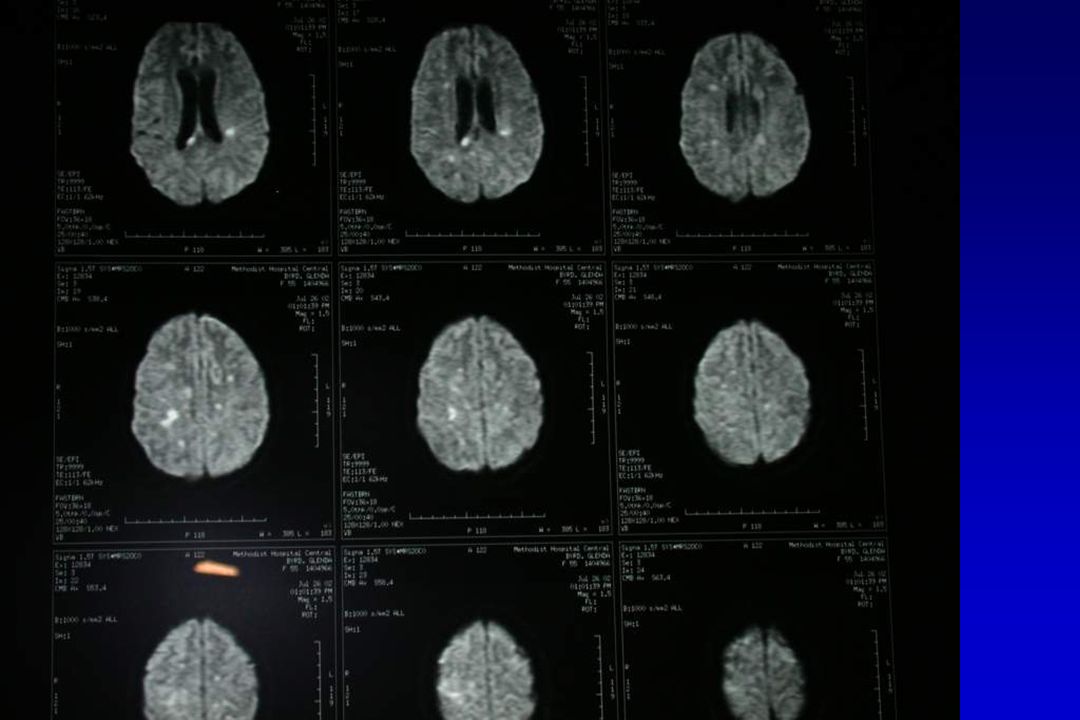
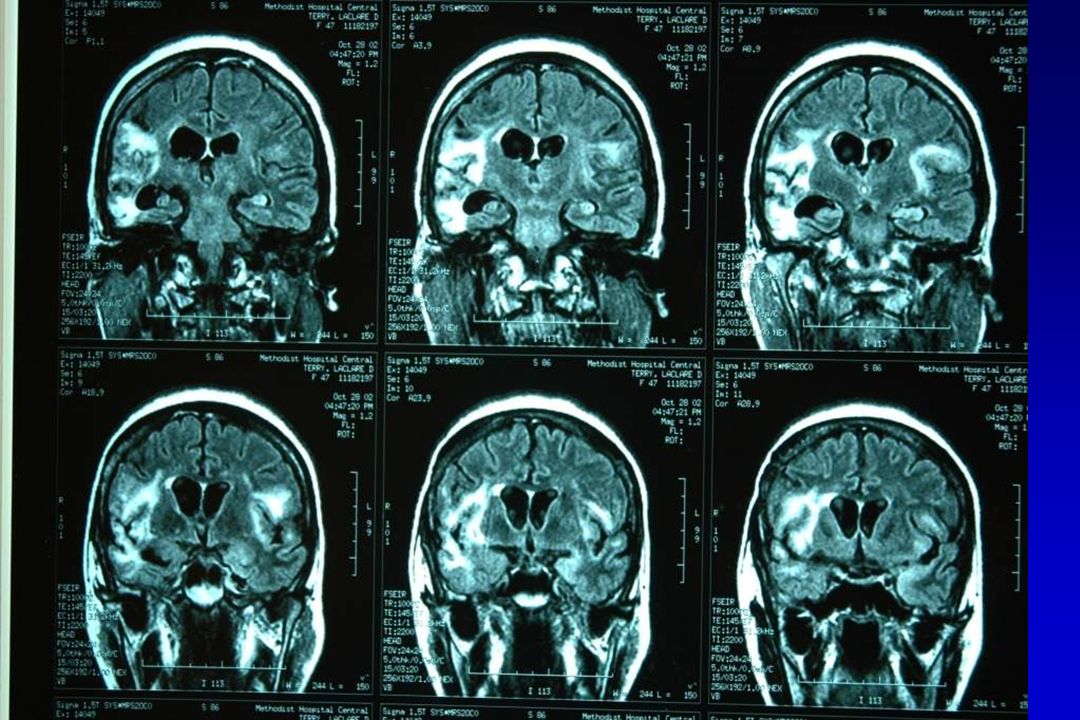
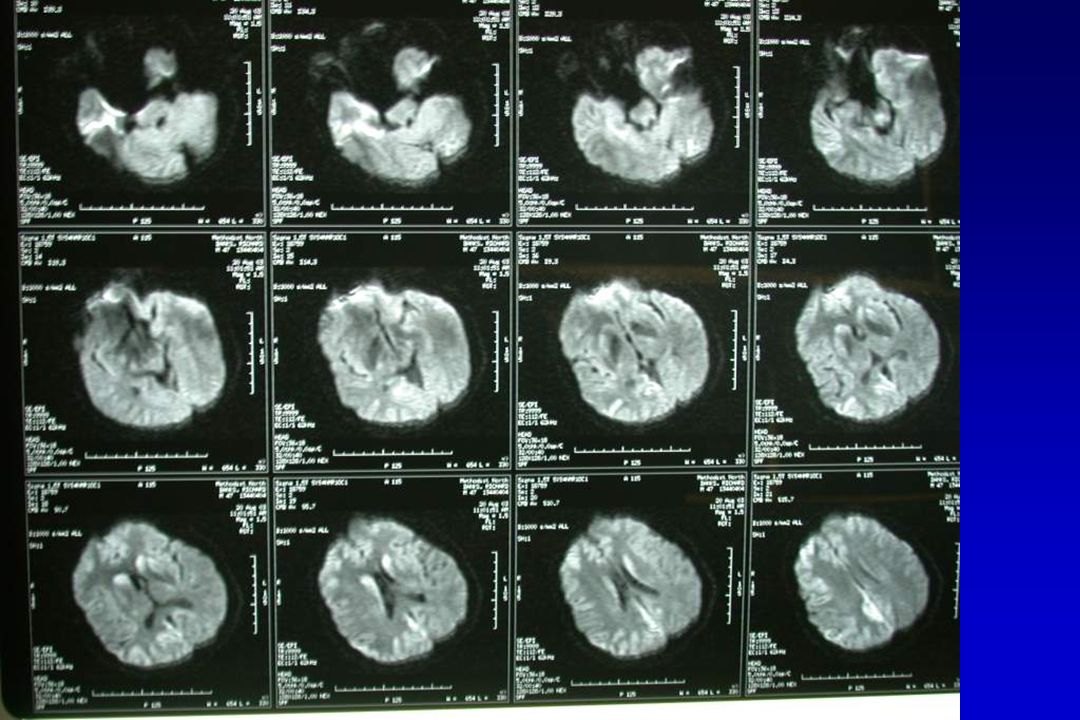
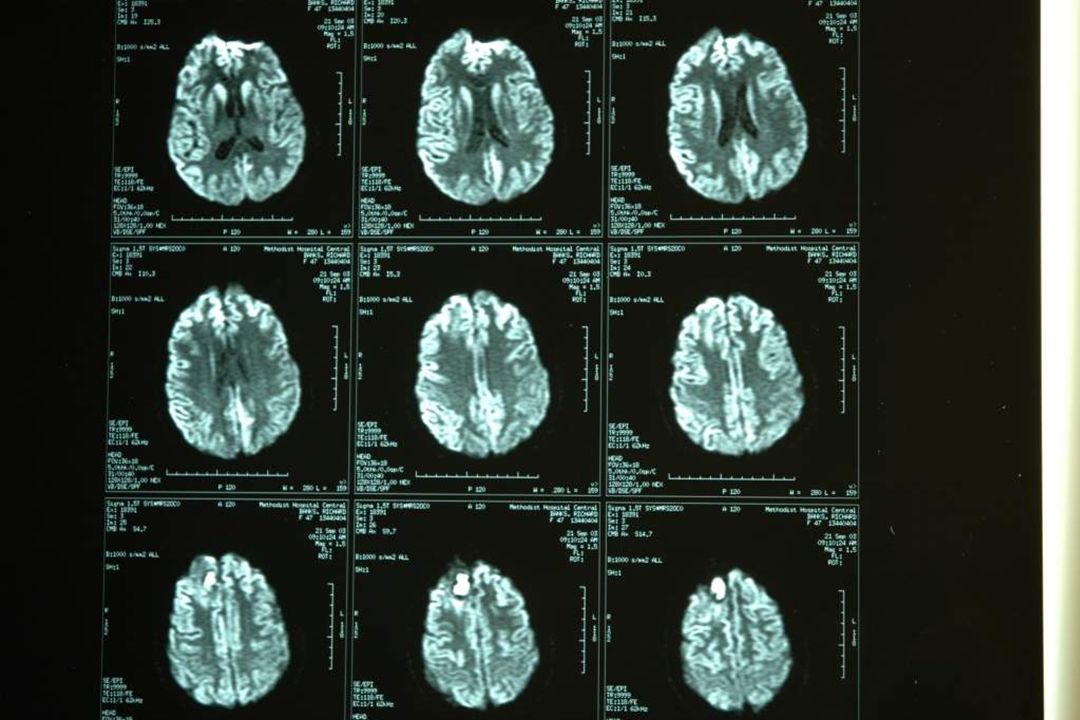
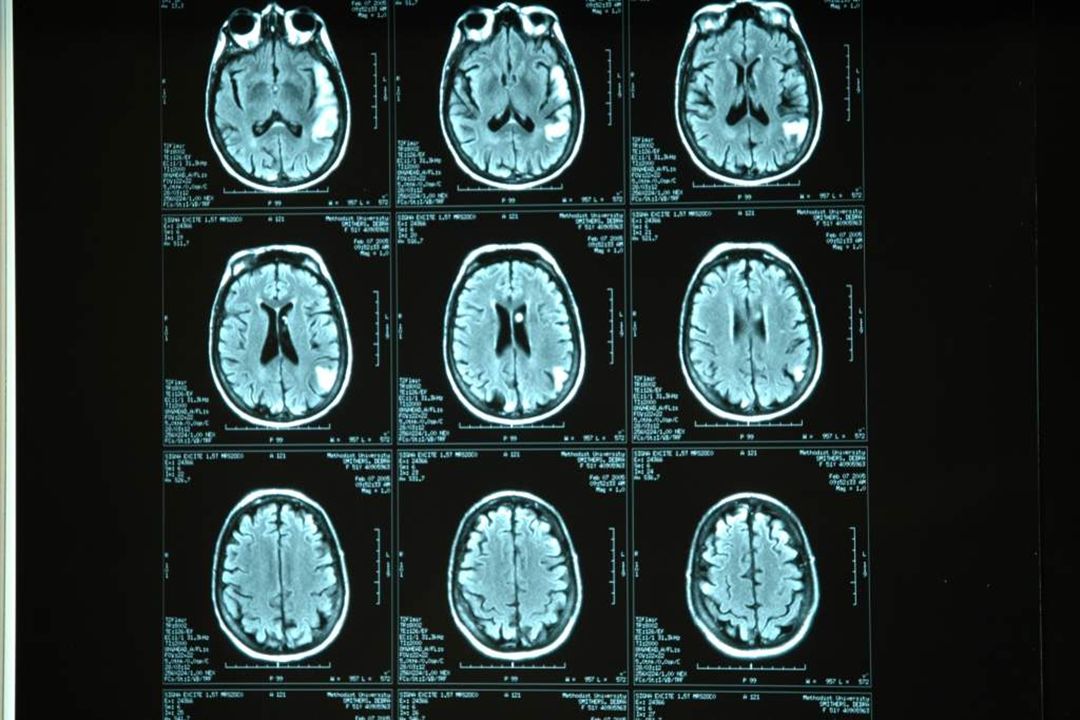
7-26-08 8-3-08 82 y/o WF with no PMH admitted because of MS change 7-26-08

37
MELAS DNA testing MELAS 3243-tRNA leu 3243G MELAS 3271-tRNA leu T3271C MELAS 3252-tRNA leu A3252G MELAS 3256-tRNA leu C3256T MELAS 3291-tRNA leu T3291C MELAS 13,513-ND5 G13513A

39
Treatment for CNS vasculitis CYTOXIC AGENT CORTICOSTEROIDS _____________________________________________ Induction Cyclophosphamide 2mg/kd daily Prednisolone 1mg/kg daily therpay by mouth (max 150mg); lower (max 80mg); Reduce weekly to 4 – 6 mo dose by 25mg if >60 years WBC 10mg/day by 6 months must be >4.0 x 10 /1 Maintenance Azathioprine 2mg/kg daily Prednisolone 5 - 10mg/day therapy 6 – 24 mo MTX Escalation Acute severe disease with creatinine >500 umol/1 or pulmonary therapy hemorrhage; Consider 7 – 10 plasma exchange treatment over 14 days such that 60 ml/kg of plasma is exchanged for 4.5% or 5% human albumin solution or consider three pulses of methylprednisolone, 15 mg/kg daily for 3 days. These patients (if under 60 years) may also require 2.5mg/kg daily of cyclophosphamide.
 may also require 2.5mg/kg daily of cyclophosphamide..")
40
Thank you!

Similar presentations



























 1936Secondary fibrositis 1945Periarthrosis humeroscapular 1946Peri-extra-articular.>")




 Dr. Raid Jastania. Vasculitis Inflammation of the walls of the vessels Causes of inflammation: –Infectious, physical, chemical,>")

