Download presentation
Presentation is loading. Please wait.

1
Dr Khin Mar Aye HOD Biochemistry Unit FOM

2
Objective Describe the role of kidney in Acid-Base Balance To discuss the tubular transport of H + and HCO 3 - Renal compensation for acid base disturbances

3
Acid Molecules containing H atoms that can release (donate) H ions in solutions eg HClH + + Cl - Strong acids : - Completely dissociate : (HCl, H 2 SO 4 ) Weak acid : - Partially dissociate : ( H 2 CO 3 )
 H ions in solutions eg HClH + + Cl - Strong acids : - Completely dissociate : (HCl, H 2 SO 4 ) Weak acid : - Partially dissociate : ( H 2 CO 3 )")
4
Base An Ion that accept a H ion (H + ) eg ( HCO 3 - ) HCO 3 - + H + H 2 CO 3 Buffers Substances that Neutralize acids or bases. Are mixtures of weak acids and their conjugate bases Tends to resist changes in pH when small amounts of acid (H + ) or base (OH - ) are added.
 or base (OH - ) are added..")
5
pH Is a negative log of hydrogen ion concentration (H + ) Henderson-Hasselbalch equation: pH = pK + log Base Acid pH = pK + log [A - ] [HA]
![pH Is a negative log of hydrogen ion concentration (H + ) Henderson-Hasselbalch equation: pH = pK + log Base Acid pH = pK + log [A - ] [HA]](http://images.slideplayer.com/35/10495061/slides/slide_5.jpg "pH Is a negative log of hydrogen ion concentration (H + ) Henderson-Hasselbalch equation: pH = pK + log Base Acid pH = pK + log [A - ] [HA]")
6
Types of acids in the body Volatile acid Can leave solution and enter the atmosphere e.g. carbonic acid Fixed acids Acids that do not leave solution e.g. sulfuric and phosphoric acids Organic acids Participants in or by-products of aerobic metabolism eg. Pyruvic acid, Oxaloacetic acid

7
Common acids Carbonic acid is most important factor affecting pH of ECF CO 2 reacts with water to form carbonic acid Inverse relationship between pH and concentration of CO 2 Sulfuric acid and phosphoric acid Generated during catabolism of amino acids Organic acids Metabolic byproducts such as lactic acid, ketone bodies

8
Acid-Base Balance Normal Arterial blood pH = 7.35 – 7.45 (7.4 ± 0.05) Arterial pH less than 6.8 or greater than 8.0 is not compatible with life Acidosis- Decrease in arterial pH ( <7.35 ) due to excess H + Alkalosis- Elevation in Arterial pH ( >7.45) due to excess base
 Arterial pH less than 6.8 or greater than 8.0 is not compatible with life Acidosis- Decrease in arterial pH ( <7.35 ) due to excess H + Alkalosis- Elevation in Arterial pH ( >7.45) due to excess base")
9
Normal value Arterial blood pH = 7.35 – 7.45 (7.4 ± 0.05) Normal H + concentration = 40nmol/L (or) 0.00004 mmol/L
 Normal H + concentration = 40nmol/L (or) mmol/L")
10
Sources of H + in the body Acids taken with foods Carbonic acid formation CO 2 + H 2 0 ↔ H 2 CO 3 H + + HCO3 - Inorganic acids produced during breakdown of nutrients( sulfuric acid & phosphoric acid ) Organic acids resulting from intermediary metabolism( lactic acid)
 Organic acids resulting from intermediary metabolism( lactic acid)")
11
How the body defends against fluctuations in pH? Three Systems in the body : 1) Buffers in blood 2) Respiration through the lungs 3) Excretion by the kidney Acid Base balance is maintain tight control within range 7.35 – 7.45
 Buffers in blood 2) Respiration through the lungs 3) Excretion by the kidney Acid Base balance is maintain tight control within range 7.35 –")
12
Lines of Defense against pH changes Chemical buffers:function almost immediately, take seconds to minutes Respiratory mechanisms:take minutes to hours Renal mechanisms: may take hours to days

13
Mechanisms of H + Regulation [H + ] is precisely regulated by 1. Body fluid chemical buffers (rapid but temporary) - bicarbonate- ammonia - proteins- phosphate Buffers regulate H+ ion concentration by take up or release hydrogen ion or hydroxyl ions 2. Lungs (rapid, eliminates CO 2 ) [H + ] ventilation CO 2 loss 3. Kidneys (slow, powerful); eliminates non-volatile acids - secretes H + - reabsorbs HCO 3 - - generates new HCO 3 -
![Mechanisms of H + Regulation [H + ] is precisely regulated by 1.](http://images.slideplayer.com/35/10495061/slides/slide_13.jpg "Body fluid chemical buffers (rapid but temporary) - bicarbonate- ammonia - proteins- phosphate Buffers regulate H+ ion concentration by take up or release hydrogen ion or hydroxyl ions 2. Lungs (rapid, eliminates CO 2 ) [H + ] ventilation CO 2 loss 3. Kidneys (slow, powerful); eliminates non-volatile acids - secretes H + - reabsorbs HCO generates new HCO 3 -.")
14
Blood Buffers These buffer systems serve as a first line of defense against changes in the acid-base balance : - HCO 3 - (Directly Regulated by Renal) - Protein / Hemoglobin - Phosphate
 - Protein / Hemoglobin - Phosphate")
15
Bicarbonate buffers Make up the body’s primary buffer system Is the most important buffer in extracellular fluid (blood & interstitial fluid) even though the concentration of the components are low and pK of the system is 6.1, which is not very close to normal extracellular fluid pH 7.4 Reason: The components of the system CO 2 is directly regulated by lungs and HCO 3 - is directly regulated by the kidneys.
 even though the concentration of the components are low and pK of the system is 6.1, which is not very close to normal extracellular fluid pH 7.4 Reason: The components of the system CO 2 is directly regulated by lungs and HCO 3 - is directly regulated by the kidneys.")
16
If pH falls: H + ion is buffered by HCO 3 - eg. H + + HCO 3 - H 2 CO 3 H 2 O+ CO 2 If pH rises OH - is buffered by H 2 CO 3 eg. OH - + H 2 CO 3 HCO 3 - + H 2 O Strong base becomes weak base

17
Protein buffers Most abundant buffers in the body. Works both inside and outside of cells Acidic and Basic Amino acid in plasma and cell protein act as buffers If pH climbs, the carboxyl group of amino acid acts as a weak acid If the pH drops, the amino group acts as a weak base Hb is an important buffer, binds with H + in red cells

18
Amino acid buffer

19
Phosphate buffers Both Intra and Extra cellular phosphate act as a buffer. It react with either acids or bases. But its role is minor compared to Hb or HCO 3 - Intracellular buffers are needed because H + doesn’t cross plasma membrane. Intracellular pH is more acidic ie 7.2 HPO 4 2- + H + H 2 PO 4 - H 2 PO4 - + OH - HPO4 2- + H 2 O

20
Buffer Systems in the Body Bicarbonate: most important ECF buffer HCO3 - + H + H 2 CO 3 Phosphate: important ICF and renal tubular buffer HPO 4 2- + H + H 2 PO 4 - Ammonia: important renal tubular buffer NH 3 + H + NH 4 + Proteins: important Intracellular buffers Largest buffer store in the body Hb - + H + HHb

21
Respiratory System Second line of defense against changes in pH within minutes. Carbon dioxide is an important by-product of metabolism and is constantly produced by cells The blood carries carbon dioxide to the lungs where it is exhaled. If the metabolic formation of CO 2 increases, the PCO 2 increases, and ventilation rate must increase. Normal PCO 2 level 35 – 45 mmHg

22
Hydrogen ion concentration can affect the ventilation rate Negative feedback loop of H + and alveolar ventilation Respiratory disease – such as emphysema, smokers lung Respiratory function is reduced & drive the body toward a state of respiratory acidosis.

23
Respiratory Regulation When breathing is increased the blood carbon dioxide level decreases and the blood becomes more BASE ( CO 2 washout pCO 2 Alkalosis) When breathing is decreased the blood carbon dioxide level increases and the blood becomes more ACIDIC ( CO 2 retention pCO 2 Acidosis) By adjusting the speed and depth of breathing, the respiratory control centers and lungs are able to regulate the blood pH minute by minute
 When breathing is decreased the blood carbon dioxide level increases and the blood becomes more ACIDIC ( CO 2 retention pCO 2 Acidosis) By adjusting the speed and depth of breathing, the respiratory control centers and lungs are able to regulate the blood pH minute by minute")
24
Renal Regulation of Acid Base Balance Kidney regulates Acid-Base balance by 3 following mechanisms: 1. Secretion of H + 2. Reabsorption of HCO 3 - 3. Production of new HCO 3 -

25
The kidneys control acid-base balance by excreting either an acidic or basic urine. The kidney filters large volumes of bicarbonate and the extent to which they are either excreted or reabsorbed determines the removal of “base” from the blood. The kidney secretes large numbers of H + into the tubule lumen, thus removing H + from the blood.

26
Mechanism of HCO 3 - Reabsorption and Na + - H + Exchange In Proximal Tubule and LOH

27
Excretion of H + & Generation of HCO 3 - This process occurs in the proximal convoluted tubules. The CO 2 combines with water to form carbonic acid, with the help of carbonic anhydrase. The H 2 CO 3 then ionizes to H + and bicarbonate. The hydrogen ions are secreted into the tubular lumen; in exchange for Na + reabsorbed. These Na + along with HCO 3 - will be reabsorbed into the blood. There is net excretion of hydrogen ions, and net generation of bicarbonate. This mechanism serves to increase the alkali reserve. H + is secreted via a Na-H counter-transport process, coupled to the active movement of Na + into the interstitial fluid via the basolateral Na-K ATPase.

28
Reabsorption of Bicarbonate Bicarbonate is filtered by the glomerulus. This is completely reabsorbed by the proximal convoluted tubule, so that the urine is normally bicarbonate free. The bicarbonate combines with H + in tubular fluid to form carbonic acid. It dissociates into water and CO 2. The CO 2 diffuses into the cell, which again combines with water to form carbonic acid. In the cell, it again ionizes to H + that is secreted into lumen in exchange for Na +. The HCO 3 - is reabsorbed into plasma along with Na +

29
HCO 3 - Reabsorption and H + Secretion in Distal and Collecting Tubules

30
The urine can only accommodate a small percentage of free H + protons in solution, so much of the H + to be excreted must complex with other buffering bases to facilitate its excretion. The major such buffers are phosphates and ammonia, combine with H + to get it out into the urine.

31
Phosphate as a Tubular Fluid Buffer There is a high concentration of phosphate in the tubular fluid. H + secreted to the tubular lumen reacts with Na 2 HP0 4 (basic phosphate) converted to NaH 2 P0 4 (acid phosphate) The advantage of this system is that very large quantities of hydrogen ions are excreted with minimum change in pH. If this system was not available, urinary pH will be so acidic, which will burn the tissues. The maximum limit of acidification is pH 4.5 (limiting pH) The buffering of H + by phosphate in the tubular fluid also contribute to the generation of new bicarbonate
 converted to NaH 2 P0 4 (acid phosphate) The advantage of this system is that very large quantities of hydrogen ions are excreted with minimum change in pH. If this system was not available, urinary pH will be so acidic, which will burn the tissues. The maximum limit of acidification is pH 4.5 (limiting pH) The buffering of H + by phosphate in the tubular fluid also contribute to the generation of new bicarbonate.")
32
Buffering of Secreted H + by Filtered phosphate (NaHPO 4 - ) and Generation of “New” HCO 3 - “New” HCO 3 -
 and Generation of New HCO 3 - New HCO 3 -")
33
Production and Secretion of NH 4 + and HCO 3 - by Proximal, Thick LOH, and Distal Tubules “New” HCO 3 -

34
Excretion of ammonium ions The Glutaminase present in the tubular cells can hydrolyse glutamine to ammonia and glutamic acid. Glutamine GlutaminaseGlutamic acid + NH 3 NH 3 diffuses into the luminal fluid and combines with H + to form NH 4 + NH 4 + is actively secreted into the lumen by sodium-NH 4 + pump. Ammonium (NH 4 + ) is produced from the cellular metabolism of glutamine in all nephron segments. For each glutamine molecule metabolized,2NH 4 + are produced and secreted and 2HCO 3 - are returned to the blood.
 is produced from the cellular metabolism of glutamine in all nephron segments. For each glutamine molecule metabolized,2NH 4 + are produced and secreted and 2HCO 3 - are returned to the blood..")
35
Buffering of Hydrogen Ion Secretion by Ammonia (NH 3 ) in the Collecting Tubules
 in the Collecting Tubules")
36
Titratable Acidity The term titratable acidity of urine refers to the number of milliliters of N/10 Na0H required to titrate 1 liter of urine to pH 7.4

37
Anion gap In plasma the number of electrical charges on cations equal with the number of charges on the anions. The difference between the sum of concentration of cations and the sum of on centration of anions is called “Anion gap” It represents usually unmeasured anions normally present in the plasma such as SO 4 -, PO 4 -, lactate and acetoacetate.

38
Sodium and potassium together account for 95% of the cations whereas chloride and bicarbonate account for only 86% of the anions. Only these electrolytes are commonly measured. The anion gap is calculated as the difference between (Na + +K + ) and (HC0 3 - + CI - ) Normally this is about 12.5 mmol/liter. The alteration in anion gap is extremely useful in the clinical assessment of patients with acid-base disorders.
 and (HC CI - ) Normally this is about 12.5 mmol/liter. The alteration in anion gap is extremely useful in the clinical assessment of patients with acid-base disorders..")
39
Acid base Imbalances Can arise from either respiratory dysfunction or metabolic disturbances Deviations divided into four general categories Respiratory acidosis Respiratory alkalosis Metabolic acidosis Metabolic alkalosis

40
Respiratory Acidosis Result of abnormal CO 2 retention arising from hypoventilation Possible causes Lung disease Depression of respiratory center by drugs or disease Nerve or muscle disorders that reduce respiratory muscle activity Holding breath

41
Respiratory Alkalosis Primarily due to excessive loss of CO 2 from body as result of – Fever, hyperventilation Possible causes Anxiety Aspirin poisoning Physiologic mechanisms at high altitude

42
Compensations of Respiratory Acidosis Chemical buffers immediately take up additional H + Kidneys are most important in compensating for respiratory acidosis Compensations of Respiratory Alkalosis Chemical buffer systems liberate H + If situation continues a few days, kidneys compensate by conserving H + and excreting more HCO 3 -

43
Metabolic Acidosis Includes all types of acidosis other than those caused by excess CO 2 in body fluids Causes Excessive loss of bicarbonate from intestines (Severe diarrhea, Fistula) Uncontrolled Diabetes mellitus (Diabetic ketoacidosis) Excessive acid accumulation (renal failure, Strenuous exercise) Uremic acidosis Important point – Plasma HCO 3 - level is
 Uncontrolled Diabetes mellitus (Diabetic ketoacidosis) Excessive acid accumulation (renal failure, Strenuous exercise) Uremic acidosis Important point – Plasma HCO 3 - level is")
44
Metabolic Alkalosis It occurs when there is loss of acid other than carbonic acid from ECF or an increase in base Important point – Plasma HCO 3 - level is Causes Vomiting Ingestion of alkaline drugs Potassium depletion Thiazide diuretics ( due to loss of Cl - )
")
45
Compensations of Metabolic Acidosis Buffers take up extra H + Lungs blow off additional H + generating CO 2 Kidneys excrete more H + and conserve more HCO 3 - Compensations of Metabolic Alkalosis Chemical buffer systems immediately liberate H + Ventilation is reduced If condition persists for several days, kidneys conserve H + and excrete excess HCO 3 - in the urine

46
Summary of Acid Base Abnormalities

47
Points to note Metabolic Acidosis occurs when the kidneys fail to excrete acids formed in the body, or there is excess ingestion of acids, or the loss of bases from the body. Renal Tubular Acidosis: due to a defect in H + secretion or HCO 3 - reabsroption. Diarrhea: Excess bicarbonate loss into the feces without time to reabsorb (most common cause). Diabetes mellitus: In the absence of normal glucose metabolism the cells metabolize fats and form acetoacetic acid, reducing pH, and inducing renal acid wasting.
. Diabetes mellitus: In the absence of normal glucose metabolism the cells metabolize fats and form acetoacetic acid, reducing pH, and inducing renal acid wasting..")
48
Chronic renal failure: decreased renal function results in acid build-up in the circulation and reduced HCO3 - reabsorption. Acid ingestion: toxins such as aspirin or methyl alcohol result in excess acid formation. Metabolic Alkalosis: occurs when there is excess retention of bicarbonate or excess loss of H + from the body. Diuretic therapy: many diuretics increase tubular flow, resulting in increased sodium load, increased Na reabsorption and therefore increased bicarbonate reabsorption.

49
Excess Aldosterone: which promotes excess sodium reabsorption and stimulates H + secretion. Vomiting: loss of the acidic contents of the stomach creates a depletion of H + which is compensated for by removing more H + from the circulation. Ingestion of alkaline drugs such as sodium bicarbonate used for upset stomachs and ulcers.

50
Renal Compensations for Acid Base Disorders Acidosis: - increased H + secretion - increased HCO 3 - reabsorption - production of new HCO 3 - Alkalosis: - decreased H + secretion - decreased HCO 3 - reabsorption - loss of HCO 3 - in urine

51
Analysis of Acid Base Disorders

56
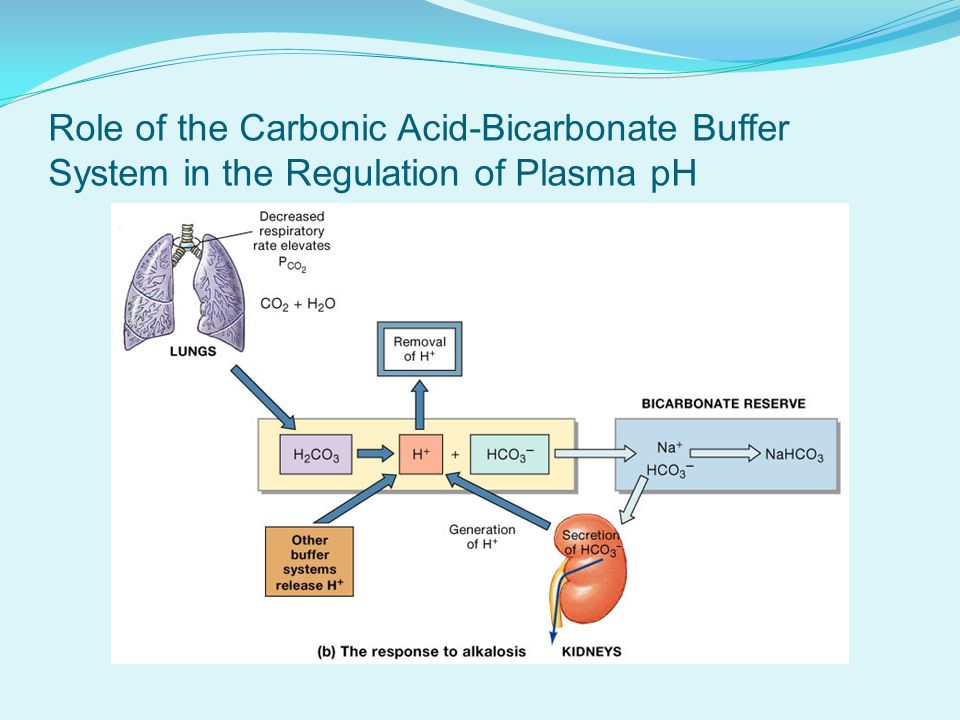
Role of the Carbonic Acid-Bicarbonate Buffer System in the Regulation of Plasma pH

58
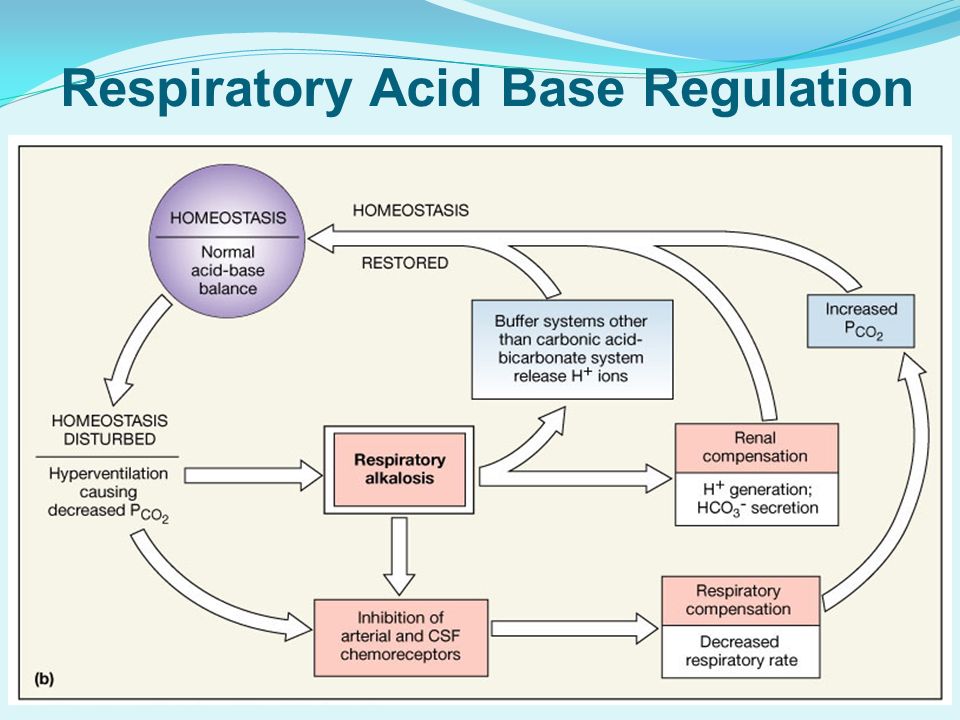
Respiratory Acid Base Regulation

60
Response to Metabolic Acidosis

61
Response to Metabolic Alkalosis

62
A Diagnostic Chart for Acid Base Disorders

Similar presentations












![1. pH = - log [H + ] H + is really a proton Range is from 0 - 14 If [H + ] is high, the solution is acidic; pH < 7 If [H + ] is low, the solution.](/15/4651316/big_thumb.jpg "1. pH = - log [H + ] H + is really a proton Range is from 0 - 14 If [H + ] is high, the solution is acidic; pH < 7 If [H + ] is low, the solution.>")
![H + Homeostasis by the Kidney. H + Homeostasis Goal: To maintain a plasma (ECF) pH of approximately 7.4 (equivalent to [H + ] = 40 nmol/L Action needed:](/15/4651439/big_thumb.jpg "H + Homeostasis by the Kidney. H + Homeostasis Goal: To maintain a plasma (ECF) pH of approximately 7.4 (equivalent to [H + ] = 40 nmol/L Action needed:>")






 H + concentration in the body.>")
![Renal Acid-Base Balance. Acid An acid is when hydrogen ions accumulate in a solution. It becomes more acidic [H+] increases = more acidity CO 2 is an.](/20/5962628/big_thumb.jpg "Renal Acid-Base Balance. Acid An acid is when hydrogen ions accumulate in a solution. It becomes more acidic [H+] increases = more acidity CO 2 is an.>")
 concentration. More H + = more acidic = lower.>")
