Download presentation
Presentation is loading. Please wait.

1
Principles of Adhesion
Lina Sharab. DDS. MS. MSc

2
Bad habits Studying from PPP

3
Objectives Be familiar with the terminology: ( adhesion , adherent, adherend, smear layer, ,whitlockite, hybrid layer, primer, surface tension, wetting, polymerization, dentinal fluid and tubules,… Learn principle of adhesion and how it applies to dentistry. Factors affecting adhesion. The difference between adhesion to enamel and dentin. Dental bonding systems. Polymerization and shrinkage.

4
Advantages of adhesion in dentistry
Adhesion improvement helped in minimizing tooth preparation affected areas with no need for the removal of sound structures to achieve retention during initial prep or when repairing a restoration. Aid better distribution of functional stress across the bonding interface. Significantly improved esthetics in dentistry. Helped in composite restoration, closing diastemata, mask discoloration, add tooth structure, bond veneers, inlays, onlays, cement crowns, fissure sealants, bond brackets, ORT splints, treat hypersensitivity,…..etc

5
Principles of adhesion
Adhesion is the attachment of one substance to another without aid of external force. Adherend is the substrate that is adhered to. Adhesive or adherent or bonding agent the material that when applied to substrates can join then together. Bonding strength is a measure of the load bearing capacity of the adhesive. Durability is the time period which the bond remains effective. Adhesion is the force btween atoms at an interface that hold two materials together. Mode of failure could be adhesive or cohesive; it is often a mix. Latin ad (to) haerere (stick).
 haerere (stick).")
6
Theories of adhesion 1- Mechanical theory: solidified adhesive interlocks micromechanically with the irregularities the substrates. 2- Adsorption theory : all kinds of chemical bonds. 3- Diffusion theory: bonding between mobile molecules from each side to become one part. 4- Electrostatic theory: electrical double layer forms at the interface (metal-polymer) contributing to the bond.
 contributing to the bond.")
7
Principles of adhesion
Important requirements for adhesion: The two materials must have intimate contact. Sufficient wetting of the adhesive on the surface; this wetting depends on surface energy.

8
Principles of adhesion
What affects spreading or wetting? Surface energy is measured by the internal angle of a droplet on a surface (dynes/cm). Smaller angles means better spreading. Enamel which primarily is hydroxyapatite high surface energy Contaminants containing any organic material could lower surface energy.
. Smaller angles means better spreading. Enamel which primarily is hydroxyapatite high surface energy. Contaminants containing any organic material could lower surface energy.")
9
Other factors affects wetting
Hydrophilic Hydrophobic Wetting of adhesive: -Adhesive Must wet the surface -Have low viscosity to penetrate the irregularities. -Able to displace air and moisture during the process of adhesion.

10
Primer Conditioner Adheasive

11
Wetting of the adhesive:
In current systems primers contain 1) Hydrophilic monomer to improve wetting of the hydrophobic resin 2) Solvent like acetone or ethanol to replace water and air What does the primer do? Amphiphilic.
 Hydrophilic monomer to improve wetting of the hydrophobic resin. 2) Solvent like acetone or ethanol to replace water and air. What does the primer do Amphiphilic.")
12
Adhesion to enamel and dentin
The principle in adhesion to tooth is based in two phases 1) the removal of Ca Po and 2) diffusion of synthetic resin in the scaffold. Hybrid layer or zone: the zone in which resin of the adhesive system micromechanically interlocks with dentinal collagen. Recent studies suggested that the use of chlorhexidine help preserve the integrity of hybrid layer. Surface energy of etched enamel increases more than twice after etching (from 28 dynes/cm to 72 dynes/cm ).
 the removal of Ca Po and 2) diffusion of synthetic resin in the scaffold. Hybrid layer or zone: the zone in which resin of the adhesive system micromechanically interlocks with dentinal collagen. Recent studies suggested that the use of chlorhexidine help preserve the integrity of hybrid layer. Surface energy of etched enamel increases more than twice after etching (from 28 dynes/cm to 72 dynes/cm ).")
13
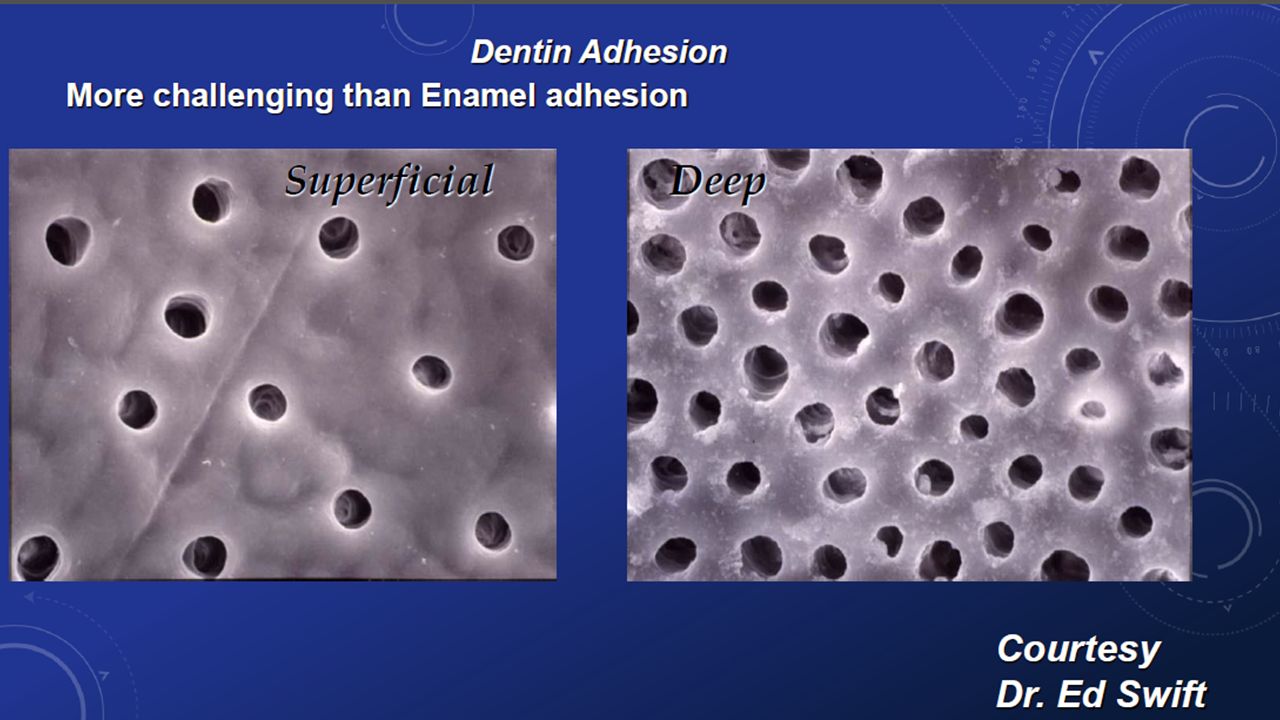
Enamel vs. dentin Enamel Dentin
Homogeneous in composition (almost) 95wt% hydroxyapatite. Heterogeneous in composition 70wt% hydroxyapatite Homogeneous in structure; prisms uniform despite the depth. Heterogeneous in structure; more tubules in the deeper dentin/m² (double). dentinal fluid in the deeper 1/3 Solid crystallites and non-dynamic Permeable and dynamic (secondary, tertiary (reparative), dentinal sclerosis) High surface energy; aids better wetting. Lower surface energy, less spreading of adhesives.
 95wt% hydroxyapatite. Heterogeneous in composition 70wt% hydroxyapatite. Homogeneous in structure; prisms uniform despite the depth. Heterogeneous in structure; more tubules in the deeper dentin/m² (double). dentinal fluid in the deeper 1/3. Solid crystallites and non-dynamic. Permeable and dynamic (secondary, tertiary (reparative), dentinal sclerosis) High surface energy; aids better wetting. Lower surface energy, less spreading of adhesives.")
14
Dr.Nagaoka

15
Adhesion to enamel and dentin
Adhesion in dentistry started in the mid 1960s with first commercial restorative composite. Acid etch technique was introduce to clinical dentistry in early 1960s. Total-etch has replaced the selective-enamel etching in 1990s. Then, universal enamel-dentin conditioners was introduced. Universal, or all purpose, or multi purpose adhesive.

16
Principles of adhesion
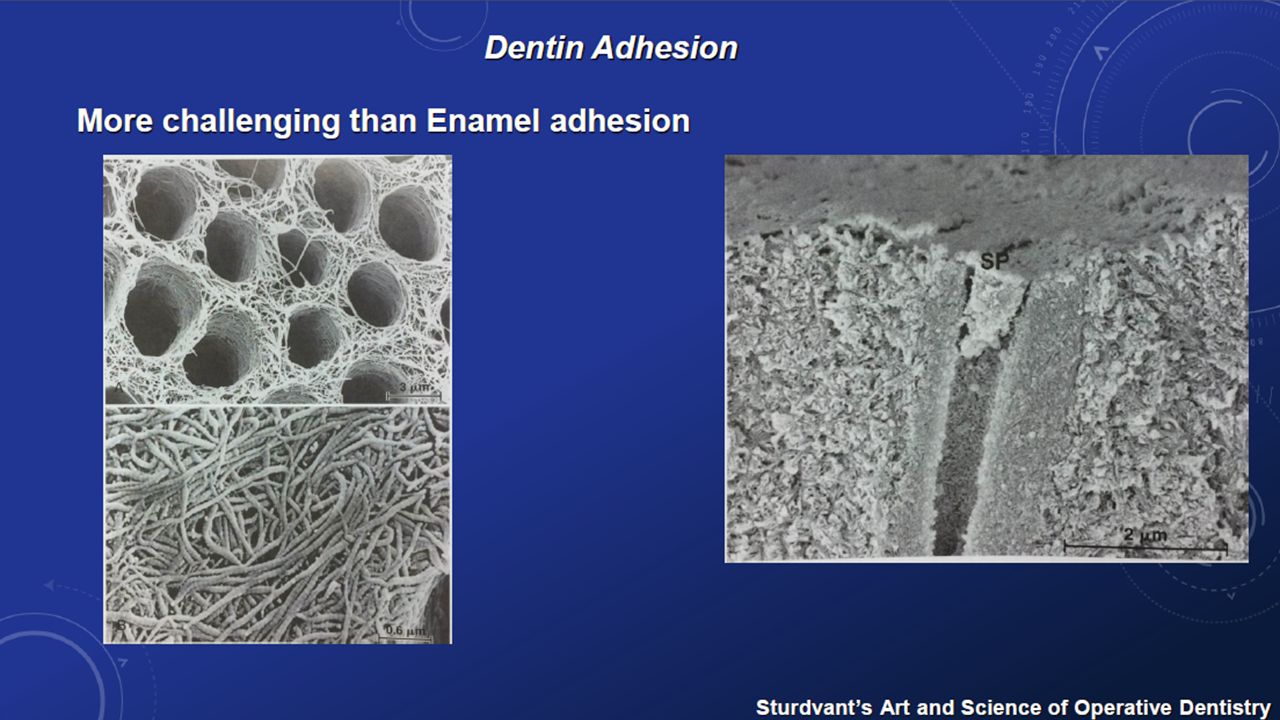
Smear layer An adherent layer of debris and can be found on tooth surface after having been cut with rotary or hand instrument. Consists primarily of shattered and crushed hydroxyapatite and fragments of collagen, bacteria and saliva. Average thickness .5-2 µm. Very irregular morphology. SL morphology depends on the technology used for cavity preparation (air abrasion, laser ablation, manual). Has advantages and disadvantages. Reduces dentine permeability by 86%. Attached weakly to dentin but cannot be removed by rinsing. Can be removed by conditioners (acid etch). Should we leave it or remove it?
. Has advantages and disadvantages. Reduces dentine permeability by 86%. Attached weakly to dentin but cannot be removed by rinsing. Can be removed by conditioners (acid etch). Should we leave it or remove it")
17
5 μm different self-etch adhesives with dentin. (Left) Unaffected dentin with SL. (Right) Interaction of three classes of self-etch adhesives with dentin and the smear layer. Because mild self-etch adhesives do not completely remove the smear layer, a relatively thin submicron hybrid layer is formed without resin tags. The intermediary strong self-etch adhesives remove the smear layer along with a shallow demineralization of dentin. Short resin tags (±10 μm) are formed, and a limited lateral wall hybridization takes place. In the bottom third of the hybrid layer, not all hydroxyapatite crystals have been dissolved. The micromorphologic aspect of strong self-etch adhesives is very similar to that of etch-and-rinse adhesives and is characterized by a 3-to 5-μm-thick hybrid layer, dentinal tubule funneling, extensive resin tags, and tubule wall and lateral tubule wall hybridization Resin tag: the polymerized resin extension in the tubule after etching. 15% of the bonding strength in dentin is ascribed to resin tags (From De Munck et al.Reprinted with permission.)
 Unaffected dentin with SL. (Right) Interaction of three classes of self-etch adhesives with dentin and the smear layer. Because mild self-etch adhesives do not completely remove the smear layer, a relatively thin submicron hybrid layer is formed without resin tags. The intermediary strong self-etch adhesives remove the smear layer along with a shallow demineralization of dentin. Short resin tags (±10 μm) are formed, and a limited lateral wall hybridization takes place. In the bottom third of the hybrid layer, not all hydroxyapatite crystals have been dissolved. The micromorphologic aspect of strong self-etch adhesives is very similar to that of etch-and-rinse adhesives and is characterized by a 3-to 5-μm-thick hybrid layer, dentinal tubule funneling, extensive resin tags, and tubule wall and lateral tubule wall hybridization. Resin tag: the polymerized resin extension in the tubule after etching. 15% of the bonding strength in dentin is ascribed to resin tags. (From De Munck et al.Reprinted with permission.)")
18
Removal of the smear layer Use bonding agent that penetrates the SL
Leave it or remove it? To overcome the low attachment strength 2 stratigies are used: Removal of the smear layer Use bonding agent that penetrates the SL Etch and rinse approach Self-etch approach successful Expose high surface energy that improves wetting and spreading of adhesive Leaves the surface with lower energy but the bonding agent can penetrate and incorporate into the bonding layer Removes the smear plug and exposes tubules exposing water and affecting wettability !! Reduces pulp sensitivity by leaving the tubules plugged 30%-40% phosphoric acid is used. The stronger the acid, more complete removal. Both weak and strong acids are used

20
Dentin near the DEJ (outer) and near the pulp (inner) are compared to show relative differences in intertubular and peritubular dentin and in lumen spacing and volume
 and near the pulp (inner) are compared to show relative differences in intertubular and peritubular dentin and in lumen spacing and volume")
21
Enamel prisms Taken from the web

22
Etched enamel prisms Taken from the web
Etched enamel is chalcky and have high surface energy 72/dyn/cm more than twice of the un etched. Etched enamel prisms Taken from the web

25
Classification of contemporary adhesives according to adhesion strategy and clinical application steps

26
Etch-and-rinse-adhesives
type 3 step Etch and rinse Two step Etch and rinse Advantages Separate bottles, low technique sensitivity, effective, most consistent long term results. Particles serve as shock absorber Simpler to apply, consistent and stable, single does package is hygienic and controlled Disadvantages Risk of over etching, time consuming, the need for rinsing, sensitivity to rinsing (wet-dry) Not substantially faster, more sensitive, risk of bonding layer too thin, risk of over etching, sensitive to dentin wetness, lower bonding effectiveness.
 Not substantially faster, more sensitive, risk of bonding layer too thin, risk of over etching, sensitive to dentin wetness, lower bonding effectiveness.")
27
Self-etch adhesives type 2 step Etch and rinse one step Etch and rinse Advantages No etching, rinsing, or drying, saves time, less sensitive to dentin wetness, consistent and controlled, hygienic, desensitizes dentin Most time efficient, less sensitive to dentin wetness Dis-advantages More elaborate application, incompatible with autocured resin, less research is done, sensitive to water, reduced shelf life, impaired durability. More technique sensitive, no long term data. Sensitive to water, short shelf life, impaired durability.

28
Polymerization contraction of restorative resins
Linking monomers into polymer chains during polymerization leads to volume shrinkage. currently used resin composites shrinks vol% during free polymerization This shrinkage creates stress within the resin of 7MPa,clinically this stress is created between the walls and the restoration. Microleakage: Passing of bacterial and their toxin ben restoration margins and tooth preparation walls pulpal irritation.

29
Polymerization contraction of restorative resins
In industry this problem was solved by double ring opening polymerization that shrinks only 1 vol%. It is being evaluated for the use in dentistry.

30
Compensation for polymerization shrinkage
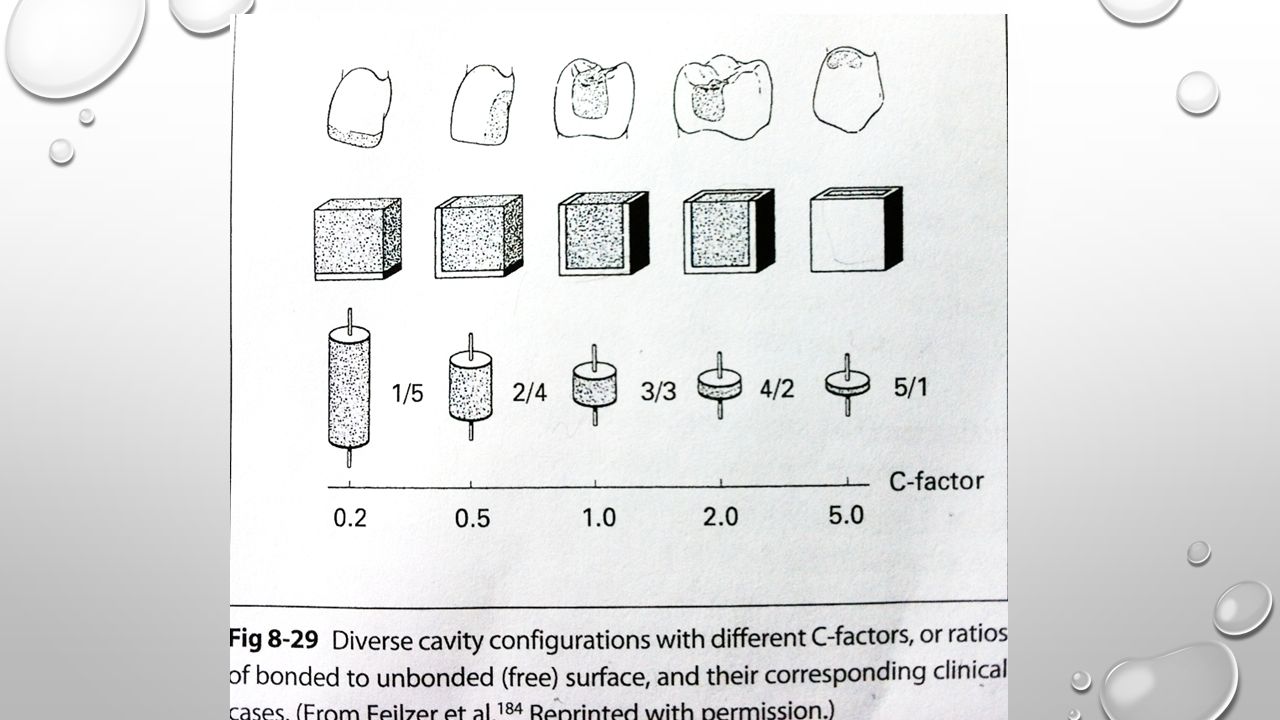
Flow or plastic deformation: It takes place during the early stage of setting when the contraction stress exceeds the elastic limit of the resin. Then decreases as the setting continues due to increase stiffness of the resin. Fast setting light cure exhibits less flow related stress relief than self-curing resin. A combination of slow and rapid cure considered favorable. C-factor is the ratio between the bonded to unbonded surfaces The higher the C factor, the more stress produced

32
Compensation for polymerization shrinkage
Fillers: Placement of precured or inert blocks in the resin before curing. Megafilled, macrofilled, microfilled resin composite. Use of inlays can help BUT higher C-factor. Microfilled have higher flexure rate and this helps the margins especially in wedge preps. However, there are other problems associated with microfills.

34
Compensation for polymerization shrinkage
Light curing adjustment: The so called soft-start, produces low intensity light (400mW/cm2) for 10 sec then increase to 800mW/cm2. Incremental placement is recommended in this technique. Camphorquinone is the photosensitizer that receives the photons and creates free radicals that initiate the polymerization process.
 for 10 sec then increase to 800mW/cm2. Incremental placement is recommended in this technique. Camphorquinone is the photosensitizer that receives the photons and creates free radicals that initiate the polymerization process.")
35
Incremental placement of composite

36
Light cure Vs. self-cure composite
Light-cured Autocured Initial setting occurs close to the light source Occurs in the bulk at the center! Fusayama “ at the base close to the pulp Faster setting low flow relaxation more stress Incremental technique is recommended. BUT shrinkage is debated. Increments are not necessary Clinically easier to deal with Takes longer time that may introduces contamination

37
Compensation for polymerization shrinkage
Cervical sealing: Sealing of cervical marginal gaps with unfilled low viscosity resin applied and cured after the restorative resin has been cured. (i.e. Permaseal) BUT it is very laborious and to sensitive to contamination. True bond will transfer the stress evenly on the remaining tooth.
 BUT it is very laborious and to sensitive to contamination. True bond will transfer the stress evenly on the remaining tooth.")
38
Safety consideration of composites
Thermal expansion of composite is 4 times more than that of the tooth structure. Microfilled resin expands more than hybrid composite marginal gap formation. However this difference my not be reflected clinically. Biocompatibility: free monomers are harmful. Acid etch affect 10 micrometer in depth of the dentin so if there is a 1mm thick dentine pulp should not be irritated. The current clinical standard is if dentin is less than .5mm, Calcium hydroxide should be used for its healing properties. BUT it dissolves rapidly leaving gaps.

39
Glass-ionomer cements
Also called polyalkenoates. The only dental material that exhibit true chemical bond. Comes as powder containing calcium aluminosilicate glass and liquid that contains acrylic acid in water Carboxyl group of the acid interact with calcium in hydroxyapatite to form ionic bond.

40
Glass-ionomer cements, cont.
Releases free fluoride ions that has anti-cariogenic properties, therefore it is recommended for people with high risk of caries. Only weak conditioner is required (polyalkenoic acid). Disadvantages:. Sensitive to changes in water content. Short working time and long setting time. Early moisture contamination removes metallic ions and causes shrinkage. Physical properties and esthetics are inferior to composites.
. Disadvantages:. Sensitive to changes in water content. Short working time and long setting time. Early moisture contamination removes metallic ions and causes shrinkage. Physical properties and esthetics are inferior to composites.")
41
Glass-ionomer cements, cont.
Resin modified glass-ionomer Cements: Dual cured and consist of both glass powder and resin monomers Mechanical properties are better than conventional G-I. Longer working time. Fluoride release is better than conventional G-I. Retention is better than adhesives. Glass-ionomer cements, cont.

42
Chronological classification:
In 1956, Buonocore reported “resin could bond to a hydrochloric acid-etched dentin surface First Generationg Second Generation Third Generation Fourth Generation Fifth Generation Sixth Generation Sturdevant’sArt and Science of Operative Dentistry

43
Other application for bonding
Amalgam Bonding: Helps sealing the margins and prevent tooth staining, increases shear stress and stronger bond in vitro. No clinical results suggest better results than conventional amalgam. Autocure, or lightcure?

44
Other application for bonding
Ceramic Bonding: Both mechanical and chemical bonds exist between adhesive and silica based ceramic. Usually etched with hydrofluoric acid to increase porosity and micromechanical bonding. Dual cure cement is recommended unless less than 2.5mm thickness of penetration.

45
Skill Remember! Good dentist Knowledge Ethics

Similar presentations