Download presentation
Presentation is loading. Please wait.

1
The Breast: 2D or not 2D Which test is noblest for the mind of the clinician? (breast cancer detection and diagnosis)
.")
2
Speakers: Dr Denise Powell Dr Marilyn Peers Dr John Branson Dr Bee Kiat Ang Breast Screen Clinical Team To ensure local clinicians have a confident and reliable approach to breast cancer screening and breast cancer diagnosis; To improve the clinicians’ understanding of the role of, and appropriate usage of, newer diagnostic modalities; To encourage the use of the triple test and the role of the GP in clinical assessment; To apply best practice in follow up of the test results. (The test is in, What’s Next?); To engage GPs, Practice Nurses, Radiologist, BreastScreen Staff, Surgeons and Allied Health as a collaborative team; To encourage local research by the collaboration engagement with rural clinical school UQ researchers. OBJECTIVES
; To engage GPs, Practice Nurses, Radiologist, BreastScreen Staff, Surgeons and Allied Health as a collaborative team; To encourage local research by the collaboration engagement with rural clinical school UQ researchers. OBJECTIVES.")
3
AGENDA Welcome – Introduction and Overview – Dr Denise Powell Screening versus diagnostic pathways – How it works in our community; - Dr Marilyn Peers The triple test - why it is the best for you and your patient. 2 local case studies – Breast Screen clinical team Screening and diagnostic imaging modalities - what is best for the presenting situation; Dr John Branson Use of mammography and ultrasound (2D);
;.")
4
AGENDA The role of newer modalities such as MRI and Tomography (3D) The breast surgeon in Bundaberg and their role in the Multidisciplinary Team in Brisbane. Breast Surgeon 2 local case studies – Dr John Branson The optimal request for Breast Imaging and pathology Identification of local issues with collaborative problem solving Anyone for research? Evaluation & Close.

5
Breast Screen Qld Program Cancer Screening Service for Women Free High Quality

6
Aims Reduce morbidity and mortality Cost effective Accessible

7
Comprehensive and continuous quality improvement system Clearly defined national and state standards of best practice

8
Directed at Asymptomatic women Target age group 50-74 years

9
Why this target group? Incidence of breast cancer is high Screening mammography is effective in reducing mortality

10
Mortality Incidence 0 20 40 60 80 100 120 Rate per 100,000 Women 19831985198719891991199319951997199920012003 Year Incidence and mortality trends Rate per 100,000 Women

11
Years after diagnosis

12
Early detection saves lives

13
Screening Cycle 2 yearly other than where there is Past history of breast cancer Past history of ADH, LCIS, ALH A strong FH of breast cancer (defined as 1 o rel < 50)
")
14
Catchment Area Miriamvale to Wondai North, Central and South Burnett (Bundaberg, Hervey Bay and Maryborough)
")
15
Participation Rates 2012/13 Agnes Water/ Miriam Vale54.4% Ashfield/ Kepnock72.7% Bargara/ Burnett Heads49.7% Branyan/ Kensington55.4% Bundaberg68.7% Bundaberg East66.7% Bundaberg North60% Bundaberg Region (North)48.8% Bundaberg South59.5% Milbank/ Avoca65.7% Svensson Heights/ Norville66.8% Walkervale/ Avenell Heights65.4%
48.8% Bundaberg South59.5% Milbank/ Avoca65.7% Svensson Heights/ Norville66.8% Walkervale/ Avenell Heights65.4%")
16
THE DIAGNOSTIC ROUTE

17
The triple test History and examination Imaging - mammogram &/or ultrasound Non-excision biopsy - FNAC &/or core biopsy The triple test is positive if any component is indeterminate, suspicious or malignant

18
For a triple test to be negative ALL three components: Clinical breast examination Medical Imaging Biopsy must be benign or normal

20
What do we know? >50% breast cancers found because of a breast change GP is the first port of call GP initiates the triple test by performing a clinical examination and ordering appropriate imaging

21
The triple test Completion of the triple test is multidisciplinary: GP Radiologist Pathologist Surgeon

22
The triple test The key is the review of all results and correlation with the presenting symptom One clinician must take responsibility What is your referral pathway?

23
Breast Imaging 101 There really are 50 shades of grey Mammography---positions—MLO and CC

26
Breast Imaging Continued Compression Radiation Exposure Ultrasound ---screening vs diagnostic Accreditation

27
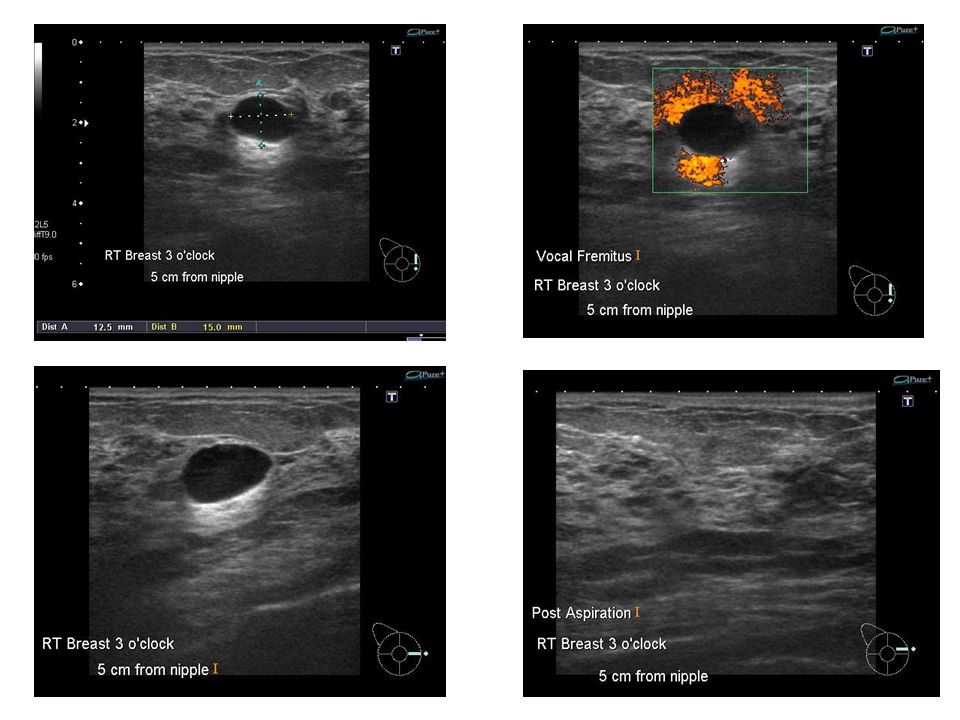
Case 1 Michele, 28-year-old dental nurse Long history of premenstrual mastalgia and nodularity of breasts Noticed new lump in right breast 1 month ago which did not resolve with menses No family history No medications

28
On examination: Bilateral nodularity of breasts especially outer quadrants More defined lump lower lateral quadrant on the right

29
Differential diagnosis of a lump in a young woman Nodule of normal breast tissue Fibroadenoma Abscess/fat necrosis Simple cyst Breast cancer

30
Breast imaging Women with breast symptoms must be referred for diagnostic assessment not to breast screening services Women < 35 years: ultrasound is the initial imaging modality

33
CASE 1

34
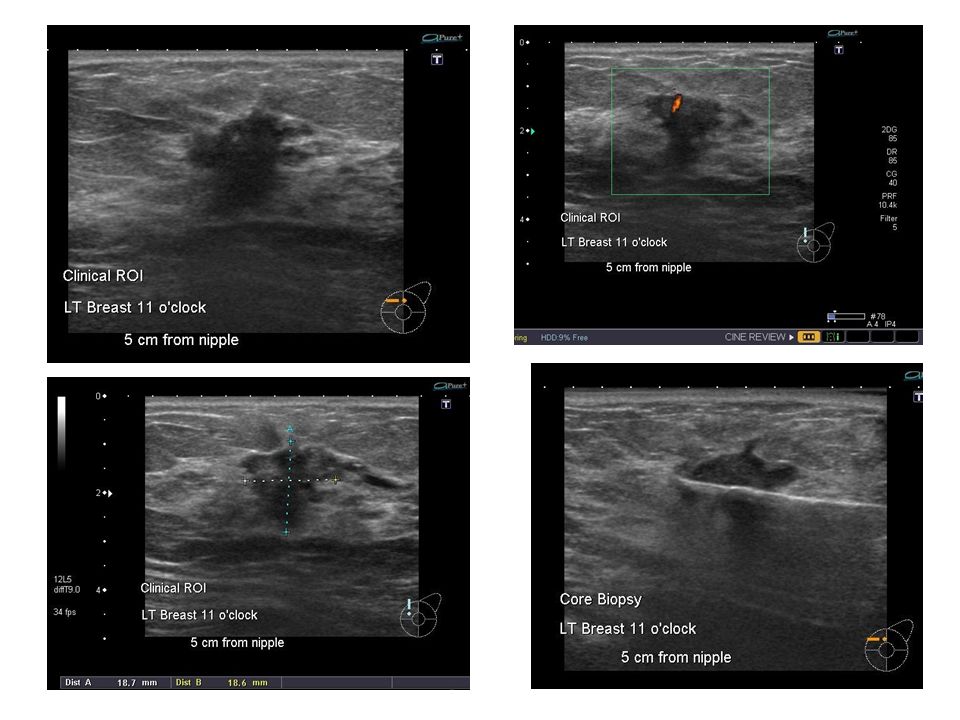
A palpable lump, seen as a solid lesion on breast ultrasound requires non- excisional biopsy (FNAC or core biopsy) to confirm pathology
 to confirm pathology")
35
Case 2 Denise is a 51-year-old dairy farmer Attends for regular pap smear On breast examination you detect a small thickening Denise is peri menopausal with very irregular menses and some hot flushes She is not taking HRT

39
Context Regional Queensland Primary referrers Opinions are strictly personal (agnostic private/public)
")
40
Local availability – mammography and US the mainstay Generally 2D technology In general, more specialised technology would require referral to a specialised imaging centre. Breast MRI best performed in a centre where there is a critical mass of referrers and patients and significant body of expertise. Local exceptions – 3D imaging

41
Mammography Evolution o Film screen mammography o Digital – CR and DR Ultrasound (US) o Generally refers to hand held US performed by a sonographer o Hand held US is not appropriate for screening o Automated US (ABUS or AWBUS) is an appropriate for initial screening of mammographically dense breasts.
 o Generally refers to hand held US performed by a sonographer o Hand held US is not appropriate for screening o Automated US (ABUS or AWBUS) is an appropriate for initial screening of mammographically dense breasts.")
42
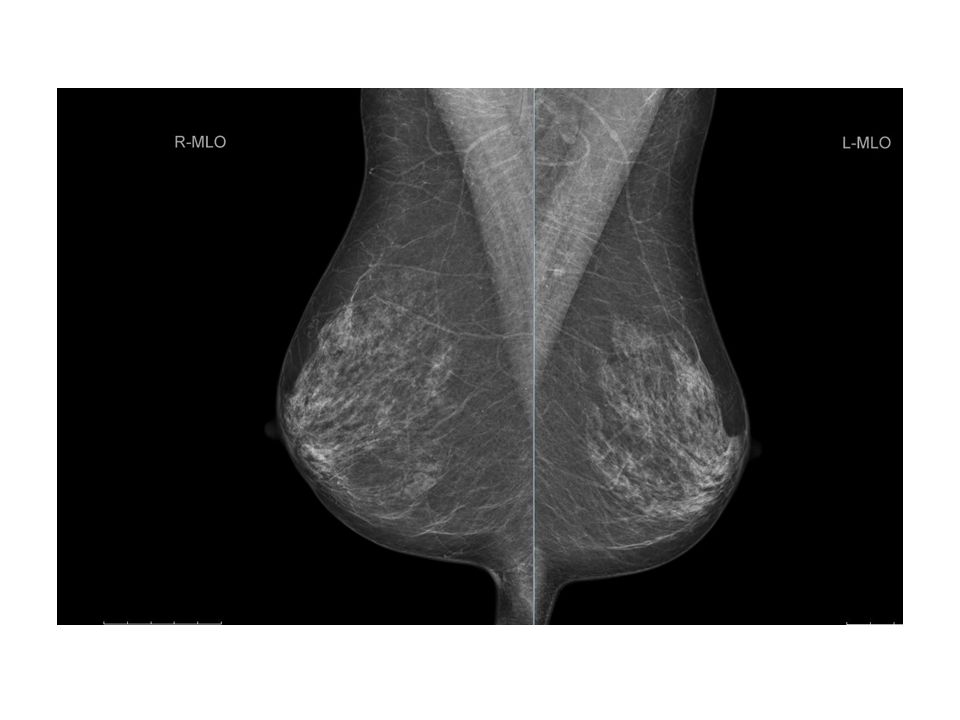
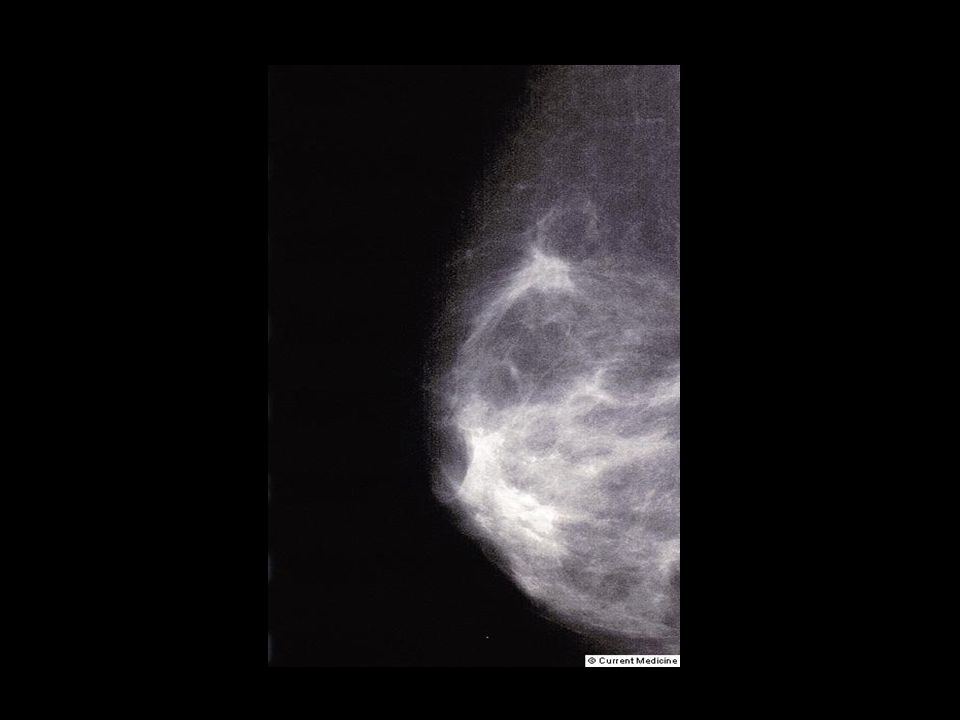
Looking at the mammogram. Four broad groups of appearances of the breast 1.predominantly fatty (less than 25% glandular tissue) - approximately 10 % of population 2.scattered fibroglandular density (25 – 50% glandular tissue) -approximately 40% of population 3.heterogeneous density (50 – 75% glandular tissue) - approximately 40 % of population 4.extremely dense (more than 75% glandular tissue) - approximately 10% of population
 - approximately 10 % of population 2.scattered fibroglandular density (25 – 50% glandular tissue) -approximately 40% of population 3.heterogeneous density (50 – 75% glandular tissue) - approximately 40 % of population 4.extremely dense (more than 75% glandular tissue) - approximately 10% of population.")
43
Figure a: Mediolateral oblique mammographic views demonstrate the four BI-RADS breast density categories. (a) Almost entirely fatty.
 Almost entirely fatty..")
44
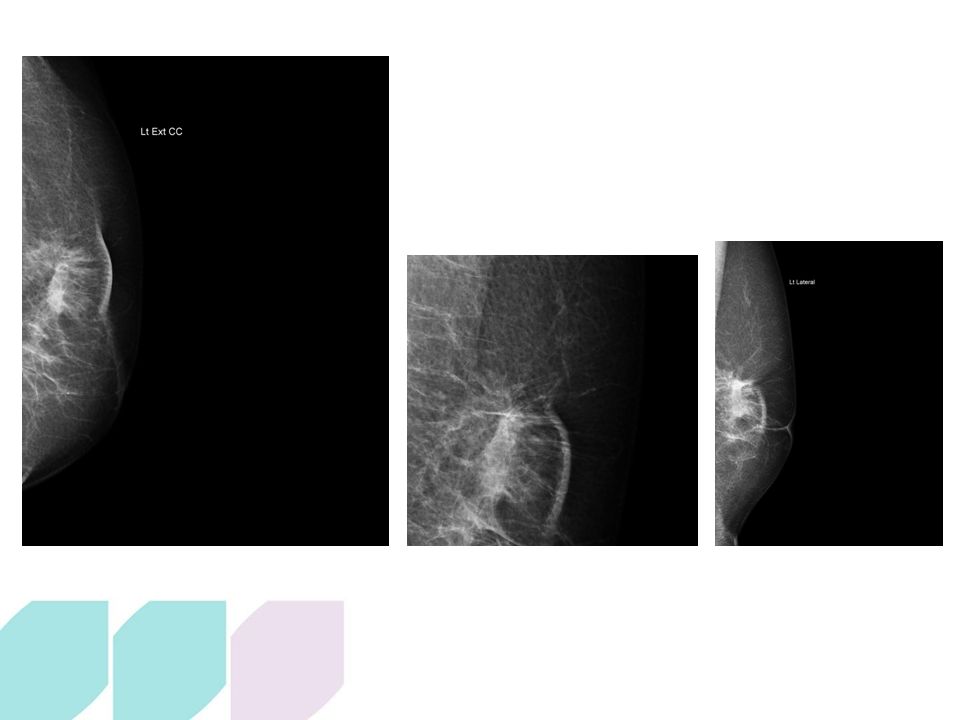
Figure b: Mediolateral oblique mammographic views demonstrate the four BI- RADS breast density categories. (b) Scattered fibroglandular density.
 Scattered fibroglandular density..")
45
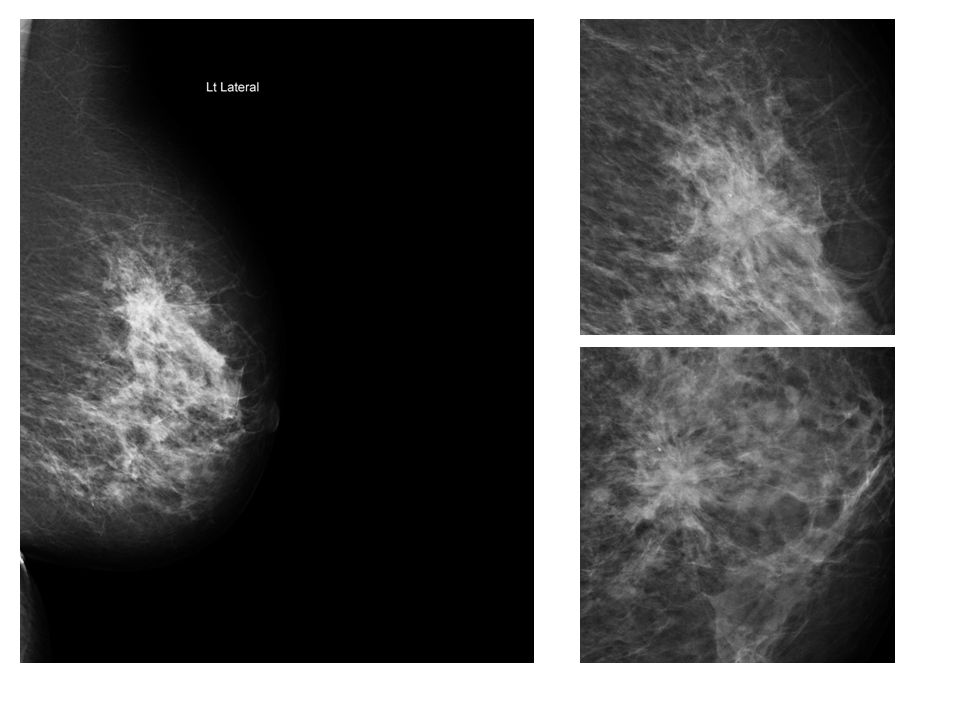
Figure c: Mediolateral oblique mammographic views demonstrate the four BI-RADS breast density categories. (c) Heterogeneously dense, which may obscure detection of small masses.
 Heterogeneously dense, which may obscure detection of small masses..")
46
Figure d: Mediolateral oblique mammographic views demonstrate the four BI- RADS breast density categories. (d) Extremely dense, which lowers the sensitivity of mammography.
 Extremely dense, which lowers the sensitivity of mammography..")
47
Mammographic sensitivity decreases as breast density increases o varying sensitivities quoted eg. Fatty breast sensitivity up to 97%, down to sensitivity varying from 30% – 48% for dense breasts

48
Analysis of mammographic findings. Primary finding o Mass (definition) - margins, density o Non-specific density (focal asymmetry on one view) o Architectural distortion (radiating lines) o Calcifications - varying forms density and distribution patterns o Combinations of the above Ancillary findings o Additional findings relating to skin (thickening, retraction), nipple retraction, lymph nodes, general breast density Methods to help further analysis of findings (additional mammographic views) o Coned (spot) compression o Magnification o Additional special views for different areas of the breast
 - margins, density o Non-specific density (focal asymmetry on one view) o Architectural distortion (radiating lines) o Calcifications - varying forms density and distribution patterns o Combinations of the above Ancillary findings o Additional findings relating to skin (thickening, retraction), nipple retraction, lymph nodes, general breast density Methods to help further analysis of findings (additional mammographic views) o Coned (spot) compression o Magnification o Additional special views for different areas of the breast.")
49
What is BI-RADS ? o United States system (Breast Imaging Reporting And Data System) o Not universally used in Australia o Roughly equivalent to the widely used 1 – 5 category 1. No significant abnormality= BI-RADS 1 2. Benign= BI-RADS 2 3. Equivocal = BI-RADS 3 4. Suspicious = BI-RADS 4 5. Malignant= BI-RADS 5
 o Not universally used in Australia o Roughly equivalent to the widely used 1 – 5 category 1. No significant abnormality= BI-RADS 1 2. Benign= BI-RADS 2 3. Equivocal = BI-RADS 3 4. Suspicious = BI-RADS 4 5. Malignant= BI-RADS 5.")
50
Referring for breast imaging Screening o Private o Public (BreastScreen) o Mammography is the mainstay and starting point o US (hand held) is not recommended for screening purposes. - how to deal with “mammography is too painful” ? o Reasons US screening is a bad idea - (false positives, false negatives, unnecessary biopsy ie over-diagnosis) therefore US is best targeted in relation to positive clinical and mammographic findings. o Exception (ABUS, AWBUS) – has significant potential as a screening tool for dense breasts, would act as guide to further targeted hand held US. o Timing – not before the big overseas holiday!
 therefore US is best targeted in relation to positive clinical and mammographic findings. o Exception (ABUS, AWBUS) – has significant potential as a screening tool for dense breasts, would act as guide to further targeted hand held US. o Timing – not before the big overseas holiday!.")
51
Fig. 2B Fig. 2B—42-year-old woman with biopsy-proven cancer of right breast. B, Handheld ultrasound image of left breast shows subtle mixed hyperechoic-hypoechoic lesions with suspicious echogenic foci (arrows).
..")
52
Fig. 2C Fig. 2C—42-year-old woman with biopsy-proven cancer of right breast. C, Automated ultrasound image of left breast shows subtle localized areas of heterogeneous echogenicity (arrows) without definite associated mass in upper outer quadrant that were not detected by any of five readers. Surgery confirmed presence of 3.0-cm ductal carcinoma in situ, micropapillary pattern.
 without definite associated mass in upper outer quadrant that were not detected by any of five readers. Surgery confirmed presence of 3.0-cm ductal carcinoma in situ, micropapillary pattern..")
53
Fig. A Fig. A, Handheld ultrasound image shows irregularly shaped hypoechoic mass with microlobulated margin (arrows) adjacent to biopsy-proven malignant mass (circle) in upper outer quadrant of left breast.
 adjacent to biopsy-proven malignant mass (circle) in upper outer quadrant of left breast..")
54
Fig. 3B Fig. 3B—44-year-old woman with breast cancer. B, Automated ultrasound image shows malignant- looking mass (arrows) adjacent to biopsy-proven malignant mass (circle), which was not detected by one reader. Surgery confirmed two foci of invasive ductal carcinoma.
 adjacent to biopsy-proven malignant mass (circle), which was not detected by one reader. Surgery confirmed two foci of invasive ductal carcinoma..")
55
Referring for diagnostic breast imaging o Cannot over emphasise the importance of clinical history and findings on CBE: this ties in with the TRIPLE TEST - the radiology request form should reflect history and CBE o In general, mammography is discouraged below age 40 - radiation dose, special exceptions exist o In general, in the young age group, US is the primary diagnostic modality o US is most useful when targeted to clinical and/or mammogram findings o Remember, significant pathology including malignancy can be occult on both mammography and US on occasions. Hence the importance of history and CBE findings Further referral for additional tests (eg biopsy, MRI etc) – generally in consultation with radiologist, surgeon, oncologist etc
 – generally in consultation with radiologist, surgeon, oncologist etc.")
56
Special situations for referral Nipple discharge o History, CBE are vital o Bilateral multiductal – benign, yellow-brownish discharge o Uniductal – suggests significant underlying disease (eg papilloma) - especially concerning if spontaneous and sustained - both blood stained and clear (`chardonnay’ ) can be associated with underlying focal pathology o US initial modality of choice, usually in conjunction with mammogram o if positive, surgical referral for possibility microdochectomy -(ductogram virtually obsolete) Saline implants o Generally clinical diagnosis (collapses) o +/- US
 - especially concerning if spontaneous and sustained - both blood stained and clear (`chardonnay’ ) can be associated with underlying focal pathology o US initial modality of choice, usually in conjunction with mammogram o if positive, surgical referral for possibility microdochectomy -(ductogram virtually obsolete) Saline implants o Generally clinical diagnosis (collapses) o +/- US")
57
Silicone implants o Mammography for both symptomatic and screening purposes, includes implant exclusion views o US – ancillary, for assessment of masses etc - less reliable than MRI for implant rupture o MRI – best detail for suspected implant rupture Lactation / infection o US o Beware older woman with red inflamed breast, possibility of inflammatory carcinoma. In the latter case needs mammography as well as US Post cancer treatment surveillance o annual mammography o usually US as well, helps in assessing possible recurrence Cosmetic surgery o Generally surgeon’s call, depends on nature of surgery

58
Looking in 3D at the breast Some practical points about MRI o cost o needs IV contrast (renal function etc) o position – must lie prone for 30 – 45 minutes (? Sedation, obesity) o timing - to be done on days 7 – 14 after LMP o not a mammogram substitute nor a panacea o Has high sensitivity but moderate specificity - very important that MRI be interpreted using full correlation with preceding breast imaging such as mammography and US, plus all relevant clinical details o Contra-indicated in some patients (claustrophobia / metal ) o Findings on MRI may lead to additional investigation, particularly “second look” US or further biopsy including MRI – guided biopsy
 o timing - to be done on days 7 – 14 after LMP o not a mammogram substitute nor a panacea o Has high sensitivity but moderate specificity - very important that MRI be interpreted using full correlation with preceding breast imaging such as mammography and US, plus all relevant clinical details o Contra-indicated in some patients (claustrophobia / metal ) o Findings on MRI may lead to additional investigation, particularly second look US or further biopsy including MRI – guided biopsy.")
59
Where MRI is particularly useful o High risk screening in young women - eg BRCA1 and BRCA2, plus other genetic predispositions - eg young women who had RT to the chest at a young age (Hodgkin’s Disease) o Note: MRI is not considered cost effective for the screening of young women who are at average risk of breast cancer o Newly diagnosed breast cancer - Most accurate way of assessing chest wall involvement - Assessing extent of disease, including additional foci of disease in the ipsilateral or contralateral breast - Large malignant tumours - Lobular carcinoma histology o Silicone implants – non contrast - Not saline (clinical) o Differentiating scar versus recurrent cancer when mammography and US are inconclusive, and biopsy is contraindicated o Metastatic breast cancer where the search for the unknown primary breast lesion on mammography and US has proved negative o Evaluating response to NAT
 o Note: MRI is not considered cost effective for the screening of young women who are at average risk of breast cancer o Newly diagnosed breast cancer - Most accurate way of assessing chest wall involvement - Assessing extent of disease, including additional foci of disease in the ipsilateral or contralateral breast - Large malignant tumours - Lobular carcinoma histology o Silicone implants – non contrast - Not saline (clinical) o Differentiating scar versus recurrent cancer when mammography and US are inconclusive, and biopsy is contraindicated o Metastatic breast cancer where the search for the unknown primary breast lesion on mammography and US has proved negative o Evaluating response to NAT")
60
The breast density problem o Dense breasts (more than 50% glandular tissue) are a challenge on mammography due to decreased sensitivity o Newer technologies attempt to address this – MRI; 3D US; Tomosynthesis o Not only a problem for radiologists and the patient, but even politicians have become involved
 are a challenge on mammography due to decreased sensitivity o Newer technologies attempt to address this – MRI; 3D US; Tomosynthesis o Not only a problem for radiologists and the patient, but even politicians have become involved")
61
January 13, 2015 – Gov. John Kasich has signed Ohio’s breast density notification bill into law, making the state the 20 th in the U.S. to enact such legislation. Effective march 2015, the law (HB 394, section 3702.40) requires that mammography facilities send to each patient a summary of the mammography report containing the results of the patient’s mammogram. If the patient has dense breast tissue, it requires that the report include the following statement: Your mammogram demonstrates that you have dense breast tissue, which could hide abnormalities. Dense breast tissue, in and of itself, is a relatively common condition. Therefore, this information is not provided to cause undue concern; rather, it is to raise your awareness and promote discussion with your healthcare provider regarding the presence of dense breast tissue in addition to other risk factors.
 requires that mammography facilities send to each patient a summary of the mammography report containing the results of the patient’s mammogram. If the patient has dense breast tissue, it requires that the report include the following statement: Your mammogram demonstrates that you have dense breast tissue, which could hide abnormalities. Dense breast tissue, in and of itself, is a relatively common condition. Therefore, this information is not provided to cause undue concern; rather, it is to raise your awareness and promote discussion with your healthcare provider regarding the presence of dense breast tissue in addition to other risk factors..")
62
What is Breast Tomosynthesis? Digital breast tomosynthesis (DBT) o 3D mammography o Digital era mammography with an old twist o Compressed breast static, X-ray tube moves in a short arc to acquire series of low dose images at a number of points (eg 15 images), then acquires a standard 2D image o Both views (MLO and CC) o Reconstruction 3D images plus standard 2D image o Images to demonstrate the above
 o 3D mammography o Digital era mammography with an old twist o Compressed breast static, X-ray tube moves in a short arc to acquire series of low dose images at a number of points (eg 15 images), then acquires a standard 2D image o Both views (MLO and CC) o Reconstruction 3D images plus standard 2D image o Images to demonstrate the above.")
63
How Hologic 3D mammography works X-ray tube moves in an arc across the breast Series of low dose images acquired from different angles Dose equivalent to one 2D mammogram 1 Projection images reconstructed into 1 mm slices Compression paddle Compressed breast Detector housing Reconstructed slices { X-ray tube arc of motion

64
In 2D Digital Mammography: Tissue superimposition hides pathologies in 2D Tissue superimposition mimics pathologies in 2D

65
Breast Tomosynthesis Improves Visibility by Reducing Tissue Superimposition

66
A Solution Is Hologic Tomosynthesis Tomosynthesis minimizes the effects of structure overlap within the breast

67
Fig. 3A Fig. 3A —74-year-old woman. Examination was retrospectively reviewed by three radiologists who stated they would have recalled woman without availability of tomosynthesis, and she was actually not recalled for diagnostic workup during clinical interpretation. She remained negative during subsequent examination 1 year later. A, Digital mammography images (A and B) demonstrate a suspicious area as shown by the arrow (A). Tomosynthesis images (C—E) show three widely spaced images from the tomosynthesis image set. Tomosynthesis images show that structures at different levels in breast can summate to create suspicious region on digital mammography image that may be identified as negative or superimposed tissue on tomosynthesis images.
 demonstrate a suspicious area as shown by the arrow (A). Tomosynthesis images (C—E) show three widely spaced images from the tomosynthesis image set. Tomosynthesis images show that structures at different levels in breast can summate to create suspicious region on digital mammography image that may be identified as negative or superimposed tissue on tomosynthesis images..")
68
Fig. 3C

69
Fig. 3D

70
Fig. 3E

71
RCC 2D

72
RCC 2D 3D February 2011

73
Slice 10 20 30 40 February 2011

74
Digital Mammo (2D) Tomo Slice (3D) Improved Sensitivity - Tubulolobular Adenocarcinoma
 Tomo Slice (3D) Improved Sensitivity - Tubulolobular Adenocarcinoma")
75
2D3D Tomosynthesis Improved Sensitivity – Invasive Ductal Carcinoma

76
Recall Reduction – Superimposed Tissue

77
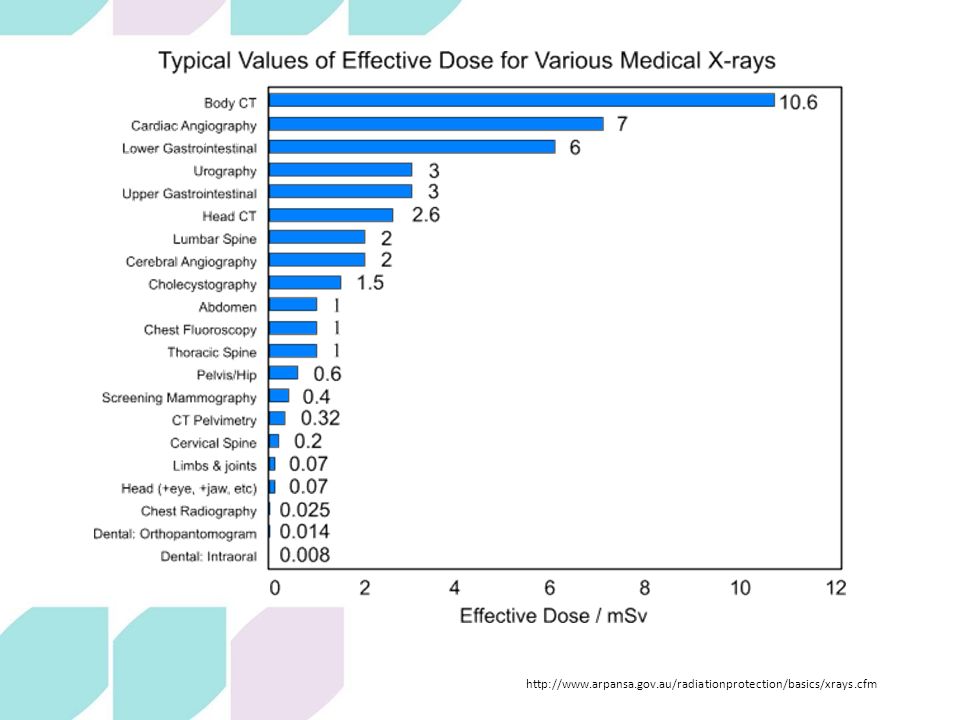
Advantages of 3D mammography – increased specificity and sensitivity o Particularly helpful in the dense breast o In all breasts leads to decreased “summation effect” (“composite shadowing” or “superimposition of normal tissue”) o Increased delineation of masses, architectural distortions and asymmetries o Screening – decreased recall rates, increased cancer detection o Diagnostic and assessment settings – fewer additional mammographic views increased pre-test probability for the subsequent US o Decreased false positives and decreased biopsy rates o Improved detection of lobular carcinoma (anecdotal only, several sources) Radiation dose Combined 2D and 3D mammography dose is approximately half of annual Australian background dose. (CTPA 7 x) See tables
 See tables.")
78
Comparison of Doses MQSA Limit

79
Patient Radiation Dose *Based on the U.S. average dose of FFDM, S/F and CR as collected from medical physicist’s’ dose measurements available at the time of MQSA inspections Jan – Sept 2012. mGy

80
Comparison of Doses http://www.arpansa.gov.au

81
http://www.arpansa.gov.au/radiationprotection/basics/xrays.cfm
82
Two case studies, both presented for screening mammography 55 year old female o See images

87
2 nd Case study, both presented for screening mammography 66 year old female o See images

95
o Medicare Local staff: Kaylene McShane & Vivien Clift for invitations & catering o UQ for the use of their wonderful facilities o All BreastScreen Qld Wide Bay Staff, with particular thanks to Di Dingle, Julie Nelson, Dan Smith and Veronica Edwards for technical help o Gabrielle Vaughan (Hologic Australia) o American Roentgen Ray Society (Images) Acknowledgements
 o American Roentgen Ray Society (Images) Acknowledgements")
Similar presentations