Download presentation
Presentation is loading. Please wait.

1
J.Calatayud Moscoso del Prado, D.Castellón Plaza, J.A Aguilar Arjona, R. Prada González, M. González Vázquez, C. Trinidad López Hospital POVISA Vigo, SPAIN

2
To calculate the prevalence of incidental Abdominal-CT features observed on Chest-CT To establish the effect of these finding and subsequent additional examinations in patient care

3
272 consecutive Chest-CTs were prospectively reviewed looking for presence of abdominal pathology.

4
CTs were obtained through the entire abdomen and pelvis to 2 cm above the level of the diaphragm.

5
Images were reviewed with soft tissue, lung and bone windows by two radiologist. Chest findings were classified as major, intermediate or minor based upon their impact on patient management. Follow-up information was obtained after additional examination when available.

6
MAJOR FINDINGS included indeterminate nodules, lesions that could require relatively prompt medical or surgical treatment; INTERMEDIATE FINDINGS included lesions that may eventually require medical or surgical intervention; MINOR FINDINGS included lesions that don't need further intervention;

7
Abdominal Findings were detected in 162 (60%) of 272 patients
 of 272 patients")
8
72 patients had at least one incidental finding. Of these, 41 patients had one finding, 26 had two findings, 2 had three findings and 1 had four findings. In total, 103 chest findings were detected.

9
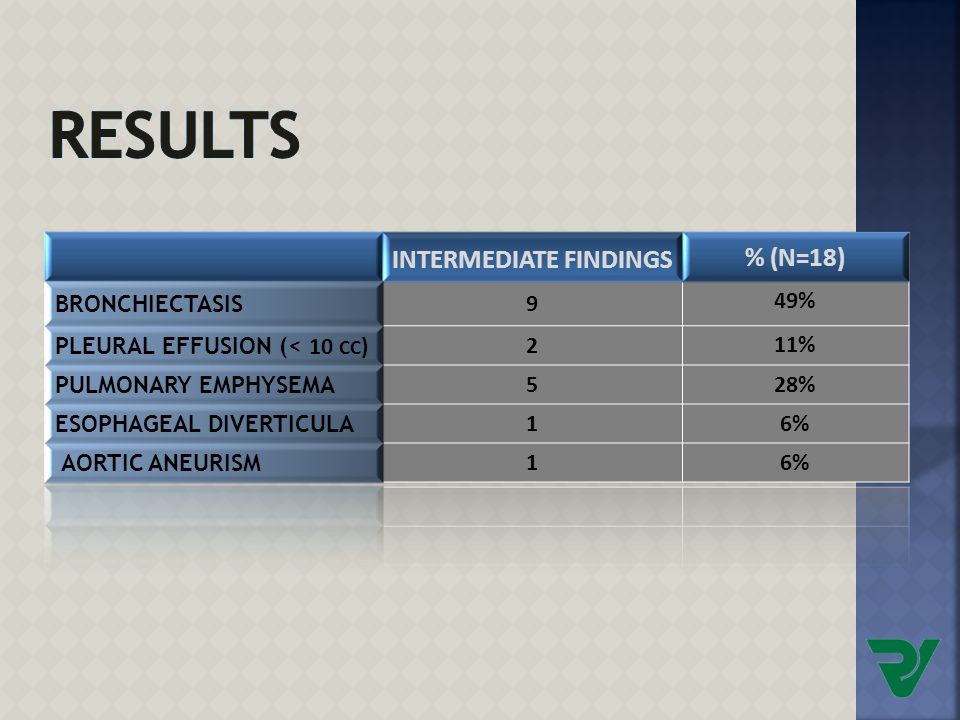
Additional explorations were recommended in 7 patients. Specific findings classified by major, intermediate and minor are shown in the next Table:

14
EXAMPLE 1 71 years old man with acute abdominal pain. Abdominal CT demostrated emphysema and inespecific pulmonary nodules. EMPHYSEMA AND PULMONARY NODULES

15
69 years old woman remited by small bowel obstruction Abdominal CT demostrated collapsed left lower lobe and massive pleural effusion. Also we detected right side cardiophrenic adenopathies. EXAMPLE 2

16
Finally, patient underwent percutaneous biposy and was diagnosticated with diffuse large B-cell Lymphoma Abdominal_CT showed peritoneal and retroperitoneal lymphadenopathies.

17
Abdominal CT revealed an adrenal carcinoma 64 years old woman with right lower quadrant pain. Transverse enhancement CT througt the lower chest showed multiple pulmonary nodules consistent with metastases. Soft-tissues window Lung window EXAMPLE 3

18
54 years old men underwent abdominal-CT to follow up diverticulitis Lower chest CT showed a left lower lobe abscess. EXAMPLE 4

19
52 years old women who come to the ER with blunt trauma. Lower chest –CT showed: RIB FRACTURES ATHELECTASIS HEMOTHORAX NEUMOTHORAX EXAMPLE 5

20
EXAMPLE 6 74 years old man with a known metastatic disease underwent a abdominal -CT. Lower CT showed right lower lobe bronchiectasis and bronchocele

21
68 years old woman with personal history of colon carcinoma Transverse CT througt the lower chest showed a honeycomb pattern characterized by round cyst lesions with a diameter up to 1cm, bunched toguether in grape-like cluster. EXAMPLE 7

22
Abdomen-CT reveal an important number of unsuspected thoracic findings on lower chest. Most of them were major and required further intervention or follow up. Therefore, it`s of almost importance to look through the lower chest systematically and report these findings in order to improve patient care and avoid unnecessary examinations.

23
The goal of our study is to asses the prevalence of chest findings at abdomen-CT and to establish the importance of looking at the chest. It’s important to arrive to a correct diagnosis of an incidental findings and know which of them will require further examinations.

Similar presentations







, FCCP>")









 3.>")
: Principal Modality (2): PET/CT CT Faculty Reviewer:>")



