Download presentation
Presentation is loading. Please wait.

1
THROMBOTIC MICROANGIOPATHIES DR.SRIKANTH SILIVERU JR.CONSULTANT CRITICAL CARE

2
18 year old female presents to ER 1) Confusion of 2 days duration with a fever. No family present to give history. No known past medical problems. On exam, she is 150 pounds, a temp of 39.5, and blood pressure of 90/60. She is obtunded. There are no skin rashes or meningeal signs. Fundi are normal. Cardiopulmonary exam is unremarkable. Lab: HCT of 21, platelet count:20K, BUN of 80, creatinine of 3.0. Reticulocyte count is mildly elevated at 4.0%, with an elevated LDH of 700U/L. Chest X- ray is unremarkable. EKG is sinus tachycardia.

3
*PT and pTT are normal. *D-dimer is negative with normal fibrinogen *Head CT was negative for intracranial bleed. *Lumbar puncture was not performed secondary to low platelet count. *Broad spectrum antibiotics were started to cover for meningitis and possible sepsis. *Patient is given a 2L NS bolus and quickly rushed to the ICU.

5
Thrombotic microangiopathies are microvascular occlusive disorders that are a common pathway of different pathological processes. Such disorders are characterized by systemic or intrarenal aggregation of platelets and/or fibrin, mechanical injury to red blood cells, and thrombocytopenia.

6
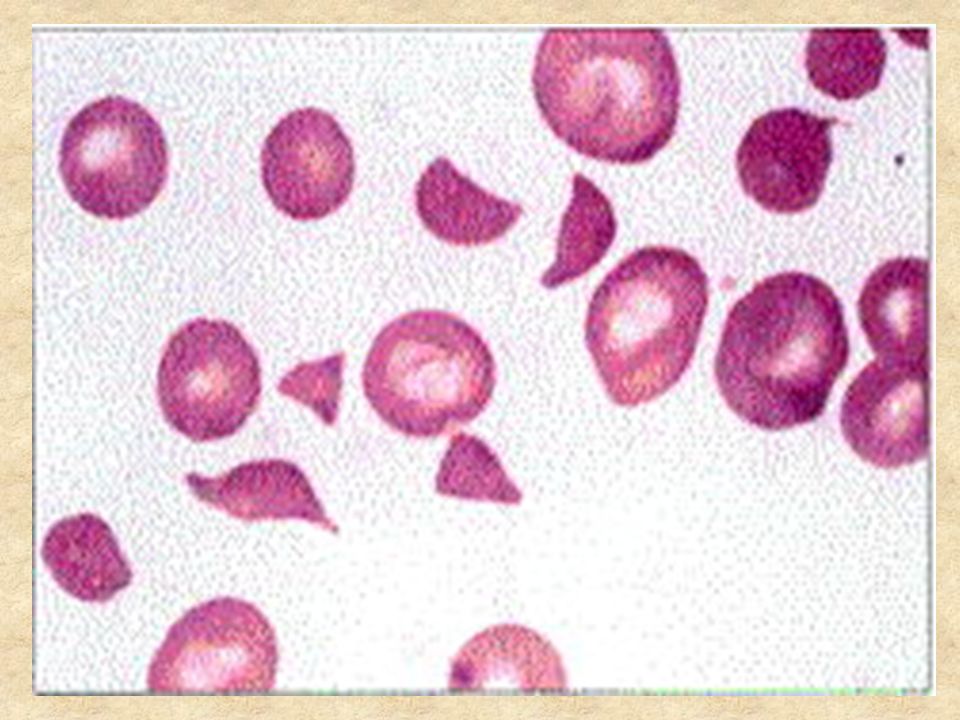
Thrombotic Microangiopathy Key diagnostic features – Microangiopathic hemolytic anemia Schistocytes Hemolysis – Thrombocytopenia – End organ damage

7
Thrombotic Thrombocytopenia Purpura Four general types exist: -infantile -acquired -drug induced -systemic disease Overall incidence is low with approximately 3.7 cases/1,000,000 population.

8
Familial TTP May appear in infancy or early childhood Recurs at monthly intervals Prognosis very poor Caused by a deficiency of ADAMST13, an endothelial protease

9
Acquired TTP Usually occurs in adults and children, with a peak in the second decade of life Is sporadic and characterized as a single acute episode, although recurrences can occur Thought to be caused by an autoantibody to ADAMST13

10
Drug-Induced TTP Quinine typically most common Anti-platelet agents ticlopidine and clopidogrel have been associated with TTP presenting in adults Mechanism of action unknown, except quinine know to induce autoantibody against platelets

11
Systemic Disease Associated with TTP Adenocarcinoma of Stomach / Pancreas / Prostate Antiphospholipid Antibody Syndrome Systemic Lupus Erythematosus Pregnancy/Contraception AIDS

12
The Pentad of TTP: Thrombocytopenia MAHA Mental status changes: only seen in 40-50% Renal insufficiency: most often mild – Proteinuria most common Fevers: 20%

13
Other Abnormalities LDH elevations (>2-3x nl) Myocardial involvement Pulmonary involvement Gastrointestinal involvement – Pancreatitis
 Myocardial involvement Pulmonary involvement Gastrointestinal involvement – Pancreatitis")
14
Pitfalls in Diagnosis Classic pentad most often not present Thrombocytopenia may be mild (20- 60,000/ul) Neurological defects vague Diagnosis not thought of
 Neurological defects vague Diagnosis not thought of")
15
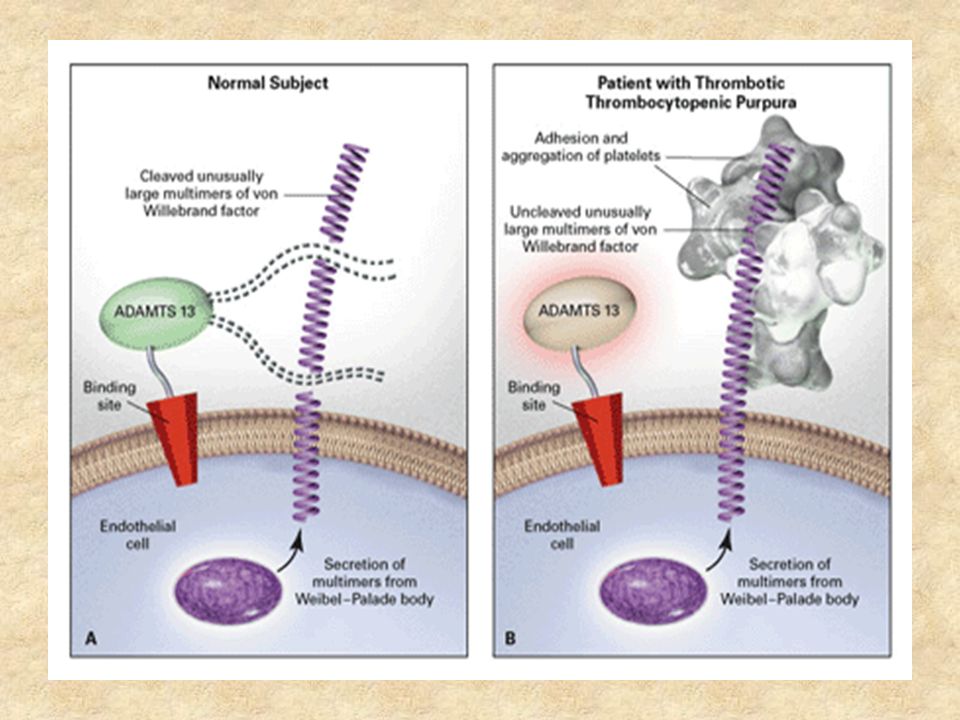
Pathophysiology of TTP More well defined Microvascular thrombi consist only of platelet aggregates. No perivascular or endothelial cell damage. Platelet aggregates contain abundant von Willebrand factor multimers, which are the precleaved form of vWf antigen and bind platelets at the glycoprotein 2B/3A receptor with high affinity.

16
Pathophysiology of TTP: A metalloprotease enzyme (ADAMS T13) is usually produced by hepatocytes, binds to endothelial cells by a thrombospondin receptor, and cleaves vWf multimers to produce monomers with a low affinity for platelet binding.
 is usually produced by hepatocytes, binds to endothelial cells by a thrombospondin receptor, and cleaves vWf multimers to produce monomers with a low affinity for platelet binding.")
17
VWF GPIb

18
VWF GPIb

19
VWF ADAMTS13 VWF

20
ADAMTS13 GPIb

22
ADAMTS13 in TTP Papers have demonstrated lack of ADAMTS13 activity in TTP patients – IgG inhibitory antibody found in many patients – ADAMTS13 activity increased with exchange Usually decreased in classic TTP Usually normal in classic HUS Mutations seen in hereditary TTP/HUS

23
Hemolytic Uremic Syndrome Diverse group of disorders -Inherited -Post-Infectious -Drug related -Thrombotic Microangiopathy

24
Post-Infectious HUS Most common cause of renal failure in children less than 4 years of age, epidemic cases are associated with a bacterial protein referred to as a shiga toxin Organisms most commonly associated- E. Coli 0157:H7, shigella dysenteria type 1, and rare cases of Streptococcus pneumonia (mechanism not currently known) 9 to 30% of patients with E. Coli 0157:H7 infection progress to having HUS
 9 to 30% of patients with E. Coli 0157:H7 infection progress to having HUS.")
26
Hemolytic Uremic Syndrome In the state of North Carolina, the average number of reported E. Coli 0157:H7 cases per year from 1997-2000 was 97. Beef and cattle are the main reservoir, with risk of transmission greatest when ingesting uncooked or partially cooked meat and/or unpasteurized dairy products.

27
Post-Infectious HUS- Strep. Pneumonia Usually have a poorer clinical outcome in comparison to shiga toxin induced HUS A study in Pediatrics 2000 found that children were younger (22.1 vs. 49 months), more likely to require dialysis (75 vs. 49%), had longer hospital stays (33.2 vs. 16.1 days), and received more platelet and red blood cell transfusions.
, more likely to require dialysis (75 vs. 49%), had longer hospital stays (33.2 vs days), and received more platelet and red blood cell transfusions..")
28
Inherited HUS- Factor H deficiency Relatively common cause of HUS and accounts for approx. 5-10% of all cases Factor H is an important enzyme in the complement cascade, which when absent, allows unregulated complement mediated cell lysis Such cell lysis is preferentially localized to glomerular endothelial cells causing the symptom complex of HUS

29
Drug Induced HUS Associated with immunosuppressants cyclosporine, tacrolimus and is a seen side effect after allogenic bone marrow, kidney, liver, heart, and lung transplantation. OKT3 implicated in transplanted kidneys found to have evidence of HUS Occurs after prolonged combination chemotherapy and total body irradiation, with mitomycin and cisplatin common agents implicated Mechanism of these microangiopathies unknown

30
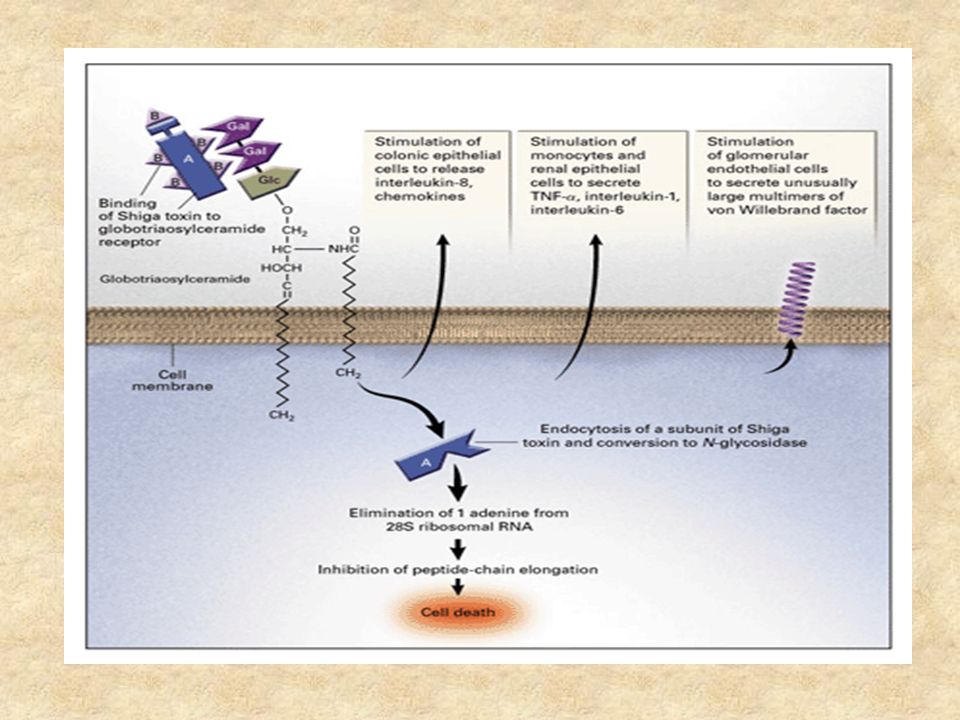
Proposed Mechanism of HUS Shiga toxin binds by the B subunit to colonic epithelia, generating an intense inflammatory response mediated by neutrophils and interleukin-8. Higher initial WBC is thought to be a predictor of worse outcome because of the intense neutrophil response. Binding of the shiga toxin allows bacterial entrance to mucosal cells causing cell death and exposing underlying vasculature.

31
Proposed Mechanism of HUS Shiga toxin crosses into the circulation and travels by platelets/monocytes to bind to glomerular, mesangials, and renal tubular epithelial cells. Toxin stimulated renal epithelial cells may secrete unusually large multimers of vWf that then bind toxin activated platelets. ADAMTS 13 activity is thought to be impaired secondary to interaction with Gb3 receptors on endothelial cells.

32
HUS- Why the Kidneys? Gb3, the glycolipid receptor responsible for binding the B subunit of shiga toxin, is expressed 50X more in kidney than in the endothelial cells of lung or liver. The shiga toxin appears to stimulate release of TNF from kidney cells in vitro, which may in turn stimulate increased production of Gb3 further potentiating injury.

33
aHUS Disease of uncontrolled complement activation leading to renal failure Difficult to diagnoses Course in past usual terminated in renal failure/death

34
Therapy of TTP/HUS: Plasma Exchange Plasma exchange has become standard of care for all patients given the diagnosis of TTP. Prior to plasma exchange, the 6 month mortality of patients with TTP was greater than 90%. Goal is to rapidly reduce circulating levels of autoantibody against ADAMST13 and other possible prothrombotic compounds present in patients’ serum.

35
Therapy of TTP/HUS: Plasma Exchange Venous blood is withdrawn and separated into blood cells and plasma. (plasmapheresis) Separation occurs by centrifugation (intermittent or continuous), or by a membrane filter with a selective pore size for plasma. Blood cells cells are then mixed with FFP and given back to patient.
 Separation occurs by centrifugation (intermittent or continuous), or by a membrane filter with a selective pore size for plasma. Blood cells cells are then mixed with FFP and given back to patient..")
36
Therapy of TTP/HUS: Plasma Exchange 210 adult patients with TTP were treated with either plasma exchange or plasma alone. The 6 month survival was 78% for plasma exchange and 31% for plasma alone Study was confounded secondary to those who underwent plasma exchange received 3X the amount of plasma.

37
Steroids Seems to play a role in TTP therapy Usually 60-120 mg prednisone Slow taper when patients responds Some patients steroid sensitive

38
Other Therapies IVIG: not effective Vincristine: classic drug for resistance disease – 2 mg day 1, 4, 7, 10 Splenectomy: very controversial

39
Rituximab Appears to be useful for TTP No great RCT but abundant anecdotes – Faster remissions – Less relapses Give after exchange

40
Phase II Study 40 patients with acute TTP – 34 de novo, 6 relapse Rituximab within 3 days Compared to historical controls Blood 118:1746, 2011

41
Results No difference in number of exchanges No difference in hospital days – Was decreased in non-ICU patients Marked decrease in relapses – 10% from 57%

42
Bottom Line Rituximab useful in preventing relapses in antibody positive patients Acute role is undefined – Refractory cases?

43
Therapy of TTP/HUS- Plasma Exchange Complications – Bacteremia (10/71 patients) – Catheter Obstruction (7/71 patients) – Hemorrhage (2/71 patients) – Fungemia (2/71 patients) – Venous Thrombosis (2/71 patients) – Pneumothorax (2/71 patients)
 – Catheter Obstruction (7/71 patients) – Hemorrhage (2/71 patients) – Fungemia (2/71 patients) – Venous Thrombosis (2/71 patients) – Pneumothorax (2/71 patients)")
44
Treatment of TTP/HUS- Alternatives? 2 prospective trials evaluating the use of urokinase/heparin and dipyridamole/heparin were performed which no change in duration of renal failure, hemolysis, and thrombocytopenia. IVIG was used in a controlled trial (400mg/kg for 5 days) with no difference in hemolysis, thrombocytopenia, and creatinine at one year.
 with no difference in hemolysis, thrombocytopenia, and creatinine at one year..")
Similar presentations






 Richard L. Siegler M.D. Professor Emeritus University of Utah School of Medicine.>")




 Thrombocytopenic Purpura AM Report 5/25/2010.>")



 Nicola Davis.>")



