Download presentation
Presentation is loading. Please wait.

1
Hepatitis C Past, present and future Salil Singh Consultant Gastroenterologist, RBH Salil.Singh@Boltonft.nhs.uk

2
Case presentation? Doctor, sorry to trouble you but do you think I should be tested for hepatitis C?

3
Case presentation? Bilirubin16 (<20) AST54 (<40) ALP97 (<120) Albumin43 (35-50)
 AST54 (<40) ALP97 (<120) Albumin43 (35-50)")
4
Hepatitis - Past Who should be tested for hepatitis C? If the Hep C antibody comes back +ve, what do you do next? What do you tell your patient before referring him to secondary care?

5
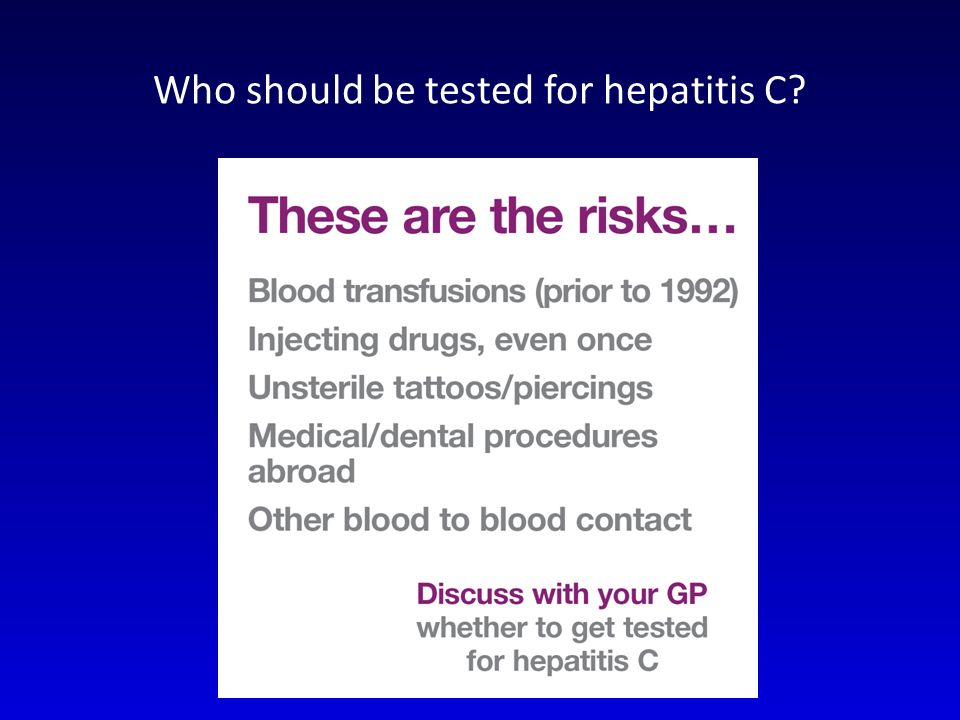
Who should be tested for hepatitis C?

7
Hep C epidemiology

9
200,000 – 500,000 in the UK have Hep C 60,000 – 200,000 will develop liver failure Liver transplant? Long window of opportunity for treatment. Cost effective Hep C epidemiology

10
Keep two stereotypes in mind.

11
If the Hep C antibody comes back +ve, what do you do next? Hep C PCR

12
What do you tell your patient before referring him to secondary care? How did I get this? How long have I had it? Is there a cure? Will I pass it on to anyone? Is this why I get abdominal pain?

13
First consultation (my questions) – Have they got chronic HCV – How long have they had it – Have they got any other liver disease – Have they got aggressive disease – Have they got advanced disease Hepatitis - Present
 – Have they got chronic HCV – How long have they had it – Have they got any other liver disease – Have they got aggressive disease – Have they got advanced disease Hepatitis - Present")
14
First consultation (patient’s questions) – Acquisition / transmission – How long they have had it – Natural history of HCV – Next line of investigations Genotype Routine bloods Abdo USS HIV and Hep B Liver screen Hepatitis - Present
 – Acquisition / transmission – How long they have had it – Natural history of HCV – Next line of investigations Genotype Routine bloods Abdo USS HIV and Hep B Liver screen Hepatitis - Present")
15
Second consultation – Genotype – HIV co-infection – Gender – Age – Weight – Race – Alcohol – Liver biopsy Hepatitis - Present

16
Second consultation – Genotype – HIV co-infection – Gender – Age – Weight – Race – Alcohol – Liver biopsy Hepatitis - Present

17
Second consultation Should we treat with PEG interferon and Ribavarin? – Injections and tablets – Side effects – Efficacy – Family planning – Promise of better drugs Hepatitis - Present

18
GenotypeG1 48 weeks (45%) G3 24 weeks (75%)
 G3 24 weeks (75%)")
19
Second consultation – Genotype – HIV co-infection – Gender – Age – Weight – Race – Alcohol – Liver biopsy Hepatitis - Present

20
GenotypeG1 48 weeks (45%) G3 24 weeks (75%)
 G3 24 weeks (75%)")
21
Hepatitis - Present GenotypeG1 Wait for triple therapy G3 24 weeks (75%)
")
22
Hepatitis - Future Triple therapy adds Boceprevir or telaprevir Licensed Available in Scotland NICE due to rule in 2012 Achieves a clearance of 79% AND reduces the 48 week treatment period down to 24 weeks in those who are PCR –ve at weeks 4+12

23
Triple therapy Telaprevir Standard therapy PEG/Riba Pruritus (SSC)5226 Rash (SSC)5533 Gastrointestinal disorders Nausea3929 Diarrhea2619 Haemorrhoids123 Anorectal discomfort82 Anal pruritus61 Blood and lymphatic system disorders Anaemia (SSC)3215 Hepatitis - Future
5226 Rash (SSC)5533 Gastrointestinal disorders Nausea3929 Diarrhea2619 Haemorrhoids123 Anorectal discomfort82 Anal pruritus61 Blood and lymphatic system disorders Anaemia (SSC)3215 Hepatitis - Future")
24
Triple therapy Telaprevir Standard therapy PEG/Riba Pruritus (SSC)5226 Rash (SSC)5533 Gastrointestinal disorders Nausea3929 Diarrhea2619 Haemorrhoids123 Anorectal discomfort82 Anal pruritus61 Blood and lymphatic system disorders Anaemia (SSC)3215 Hepatitis - Future
5226 Rash (SSC)5533 Gastrointestinal disorders Nausea3929 Diarrhea2619 Haemorrhoids123 Anorectal discomfort82 Anal pruritus61 Blood and lymphatic system disorders Anaemia (SSC)3215 Hepatitis - Future")
25
Both boceprevir and telaprevir have serious and life threatening drug interactions because they are metabolised through a commonly used enzymatic hepatic pathway (CYP3A)
")
26
Summary Hepatitis C is a silent but growing problem We should be screening at risk populations Check HCV PCR We are keen to see HCV patients and may set up a service

27
Glossary Treatment Naive – No previous therapy given Viral load – Amount of RNA in blood expressed as international units/ml SVR – Sustained virological response. Negative PCR at end of treatment and 6 months later. eVR – early virological response. Negative PCR at 4 weeks Combination therapy – PEG interferon and ribavarin Triple therapy – Used for genotype 1 and consists of combination therapy + direct acting antiviral (currently boceprevir and telaprevir) Null responders – Failure to reduce viral load by at least log 10 2 at week 12. Partial responders – Reduced viral load at week 12 but detectable virus at end of treatment Prior relapsers – PCR negative at the end of treatment but detectable at 6 months following treatment completion.
 Null responders – Failure to reduce viral load by at least log 10 2 at week 12. Partial responders – Reduced viral load at week 12 but detectable virus at end of treatment Prior relapsers – PCR negative at the end of treatment but detectable at 6 months following treatment completion..")
Similar presentations




 Associate Professor of Medicine University of Toronto Protease Inhibitors in Chronic Hepatitis C: An Update.>")

 Phase 3 Treatment Experienced Zeuzem S, et al. N Engl.>")













