Download presentation
Presentation is loading. Please wait.

1
Stroke Local Pharmacy Group meeting 7 th May 2013 Dr. Lucy Sykes

2
Outline Overview of stroke Case presentation Risk factors Atrial fibrillation Targets Treatment options TIA Resources

3
What is a stroke? Focal neurological deficit > 24 hrs 2/3 infarction, 1/3 haemorrhage (UK) 3 rd leading cause death in UK (11%) Significant cause of major disability Risk recurrence within 5 yrs ~ 40%
 3 rd leading cause death in UK (11%) Significant cause of major disability Risk recurrence within 5 yrs ~ 40%.")
4
Risk factors High BP High cholesterol Diabetes (DM) Smoking Atrial fibrillation Previous or family history
 Smoking Atrial fibrillation Previous or family history")
5
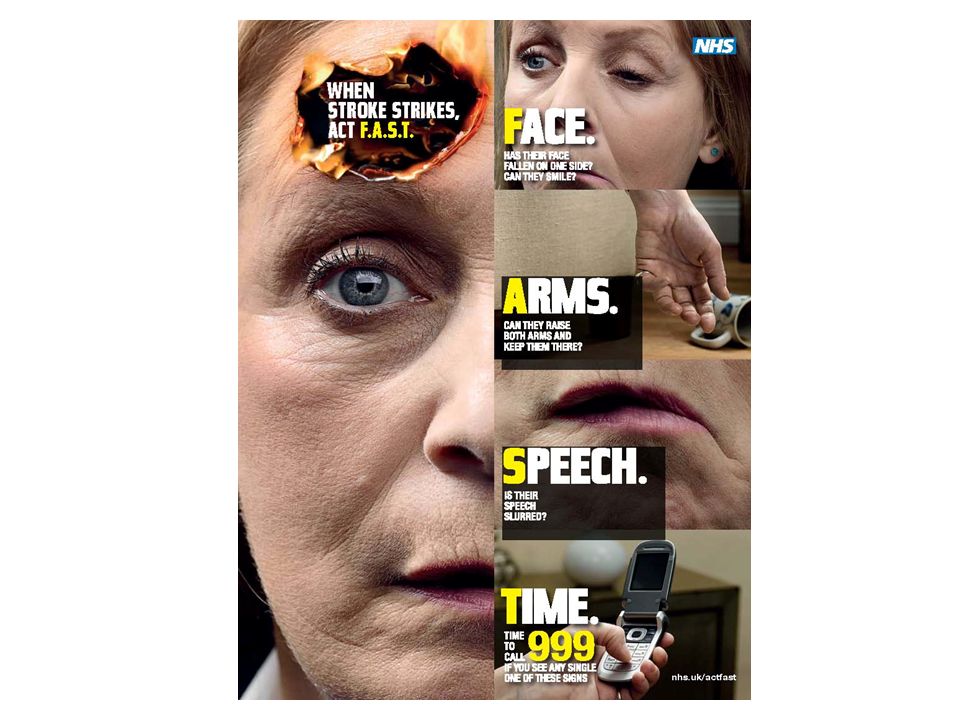
A case 95 year old lady Sudden onset whilst watching TV Right arm / leg weakness Slurred speech Headache Daughter did FAST test = positive

7
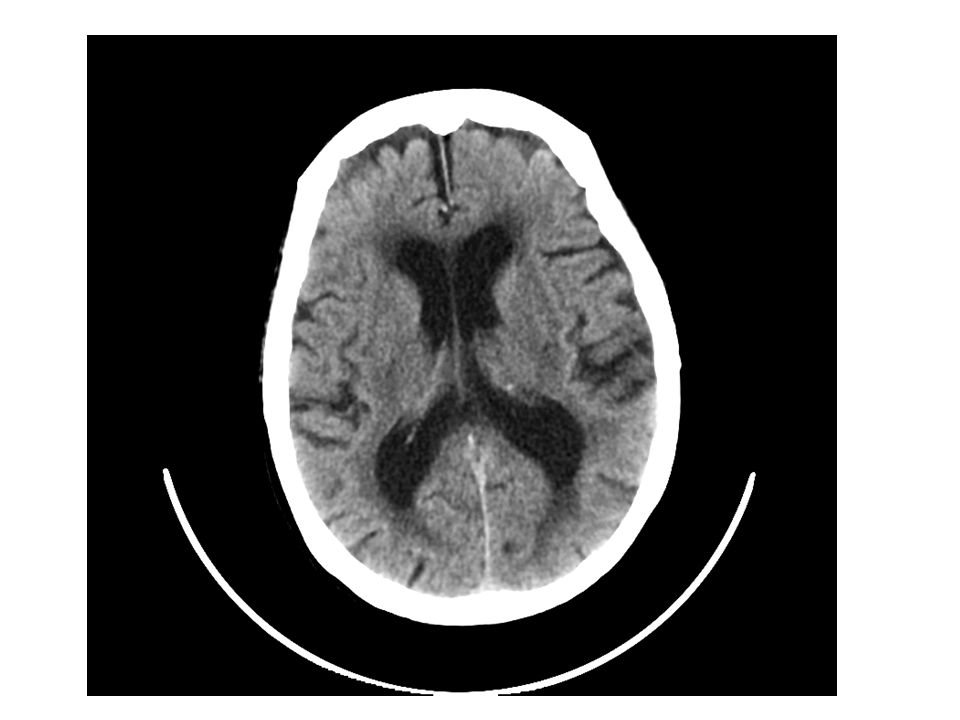
Arrived in ED Seen by stroke consultant & nurse Considered for thrombolysis CT brain showed no bleed Not for thrombolysis as >4.5 hours since time of onset Transferred to stroke unit

9
Standard acute stroke treatment Aspirin 300mg od 2/52 Then clopidogrel 75mg od long term Control risk factors (BP, diabetes, chol) Life-style advice (smoking, diet, exercise) Look for cause of stroke
 Life-style advice (smoking, diet, exercise) Look for cause of stroke")
10
TOAST Classification 1Large artery atherosclerosis 2Cardioembolism 3Small vessel occlusion (lacunar) 4Other determined aetiology 5Undetermined aetiology
 4Other determined aetiology 5Undetermined aetiology")
11
Investigations Fasting chol & glucose ECG / 24 hour tape Echocardiogram USS doppler neck arteries

12
Results 1 BP 200/110 (target is 130/80) Not diabetic (target in DM is glu 4-11) High chol 6.2 (target is chol <4, LDL <2)
 Not diabetic (target in DM is glu 4-11) High chol 6.2 (target is chol <4, LDL <2)")
13
Treatment options 1 BP –Evidence for all antihypertensives in stroke –Target BP is most important thing –Choice depends on SE profile ACE-i or A2RB Ca2+ channel blockers B-blockers

14
Treatment options 2 Cholesterol –Statins = main-stay of therapy –Benefits even if normal chol (plaque stability) –Rosuva good for those with myositis Diabetes –Usual diabetic treatment options –SU, metformin, gliptins, insulins
 –Rosuva good for those with myositis Diabetes –Usual diabetic treatment options –SU, metformin, gliptins, insulins")
15
Results 2 24 hour ECG - paroxysmal AF Echo – good cardiac funct, enlarged LA Neck arteries – no stenosis

16
ECG Normal sinus rhythm –Normal heart rate –Regular rhythm –P waves –Steady baseline AF –Heart rate increased (tachyarrhythmia)* –Irregularly irregular rhythm –No P wave P Ashley EA,Niebauer J. Cardiology Explained. Remedica: London 2004 *Reduced heart rate (bradyarrhythmia) may also be observed Regular rhythm Irregularly irregular rhythm
 may also be observed Regular rhythm Irregularly irregular rhythm.")
17
Why does AF matter? Symptoms –Palpitations –Chest pain –Breathlessness –Reduced exercise tolerance Complications –Risk of clot formation, i.e. risk of embolus to brain or elsewhere in body

18
Stroke risk in AF

19
Rate vs. rhythm Prevent fast / slow rates vs. Correct back into sinus rhythm Both effective at improving –Mortality –Stroke risk –Symptoms –Quality of life

20
Treatment options for AF Adapted from Prystowsky EN. Am J Cardiol 2000;85:3D–11D. STROKE PREVENTION Vitamin K antagonists (e.g. warfarin) Aspirin / clopidogrel Dabigatran etexilate Rivaroxaban Apixaban PHARMACOLOGICAL Removal/isolation of left atrial appendage NON-PHARMACOLOGICAL Anti-arrhythmic drugs – Class IA – Class IC – Class III MAINTENANCE OF SINUS RHYTHM PHARMACOLOGICAL Ablation Surgery (MAZE procedure) NON-PHARMACOLOGICAL CONTROL OF HEART RATE -blockers Calcium channel blockers (non-DHP) Digoxin PHARMACOLOGICAL Ablation/permanent pacing NON-PHARMACOLOGICAL DHP = dihydropyridine
 Aspirin / clopidogrel Dabigatran etexilate Rivaroxaban Apixaban PHARMACOLOGICAL Removal/isolation of left atrial appendage NON-PHARMACOLOGICAL Anti-arrhythmic drugs – Class IA – Class IC – Class III MAINTENANCE OF SINUS RHYTHM PHARMACOLOGICAL Ablation Surgery (MAZE procedure) NON-PHARMACOLOGICAL CONTROL OF HEART RATE -blockers Calcium channel blockers (non-DHP) Digoxin PHARMACOLOGICAL Ablation/permanent pacing NON-PHARMACOLOGICAL DHP = dihydropyridine.")
21
Which treatment for AF? CHADS 2 < 2nothing CHADS 2 > 2warfarin / NOAC CHADS 2 scoreAnnual stroke risk % 01.9 12.8 24.0 35.9 48.5 512.5 618.2

22
CHADS 2 = 2? CHA 2 DS 2 VASc ConditionPoints CCongestive cardiac failure1 HHypertension (> 140/90)1 A2A2 Age ≥ 742 DDiabetes1 S2S2 Previous stroke / TIA / VTE2 VOther vascular disease1 AAge 65-741 ScSex category (female)1
1 A2A2 Age ≥ 742 DDiabetes1 S2S2 Previous stroke / TIA / VTE2 VOther vascular disease1 AAge ScSex category (female)1.")
23
CHA 2 DS 2 VASc = 0nothing CHA 2 DS 2 VASc = 1warfarin / NOAC CHA 2 DS 2 VASc ≥ 2warfarin / NOAC CHA 2 DS 2 VAScAnnual Stroke Risk % 00 11.3 22.2 33.2 44.0 56.7 69.8 79.6 86.7 915.2

24
Warfarin Target INR in AF 2-3 Time in therapeutic range >72%

25
TIA (mini-stroke) Focal neurological deficit < 24 hrs –in practice < 1hr Treatment essentially same as for stroke –Warning of high stroke risk Urgent referral to TIA clinic Risk factors & investigations same
 Focal neurological deficit < 24 hrs –in practice < 1hr Treatment essentially same as for stroke –Warning of high stroke risk Urgent referral to TIA clinic Risk factors & investigations same")
26
TIA treatment CT scanning - ? bleed –If no bleed give clopidogrel 300mg stat then 75mg od US doppler neck arteries - ? Stenosis >50% –If pos need urgent vascular surgical review ECG - ? AF –If pos need urgent anticoag with warf + clex or NOAC (anticoag instead of clop) Other investigations as OP
 Other investigations as OP.")
27
Key messages TIA & stroke essentially the same –Both need urgent medical attention FAST Look for a cause Manage risk factors & meet targets

28
Useful resources www.stroke.org.uk –The Stroke Association –For professionals & patients www.basp.ac.uk –> ‘resources’ –> ‘changes to RCP guidelines for stroke 2012’

Similar presentations




 -Pt acutely unwell with palpitations -Pt with haemodyanically unstable acute onset AF -2 nd /3 rd heart block -Exercise.>")














