Download presentation
Presentation is loading. Please wait.

1
Dr. Maha Al-Sedik

4
Pain Pathophysiology: Pain may be: Visceral. Referred. Assessment: Use OPQRST to evaluate type and severity.

5
Management After assessing ABCs, allow patient to assume a position of comfort. Be prepared for potential nausea and vomiting. Provide spasmolytic if necessary. Establish an IV line.

6
Urinary Tract Infections (UTIs) Definitive treatment requires antibiotics. Pathophysiology: Usually develops in lower urinary tract. Spread if untreated.

7
Classic symptoms: Painful urination. Frequent urges to urinate. Difficulty urinating. Pain. Patients appear restless and uncomfortable. Vital signs vary based on degree of illness.

8
Management Mainly supportive care of ABCs. Transport in a position of comfort. Be prepared for nausea or vomiting. Analgesics in severe cases only. Establish an IV line.

9
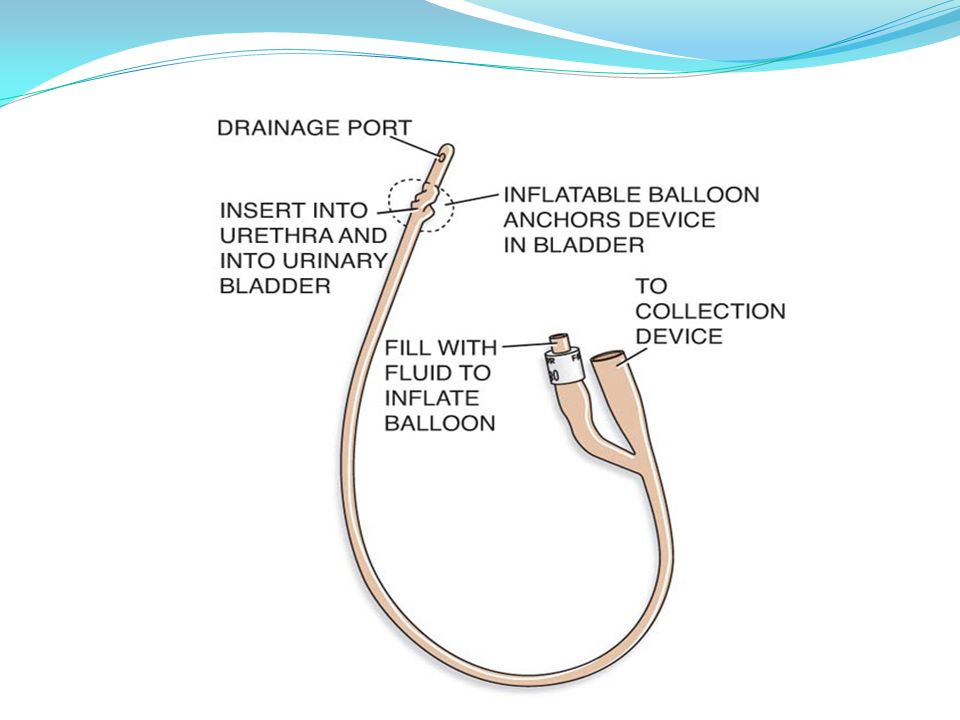
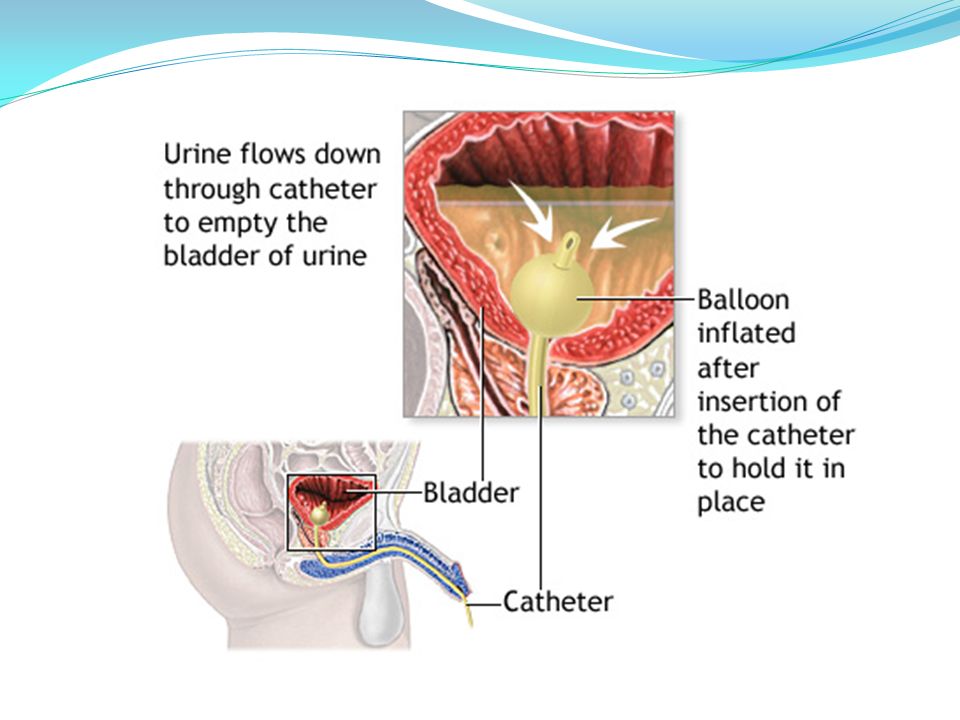
Urinary Catheters Many patients hospitalized for a urinary problem or disease receive catheterization. Urine backflow is a concern when transporting a catheterized patient. Do not lift the drainage bag while handling the patient.

13
Urinary Incontinence Loss of bladder control. Medical problem if in one of two categories: Urge incontinence. Overflow incontinence.

15
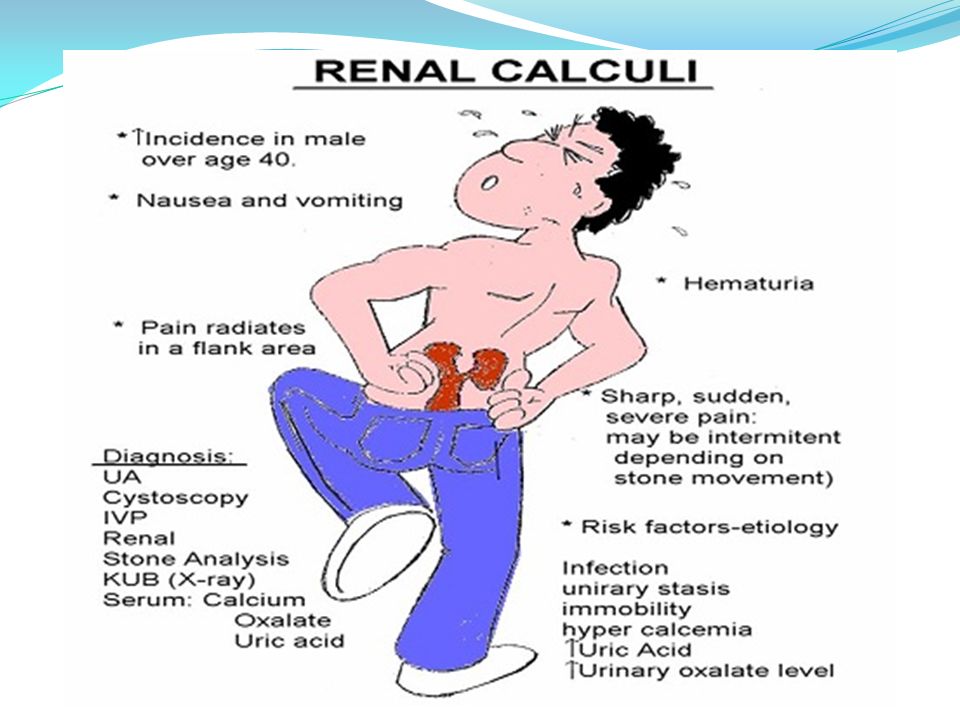
Renal Calculi (Kidney Stones) Pathophysiology: Originate in renal pelvis. Form when an excess of insoluble salts or uric acid crystallizes in the urine.

17
Common Types of the stones Calcium stones Triple phosphate Uric acid cystine stones

18
Assessment findings: Patients almost always experience pain. Patient may be restless or guard abdomen. Palpation may be difficult. Vital signs vary.

19
Management Ensure ABCs. Position of comfort Administer analgesia if local protocols allow. Establish an IV line and administer fluids.

20
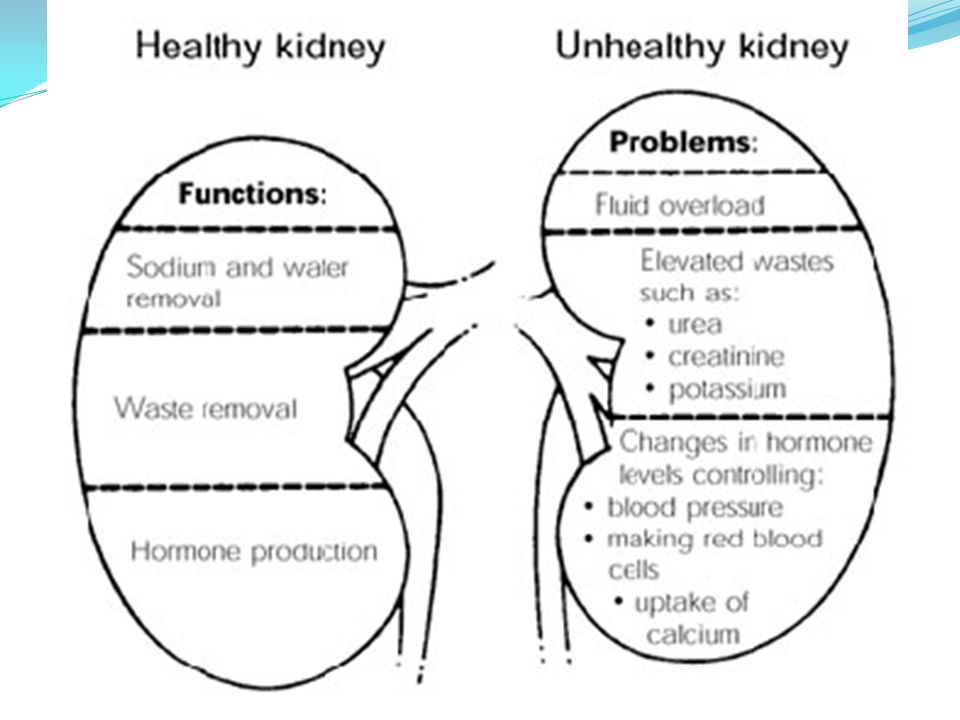
Acute Renal Failure (ARF) Sudden decrease in filtration through the glomeruli. Causes toxins to accumulate in the blood.

21
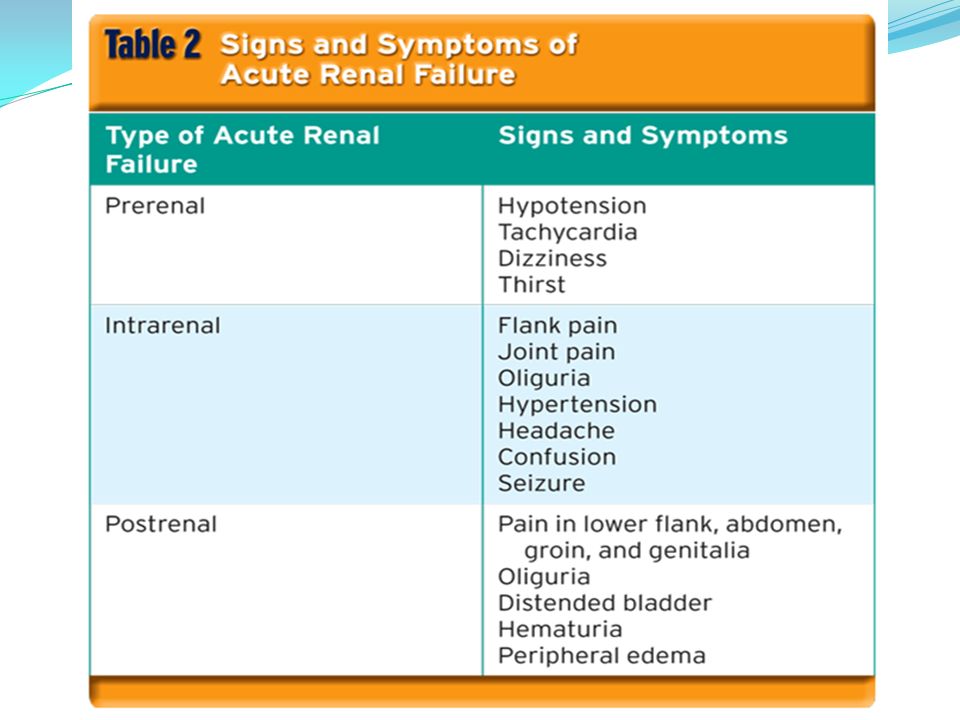
Oliguria: Urine output of less than 500 mL/day. Anuria: Complete cessation of urine production. Patient may experience: Generalized edema. Acid buildup. High levels of nitrogenous compounds in the blood. High levels of metabolic wastes in the blood.

22
If untreated, can lead to: Heart failure Hypertension Metabolic acidosis Classified into three types Based on where it occurs

23
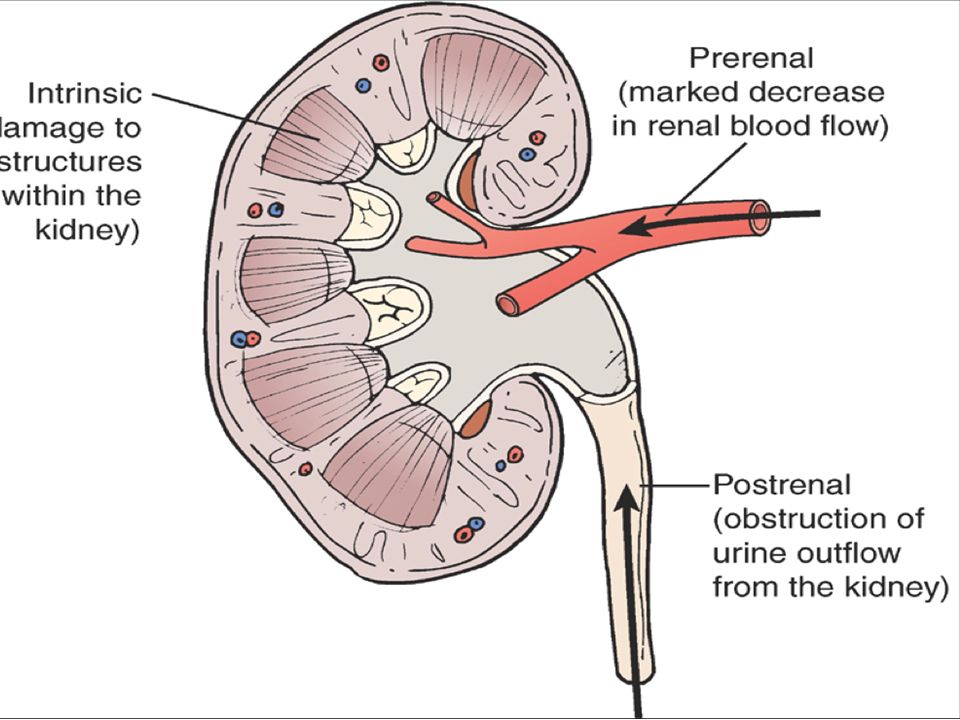
Prerenal ARF: Caused by hypoperfusion of the kidneys. Intrarenal acute renal failure (IARF): Involves damage of the kidney. Postrenal ARF: Caused by blockage of urine flow from kidneys. Types of acute renal failure
: Involves damage of the kidney. Postrenal ARF: Caused by blockage of urine flow from kidneys. Types of acute renal failure.")
25
Prerenal ARF Intrarenal (IARF) Postrenal ARF
 Postrenal ARF")
28
Management Metabolic changes caused by ARF are life threatening. Support the ABCs. Place in shock position.

29
Pathophysiology Inadequate kidney function caused by the permanent loss of nephrons. Scarring occurs as the damaged nephrons cease to function. Uremia and accumulation of toxins develop. Systemic complications develop. Chronic Renal Failure (CRF)
.")
31
Assessment findings Patients present with: An altered level of consciousness edema Accumulation of nitrogenous waste products. Oliguria anaemia

32
Management Similar to patients with ARF Patients will ultimately require renal dialysis. Due to electrolyte imbalances, be conservative with treatment plans. Transport in a calm manner.

33
End-Stage Renal Disease (ESRD) Pathophysiology Result of untreated acute or chronic renal failure Kidneys have lost all ability to function Fatal unless treated by dialysis or renal transplant
 Pathophysiology Result of untreated acute or chronic renal failure Kidneys have lost all ability to function Fatal unless treated by dialysis or renal transplant")
34
Management Treatment is limited to renal dialysis or kidney transplant. Support ABC. Place the patient in the shock position.

35
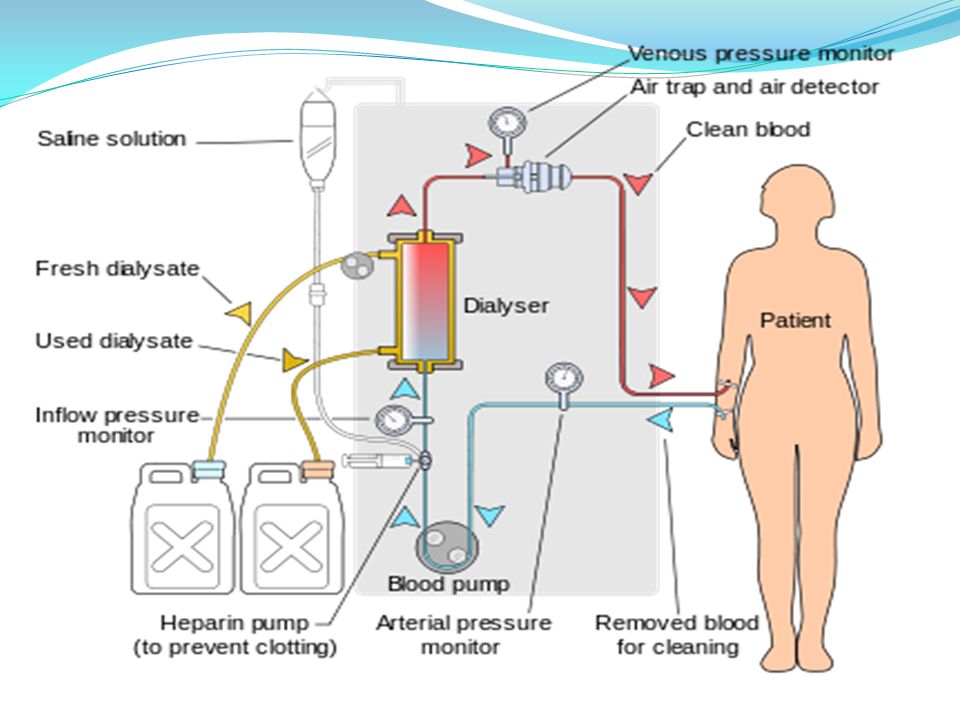
Renal Dialysis

37
Technique for: Filtering the blood of its toxic wastes. Removing excess fluid. Restoring the normal balance of electrolytes. Renal Dialysis Patients requiring dialysis usually undergo the process every 2 or 3 days for 3 to 5 hours.

38
Principles of dialysis: The process of diffusion: Blood cells are too big to pass through the dialysis membrane, but body wastes begin to diffuse (pass) into the dialysis solution. Diffusion is complete. Body wastes have diffused through the membrane, and now there are equal amounts of waste in both the blood and the dialysis solution.

39
Patients who miss dialysis treatments often present with signs of electrolyte imbalance. Other complications of dialysis include: Infections at the IV site

40
Male Genital Tract Conditions Epididymitis Infection that causes inflammation of epididymis along the posterior border of testis. Orchitis When one or both testes become infected Prehospital management is supportive.

42
Fournier gangrene Causes infection and necrosis of the subcutaneal tissue and muscle in the scrotum The scrotum will be spongy. Tissues will be gray-black. Prompt transport is required. Assess and treat for shock.

43
Benign prostate hypertrophy (BPH) Age-related nonmalignant enlargement of the prostate gland May be asymptomatic, or may lead to: Difficulty starting urine flow Incomplete emptying of the bladder Increased urination at night
 Age-related nonmalignant enlargement of the prostate gland May be asymptomatic, or may lead to: Difficulty starting urine flow Incomplete emptying of the bladder Increased urination at night")
46
Testicular torsion Twisting of the testicle on the spermatic cord Medical emergency if twisting reduces blood flow to testis Usually unilateral Transport carefully and promptly.

Similar presentations

























 that can damage.>")

