Download presentation
Presentation is loading. Please wait.

1
SRS/SRT AUDIT Dr Sarah Pascoe Neuro-Oncology Study Day 8 th June 2007

2
STEREOTACTIC RADIOSURGERY First introduced by Leksell in 1951 Single high dose photon irradiation – intracranial treatment Initially 300kV XR beams Late 1960s – first gamma-knife – collimated Co-60 beams

3
STEREOTACTIC RADIOSURGERY Benefits: Precise, highly conformal treatment Dose escalation ‘Inoperable’ lesions Single treatment which may be repeated

4
CO-ORDINATE SYSTEM X YZ

5
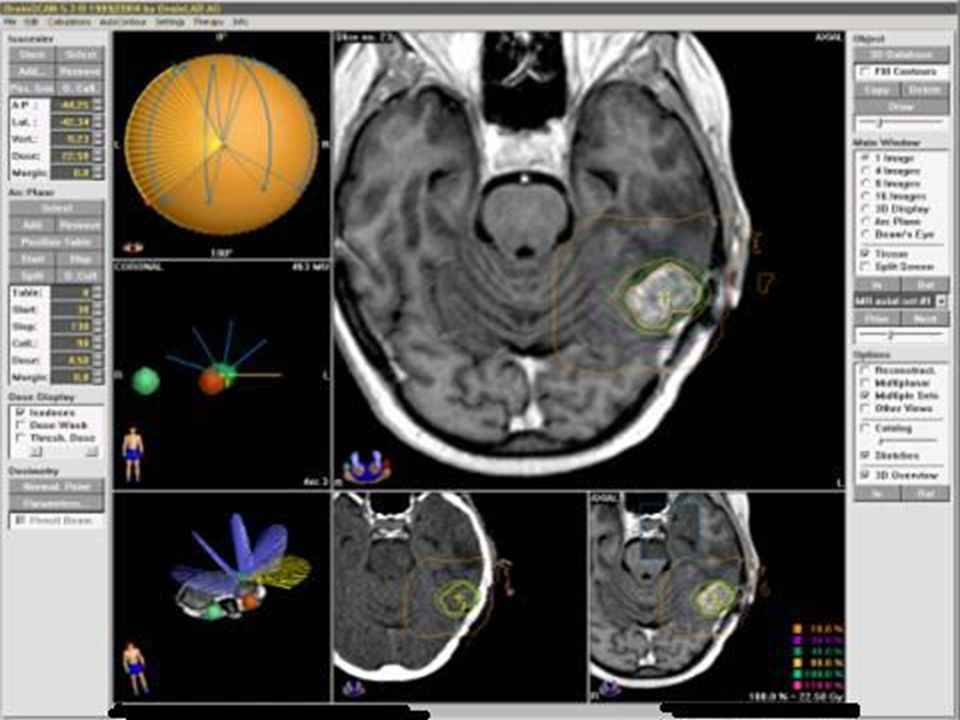
STEREOTACTIC IMMOBILISATION BrainLAB stereotactic headring for SRS and functional cases BrainLAB mask system for fractionated SRT treatments and frameless radiosurgery Head and neck fixation system for fractionated SRT treatment to T1

6
STEREOTACTIC RADIOSURGERY

7
WHAT IS SRS? Multiple Isocentre Circular BeamsSingle Isocentre Shaped Beams Conformal Shaped BeamTraditional Radiosurgery Lesion Radiation Critical Organs

8
Clinical Procedure WHAT IS SRS? Patient fixation Imaging Planning m3 Treatment Set-Up Patient Treatment Completed 90 min. 20 min. 30 min. 60 min. Start 20 min.

9
STEREOTACTIC RADIOSURGERY

10
SRS/SRT AUDIT Started treating patients 5/2005 Two year data 110 patients referred 40 male, 70 female 85 treated to date

11
POSTCODES PL - 46 EX - 26 TR - 14 TQ - 20 BH - 2 SA - 1 No PC - 1

12
INDICATIONS Acoustic neuromas AVMs/haemangioblastomas Gliomas – re-treat Meningiomas Metastases Pituitary tumours/craniopharyngiomas

13
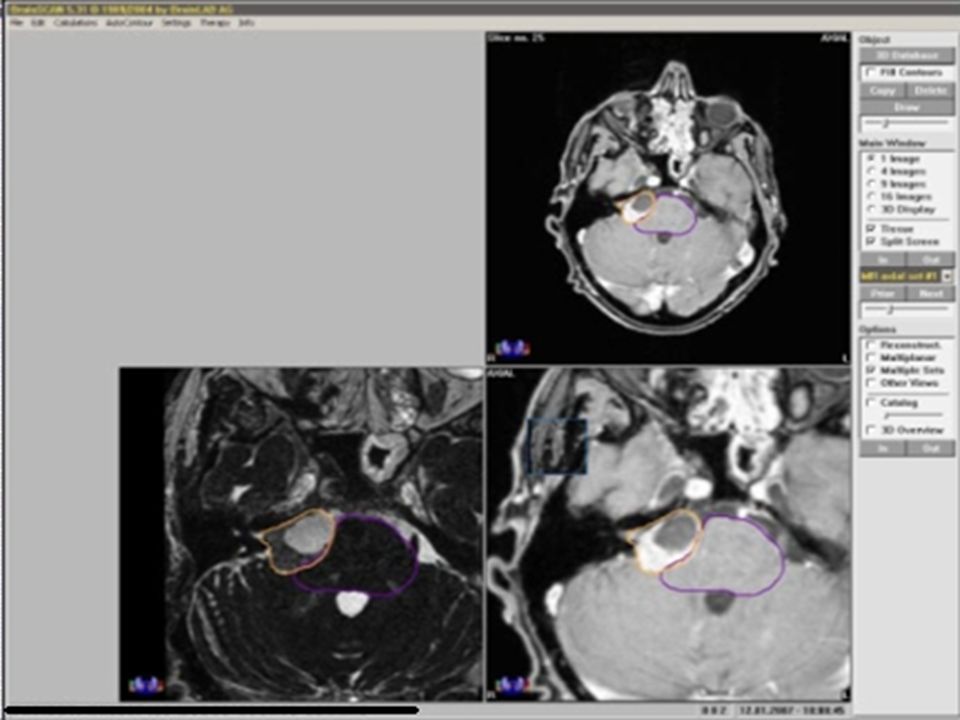
ACOUSTIC NEUROMAS 27 patients referred 21 treated 12 male, 15 female Single fraction – 16 Fractionated treatment – SRT – 5

14
ACOUSTIC NEUROMAS All single fractions – 12 Gy to encompassing isodose – 89% 13.5 Gy to isocentre All fractionated regimes – 7x4 Gy to E.I, 7x5 Gy to isocentre

15
ACOUSTIC NEUROMAS Thirteen pts – 6 month FU Seven larger – 109-284% original volume Eleven pts – 12 month FU Four larger – 110-236% One pt – 18 month FU Larger by 120%

16
ACOUSTIC NEUROMAS Mo major morbidity – severe nausea/vomiting – resolved with steroids No definitive hearing assessments as yet No new facial weakness

17
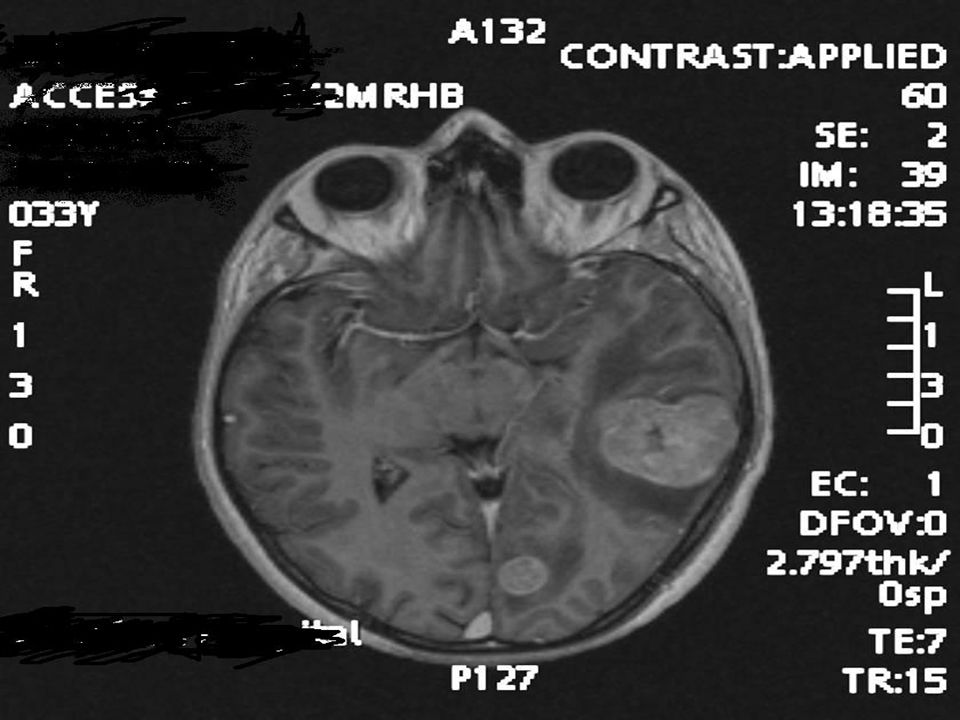
MR x. Presented 1999 – headaches, right- sided hearing loss, right-sided facial numbness and tingling MRI showed right sided acoustic neuroma No change over period 1999-2004

18
MR x MRI 6/06 – enlargement of right sided tumour ( GTV > 4 cm3 – brain stem OAR) Stable neurology SRT started 1/07
 Stable neurology SRT started 1/07")
20
AVMs 16 patients referred – 8 male, 8 female 10 treated to date Single fraction – 9 patients – 18-20Gy to E.I. One fractionated course of treatment, larger AVM, young girl

21
AVMs 3 patients – 6 month FU All lesions are smaller 40-65% of original volume No immediate morbidity except hair loss Obliteration unlikely until 2-3 years post SRS/SRT

23
MENINGIOMAS 24 patients referred 17 female, 7 male 19 treated – 3 referred to RMH, 2 waiting for treatment

24
MENINGIOMAS 15 single fractions – 12 – (14) Gy to E.I. 4 fractionated – 7x4 Gy to E.I. One conventional fractionation – optic nerve tumour – 28x1.8 Gy fractions

25
MENINGIOMAS Eleven – 6 month FU Three increased in size – 141-155% Eight smaller – 10-88% of original volume Six – 12 month FU – all same size/smaller than original volume

28
MENINGIOMAS Hemiparesis, required high dose steroids post treatment Deterioration in visual acuity ?resolved Post SRS haemorrhage

29
JUNE CARTER

30
MISCELLANEOUS 2 adenocystic tumour recurrences 1 HGG 1 NF1 patient 1 occipital fibrosarcoma recurrence

31
MISCELLANEOUS 1 oligodendroglioma 3 pituitary tumours/craniopharyngiomas – move toward SRT as standard treatment 1 recurrent germinoma – in CR

32
VASCULAR Two haemangioblastomas – both female, one required admission soon after SRS – high dose steroids, remains dysphasic One cavernoma referred – no clear evidence base for SRS – not treated

33
METASTASES 23 patients 15 female, 8 male 27 fractions – all single fractions, 4 patients treated on two separate occasions Aged 29 – 75 – mean age 55

34
METASTASES Lung – 8 Melanoma – 5 Bladder/renal – 4 Breast – 3 Thyroid – 1 Ovarian – 1 NET – 1

35
SELECTION CRITERIA 1-3 intracranial metastases – MRI, WBRT not necessarily needed/CI Good PS Controlled systemic disease

36
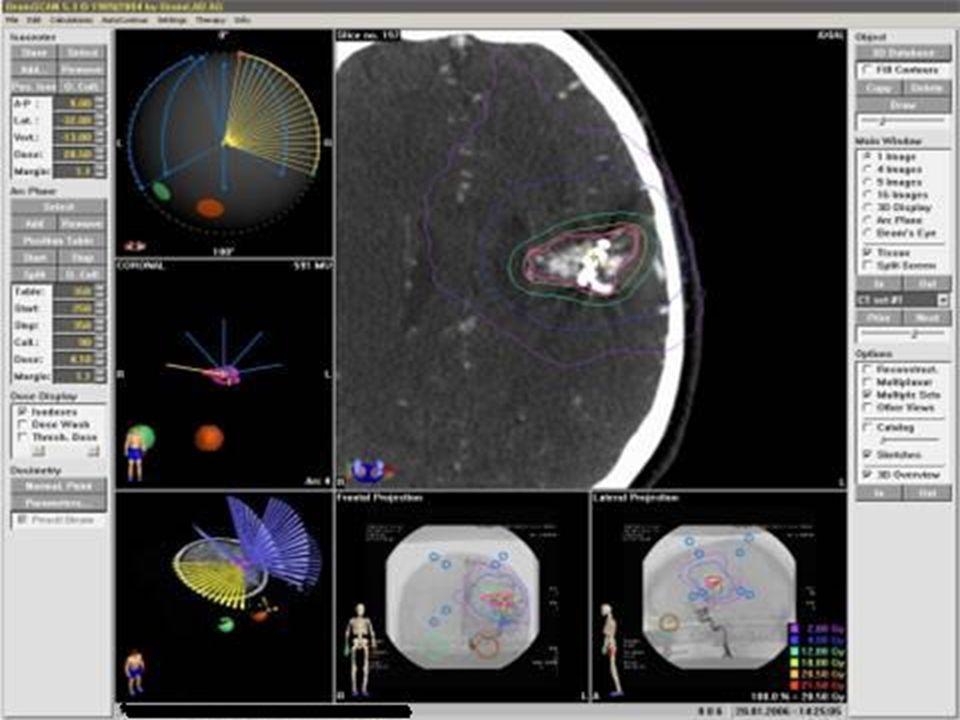
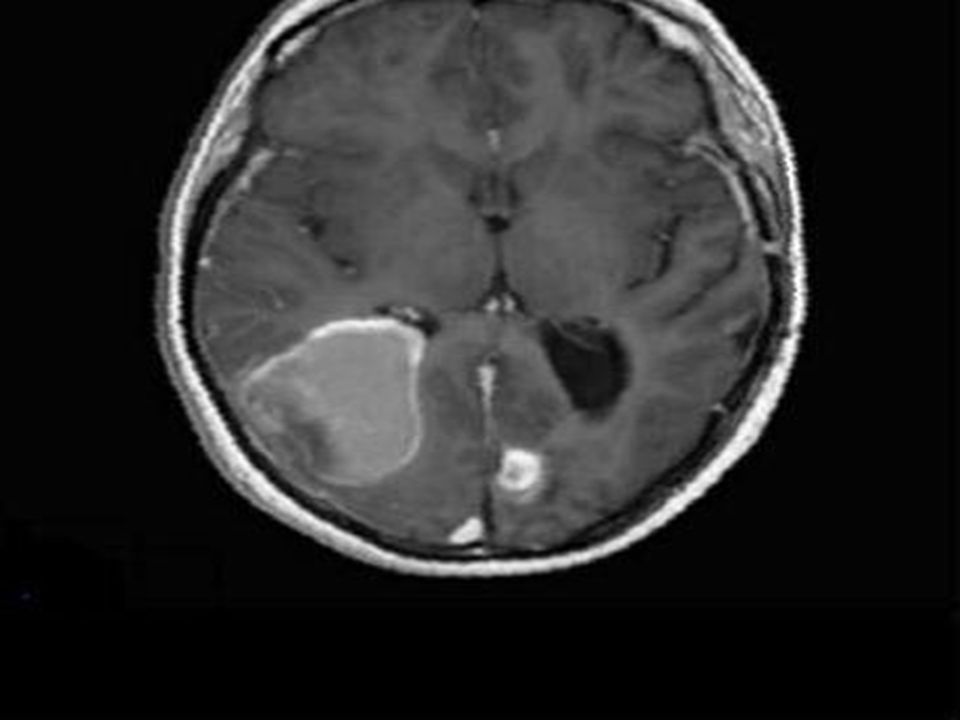
MISS W. 33 year old Melanoma – diagnosed 1997 Presented – grand mal seizure MRI – two metastases left cerebral hemisphere Systemic CT - NAD

37
MISS W. 8/05 – larger lesion excised Histology confirmed metastatic melanoma Left occipital lesion and tumour bed – SRS – 9/05

40
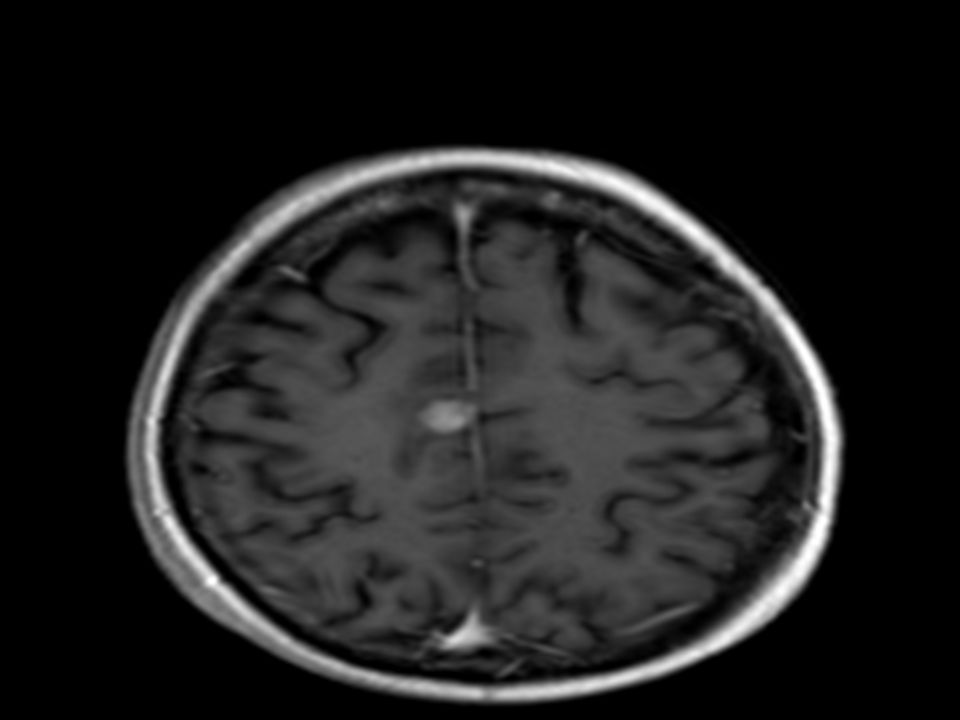
6 Months8 Months 0 Months 3 Months

41
MISS W. Developed further metastasis 6/06 – right occipital region – further SRS 6/06 Admitted via A/E – GCS 7 MRI – extensive oedema/haemorrhage/midline shift Required mannitol/high dose steroids

43
MISS W. Latest imaging – 12/06, stable intracranial disease, no new lesions – now 20/12 post first fraction Multiple subcutaneous nodules Has declined further imaging/systemic treatment

44
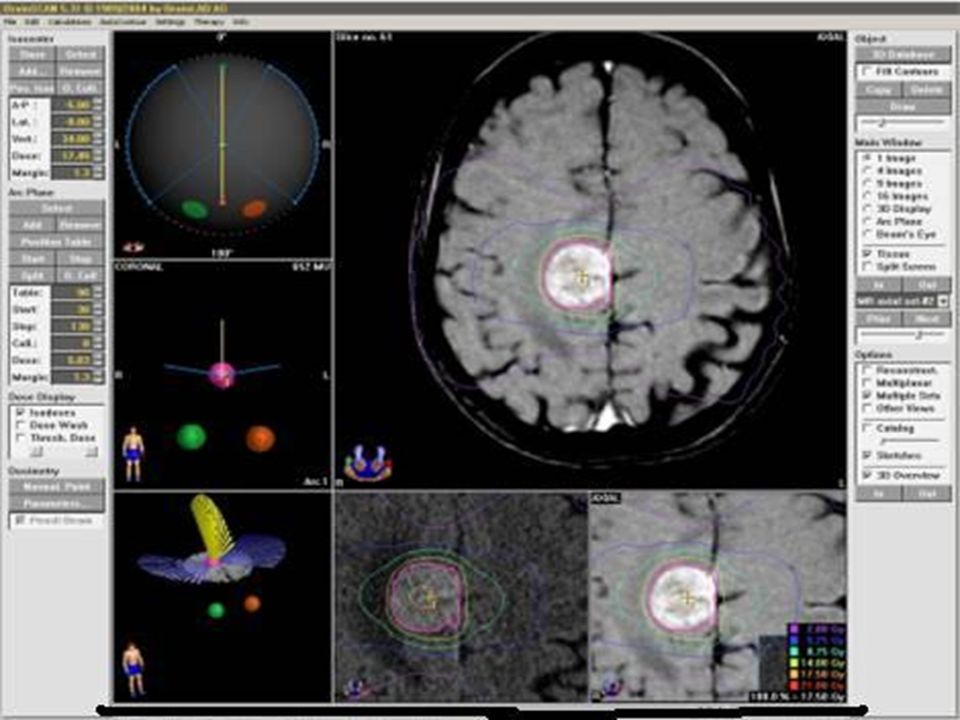
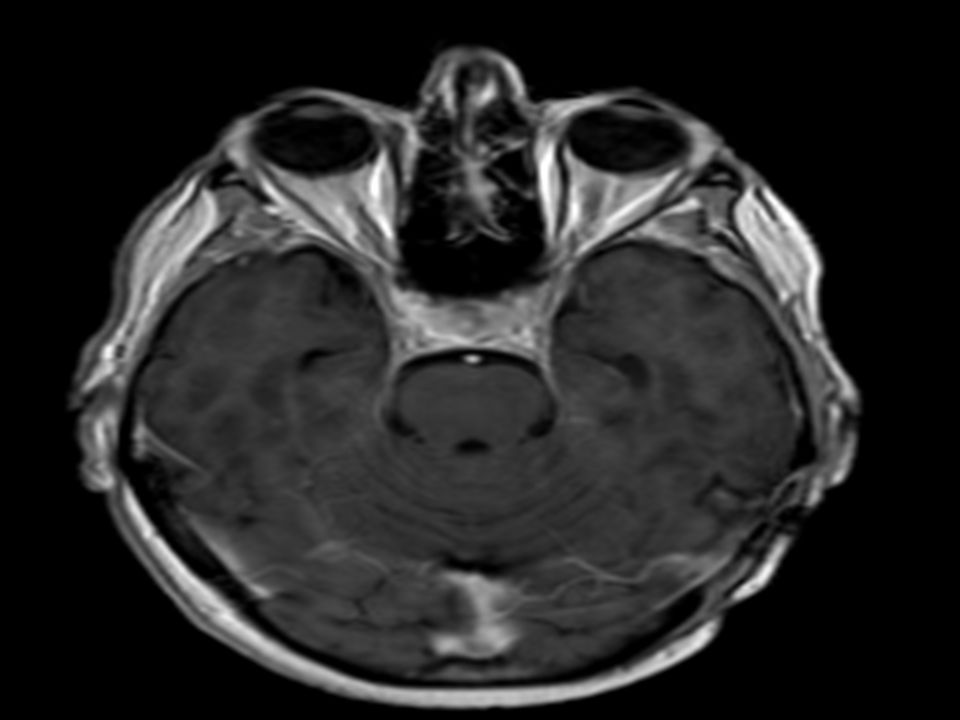
MRS Y Diagnosed with metastatic non small cell lung cancer 11/04 Left upper lobe cancer Left temporal metastasis

45
MRS Y Craniotomy 12/04 Pre-op chemotherapy – thoracotomy 6/05 Histology – squamous cell carcinoma

46
MRS Y. Admitted following seizure 7/05 MRI brain – progressive disease – site of initial brain metastasis, no new lesions SRS 7/05

48
MRS Y. Progressive systemic disease 12/05 – taxotere chemotherapy Partial response Latest systemic CT – stable appearances Further MRI head – 12/06

50
SURGICAL RESECTION + SRS No class I evidence to compare outcome between patients who have received surgery + WBRT Versus surgery + WBRT + SRS boost

51
METASTASES - PLYMOUTH Four craniotomies + SRS boost; 2 patients still alive - 20 and 21 months post SRS 2 died at 6 and 8 months post SRS Average survival 7 months

52
WBRT + SRS BOOST Andrews et.al 331 patients Solitary lesions WBRT + SRS boost (n =92) increased OS 4.9 to 6.5 months vs WBRT alone No difference in OS in pts with multiple metastases
 increased OS 4.9 to 6.5 months vs WBRT alone No difference in OS in pts with multiple metastases")
53
WBRT + SRS BOOST Significantly enhanced or stabilised KPS Reduced need for steroids Improved local control in both groups Therefore should be considered in good PS, 1-3 metastases

54
METASTASES - PLYMOUTH Eight WBRT + SRS boost; One pt alive – 17/12 post SRS Others died 4-19/12 post SRS Average survival 8.1 months

55
SRS WITHOUT WBRT RCT – 268 patients – SRS alone 301 SRS + WBRT But 24% of SRS alone group had salvage WBRT at disease relapse

56
SRS WITHOUT WBRT Japanese study – up-front WBRT significant benefit Better local control, but MS similar between two arms – SRS vs WBRT + SRS SRS alone – judicious FU to detect new metastases – further SRS or WBRT

57
METASTASES - PLYMOUTH 13 patients – SRS alone 8 patients have died – 6/52 – 12/12 post SRS Average survival 6.4 months 5 alive – 2-17/12 post treatment

58
METASTASES - PLYMOUTH 8 alive 6/52 to 22/12 post SRS Morbidity – two patients presented with raised ICP requiring mannitol/steroids Homonymous hemianopia

59
METASTASES - PLYMOUTH 15 patients have died – 3 - 19/12 survival post SRS Average survival 7.3 months Uncertainties: Date of diagnosis of brain mets Progression of systemic disease Intracranial progression

60
STEREOTACTIC RADIOSURGERY Precise, highly conformal treatment Dose escalation ‘Inoperable’ lesions Single treatment which may be repeated

61
Some morbidity – well managed Promising survival figures for patients with brain metastases Move toward extracranial SRS/SRT STEREOTACTIC RADIOSURGERY

Similar presentations









: The optimal indication for operable tumors in inoperable patients D.Katsochi 1, S.Kosmidis 1, A.Fotopoulou.>")










