Download presentation
Presentation is loading. Please wait.

1
PORTABLE MONITORING FOR THE DIAGNOSIS OF OBSTRUCTIVE SLEEP APNEA ADNAN ABBASI, MBBS, MPH

2
Conflict of interest None Disclosure None

3
OBJECTIVES Understand the need of Portable Monitoring (PM) and Home Sleep Testing (HST) in evaluation of obstructive sleep apnea (OSA) in current practice model Review technology for PM for diagnosis of OSA Review algorithmic approach to diagnosis and management of OSA using PM and auto-PAP Identify patients in whom HST can be effective
 and Home Sleep Testing (HST) in evaluation of obstructive sleep apnea (OSA) in current practice model Review technology for PM for diagnosis of OSA Review algorithmic approach to diagnosis and management of OSA using PM and auto-PAP Identify patients in whom HST can be effective")
4
EPIDEMIOLOGY OF SLEEP-DISORDERED BREATHING Prevalence of OSA (defined as an apnea-hypopnea index >5 events per hour) 33.9% in men and 17.4% in women OSA syndrome (OSA + excessive daytime sleepiness) is 14.3% in men and 5% in women Increasing rates of obesity Peppard PE. Am J Epidemiol. 2013 May 1;177(9):1006-14 Young T. N Engl J Med. 1993 Apr 29;328(17):1230-5 Al Lawati NM. Prog Cardiovasc Dis. 2009 Jan-Feb;51(4):285-93
: Young T. N Engl J Med Apr 29;328(17): Al Lawati NM. Prog Cardiovasc Dis Jan-Feb;51(4):")
5
CONSEQUENCES OF UNTREATED SLEEP APNEA Excessive daytime sleepiness Decreased workplace productivity Car crashes Systemic hypertension Cardiovascular disease Increased mortality Mulgrew AT. Sleep Med. 2007 Dec;9(1):42-53 Marin JM. Lancet 2007; 365:1046-1053 Peppard PE. NEJM 2000; 342:1378-1384 Barbe F. Am Jr Respir Crit Care Med. 1998;158:18-22
:42-53 Marin JM. Lancet 2007; 365: Peppard PE. NEJM 2000; 342: Barbe F. Am Jr Respir Crit Care Med. 1998;158:")
6
DIAGNOSIS OF SLEEP APNEA Historically, in-laboratory attended polysomnography (PSG) has been considered as the preferred method High cost Long wait times
 has been considered as the preferred method High cost Long wait times")
7
HOME TESTING MODEL In the last 15 years, there is growing interest in algorithmic approach that bypass in-laboratory sleep studies

8
TERMINOLOGY FOR TECHNOLOGY USED TO DIAGNOSE SLEEP APNEA Level 1: In-laboratory attended – EEG, chin EMG, ECG, measure of airflow, respiratory effort, oxygen saturation Level 2: Same as level 1, but performed outside the sleep laboratory Level 3: minimum of 4 parameters including oxygen saturation, measurement of heart rate or ECG, and at least two channels assessing respiration (e.g., respiratory movement and airflow) Level 4: one or two channels – nocturnal oximetry or nasal airflow alone Ferber R. Sleep. 1994;17(4):378-392
:")
10
REVISED CLASSIFICATION SYSTEM FOR PM- SCOPER S: Sleep C: Cardiac measure O: Oximetry P: Position E: Effort R: Respiration Collop NA. J Clin Sleep Med 2011;7(5):531-548
:")
11
IN-LABORATORY PSG VS. HST Most PM devices lack ability to differentiate awake from sleep state Total recording time is used as denominator for calculating AHI (Respiratory Event Index) PM underestimates severity of OSA Several PM are able to estimate total sleep time Limited EEG 1 or 2 leads Lack of head movement Actigraphy J Clin Sleep Med 2007;3(7):737-747
 PM underestimates severity of OSA Several PM are able to estimate total sleep time Limited EEG 1 or 2 leads Lack of head movement Actigraphy J Clin Sleep Med 2007;3(7):")
13
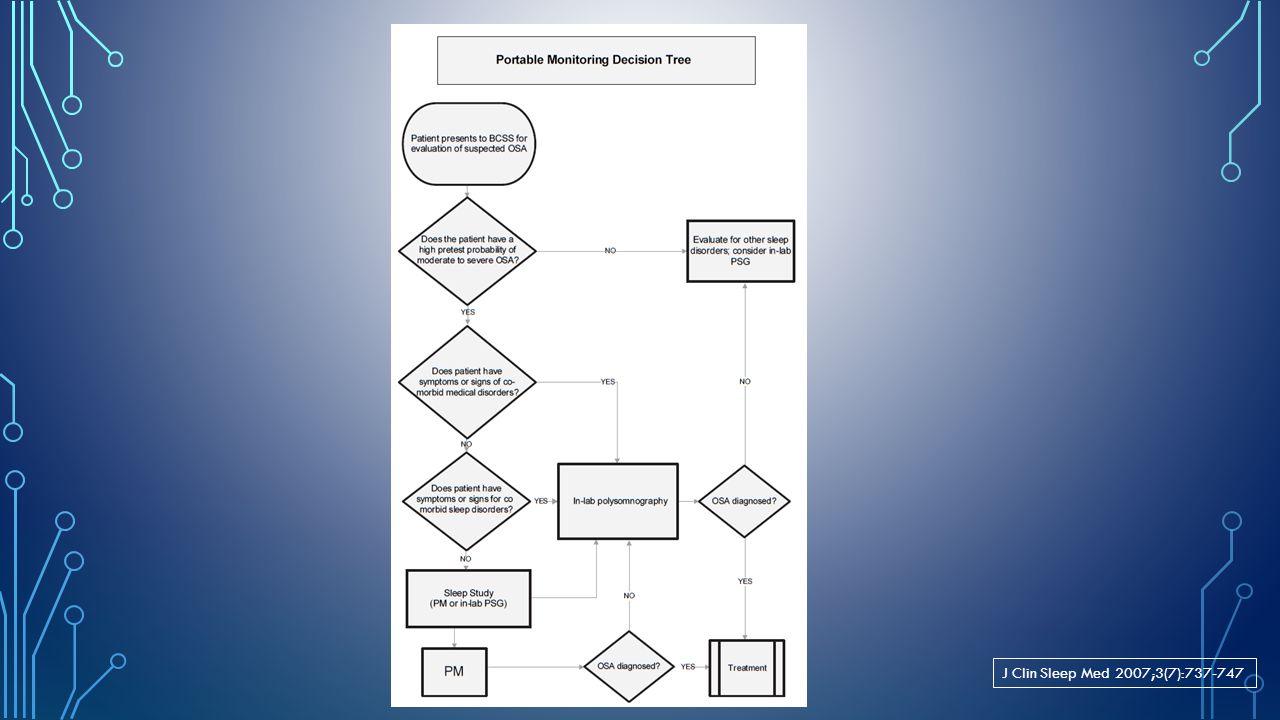
INDICATIONS FOR PORTABLE MONITORING PM for diagnosis of OSA should be performed only in conjunction with a comprehensive sleep evaluation. Clinical sleep evaluations using PM must be supervised by a Board Certified (or Board eligible) Sleep Specialist. In the absence of a comprehensive sleep evaluation, there is no indication for the use of PM. J Clin Sleep Med 2007;3(7):737-747
 Sleep Specialist. In the absence of a comprehensive sleep evaluation, there is no indication for the use of PM. J Clin Sleep Med 2007;3(7):")
14
INDICATIONS FOR PORTABLE MONITORING PM may be used as an alternative to PSG for diagnosis of OSA in patients with a high pre-test probability of moderate to severe OSA. J Clin Sleep Med 2007;3(7):737-747
:")
15
PM IS NOT APPROPRIATE FOR THE DIAGNOSIS OF OSA Patients with significant comorbid medical such as moderate to severe pulmonary disease, neuromuscular disease, or congestive heart failure. Patients suspected of having other sleep disorders, including central sleep apnea, periodic limb movement disorder (PLMD), insomnia, parasomnias, circadian rhythm disorders, or narcolepsy. For general screening of asymptomatic populations. J Clin Sleep Med 2007;3(7):737-747
, insomnia, parasomnias, circadian rhythm disorders, or narcolepsy. For general screening of asymptomatic populations. J Clin Sleep Med 2007;3(7):")
16
PM MAY BE INDICATED PM may be indicated for the diagnosis of OSA in patients for whom in-laboratory PSG is not possible by virtue of immobility, safety, or critical illness. PM may be indicated to monitor the response of non-CPAP treatments for OSA, including oral appliances, upper airway surgery, and weight loss. J Clin Sleep Med 2007;3(7):737-747
:")
17
TECHNOLOGY OF PORTABLE MONITOR At a minimum, the PMs must record airflow, respiratory effort, and blood oxygenation. The type of biosensors that are used to monitor these parameters for in-laboratory PSG are recommended for use in PMs. The sensor to detect apnea is an oronasal thermal sensor and to detect hypopnea is a nasal pressure transducer. Ideally, PMs should use both sensor types. J Clin Sleep Med 2007;3(7):737-747
:")
18
TECHNOLOGY OF PORTABLE MONITOR Ideally the sensor for identification of respiratory effort is either calibrated or uncalibrated inductance plethesmography. The sensor for detection of blood oxygen is pulse oximetry with appropriate signal averaging time and accommodation for motion artifact. J Clin Sleep Med 2007;3(7):737-747
:")
19
METHODOLOGY FOR PORTABLE MONITORING Under the auspices of an AASM accredited comprehensive Sleep Medicine Program with policies and procedures for sensor application, scoring, and interpretation of PM. An experienced sleep technician, sleep technologist, or appropriately trained healthcare practitioner must perform the application of PM or directly educate the patient in the correct application of sensors. J Clin Sleep Med 2007;3(7):737-747
:")
20
METHODOLOGY FOR PORTABLE MONITORING PM devices must allow for the display of raw data for manual scoring or editing of automated scoring by a trained and qualified sleep technician/technologist. Evaluation of PM data must include review of the raw data by a Board Certified (or Board eligible) Sleep Specialist. Scoring criteria should be consistent with the current published AASM standards for scoring of apneas and hypopneas. J Clin Sleep Med 2007;3(7):737-747
 Sleep Specialist. Scoring criteria should be consistent with the current published AASM standards for scoring of apneas and hypopneas. J Clin Sleep Med 2007;3(7):")
21
METHODOLOGY FOR PORTABLE MONITORING Due to the known rate of false negative PM tests, in-laboratory PSG should be performed in cases where PM is technically inadequate or fails to establish the diagnosis of OSA in patients with a high pre-test probability. A follow-up visit with a physician or other appropriately trained and supervised health provider should be performed on all patients undergoing PM to discuss the results of the test. J Clin Sleep Med 2007;3(7):737-747
:")
23
CMS DECISION MEMO FOR SLEEP TESTING FOR OSA In 2009 CMS approved coverage for PAP for patients diagnosed with sleep disordered breathing using PM Devices covered for diagnosis of OSA: Type I sleep testing device -if performed attended in a sleep lab facility Type II or a Type III sleep testing device if performed unattended in or out of a sleep lab facility or attended in a sleep lab facility https://www.cms.gov/medicare-coverage-database/overview-and-quick- search.aspx?FriendlyError=InvalidNCAIDhttps://www.cms.gov/medicare-coverage-database/overview-and-quick- search.aspx?FriendlyError=InvalidNCAID Document ID: CAG-00405N

24
CMS DECISION MEMO FOR SLEEP TESTING FOR OSA A Type IV sleep testing device measuring three or more channels, one of which is airflow if performed unattended in or out of a sleep lab facility or attended in a sleep lab facility. A sleep testing device measuring three or more channels that include actigraphy, oximetry, and peripheral arterial tone is covered if performed unattended in or out of a sleep lab facility or attended in a sleep lab facility. https://www.cms.gov/medicare-coverage-database/overview-and-quick- search.aspx?FriendlyError=InvalidNCAIDhttps://www.cms.gov/medicare-coverage-database/overview-and-quick- search.aspx?FriendlyError=InvalidNCAID Document ID: CAG-00405N

25
PRE-TEST CLINICAL ASSESSMENT OF OSA History and physical examination Assessment of excessive daytime sleepiness- Epworth Sleepiness Scale Review of overnight oximetry Sleep Questionnaires STOP-BANG Questionnaire Berlin Questionnaire Wisconsin Questionnaire

26
STOP-BANG QUESTIONNAIRE S: Snoring T: Tired O: Observed P: Pressure (Hypertension) B: Body Mass Index > 35 Kg/M 2 A: Age > 50 years N: Neck circumference >17” in M >16” in F G: Gender= Male Low Risk : Yes to 0 - 2 questions Intermediate Risk : Yes to 3 - 4 questions High Risk : Yes to 5 - 8 questions or Yes to 2 or more of 4 STOP questions + male gender or Yes to 2 or more of 4 STOP questions + BMI > 35kg/m 2 or Yes to 2 or more of 4 STOP questions + neck circumference > 17 inches in M or 16 inches in F http://www.stopbang.ca/osa/screening.php
 B: Body Mass Index > 35 Kg/M 2 A: Age > 50 years N: Neck circumference >17 in M >16 in F G: Gender= Male Low Risk : Yes to questions Intermediate Risk : Yes to questions High Risk : Yes to questions or Yes to 2 or more of 4 STOP questions + male gender or Yes to 2 or more of 4 STOP questions + BMI > 35kg/m 2 or Yes to 2 or more of 4 STOP questions + neck circumference > 17 inches in M or 16 inches in F")
28
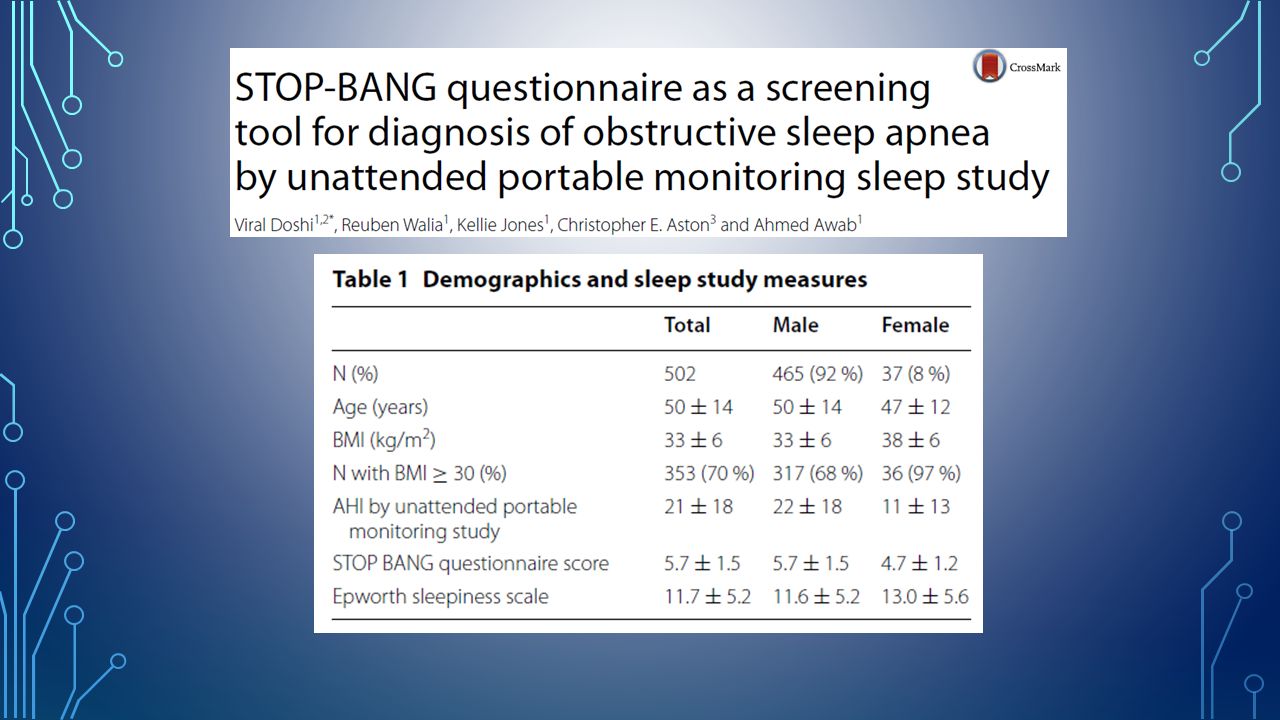
Doshi V. Springerplus. 2015 Dec 22;4:795

29
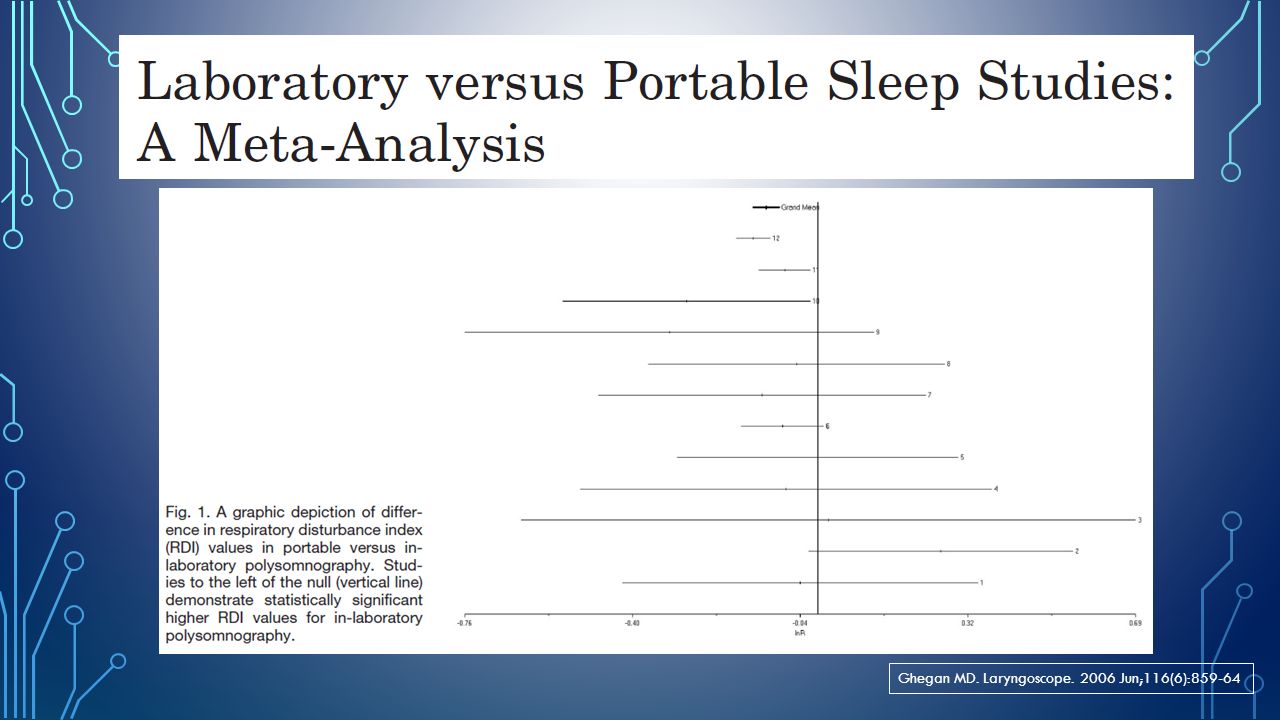
Ghegan MD. Laryngoscope. 2006 Jun;116(6):859-64
:859-64")
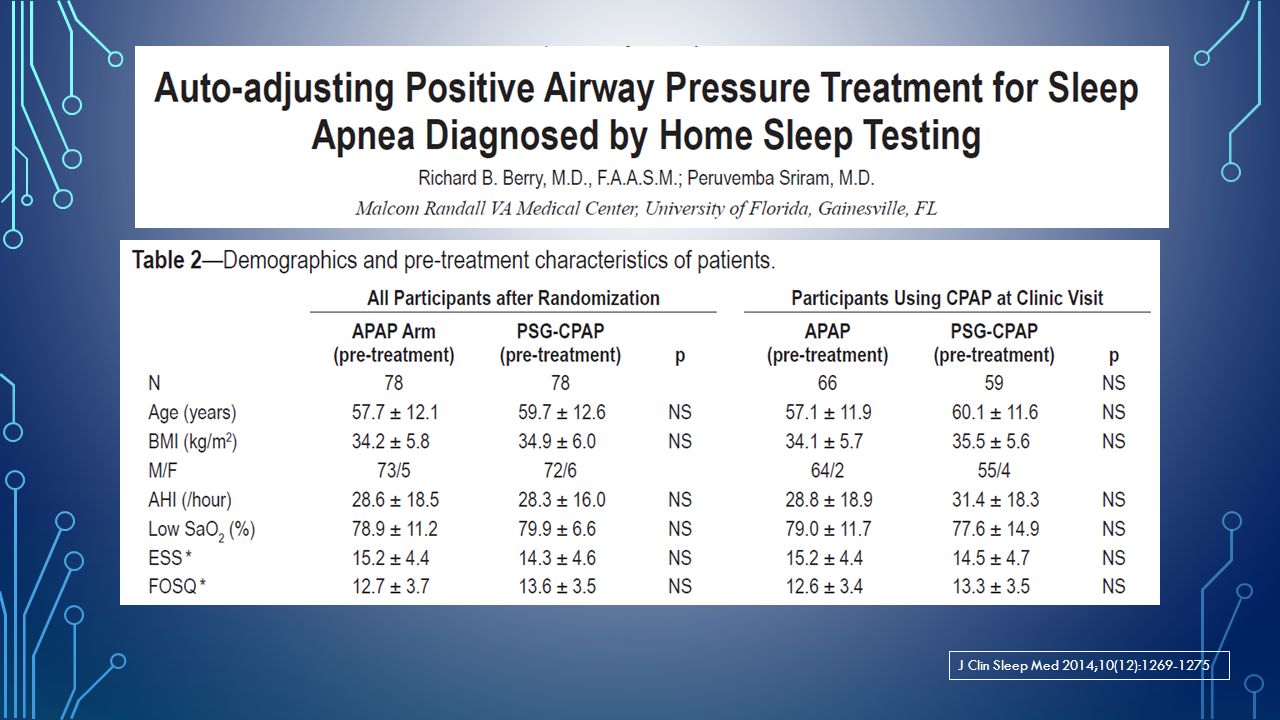
31
J Clin Sleep Med 2014;10(12):1269-1275
:")
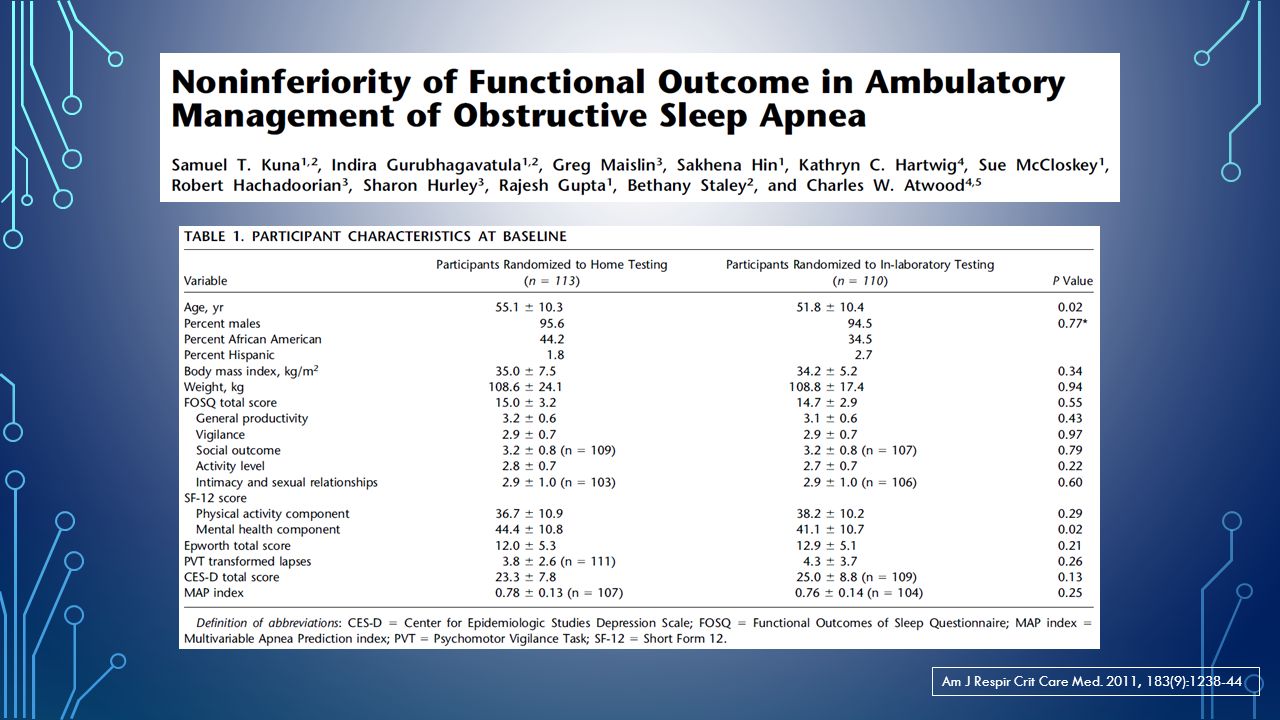
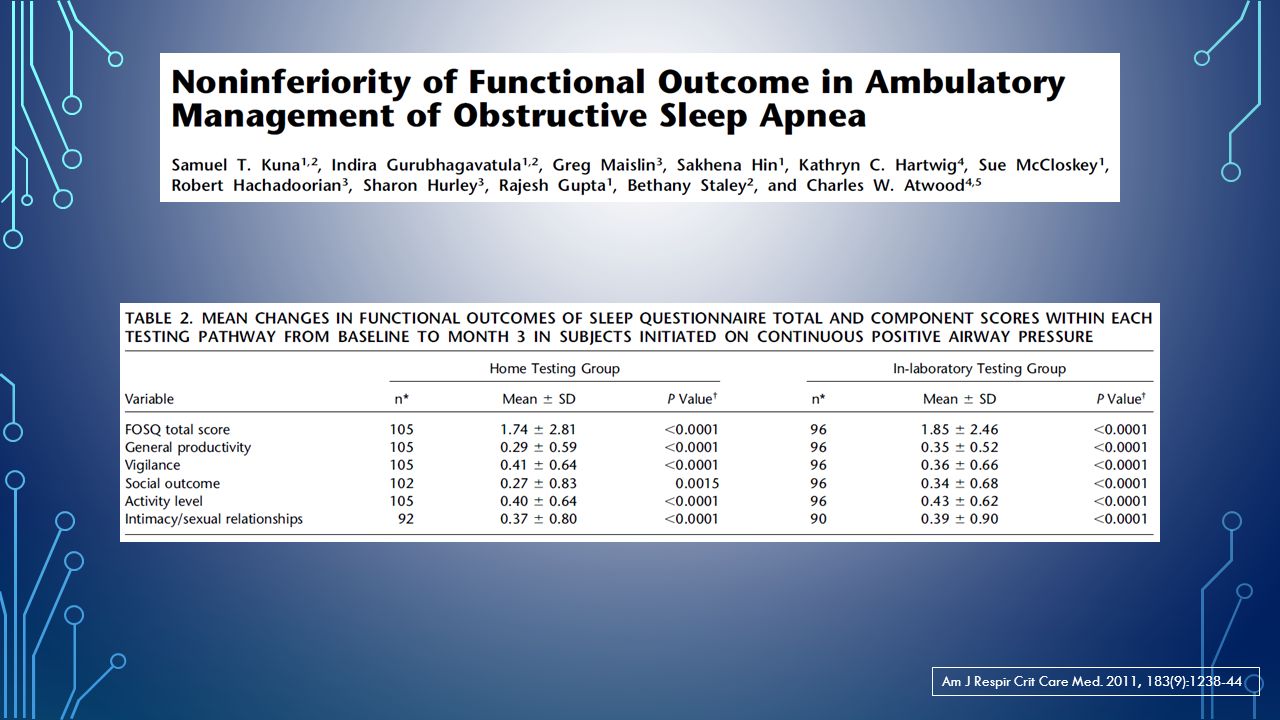
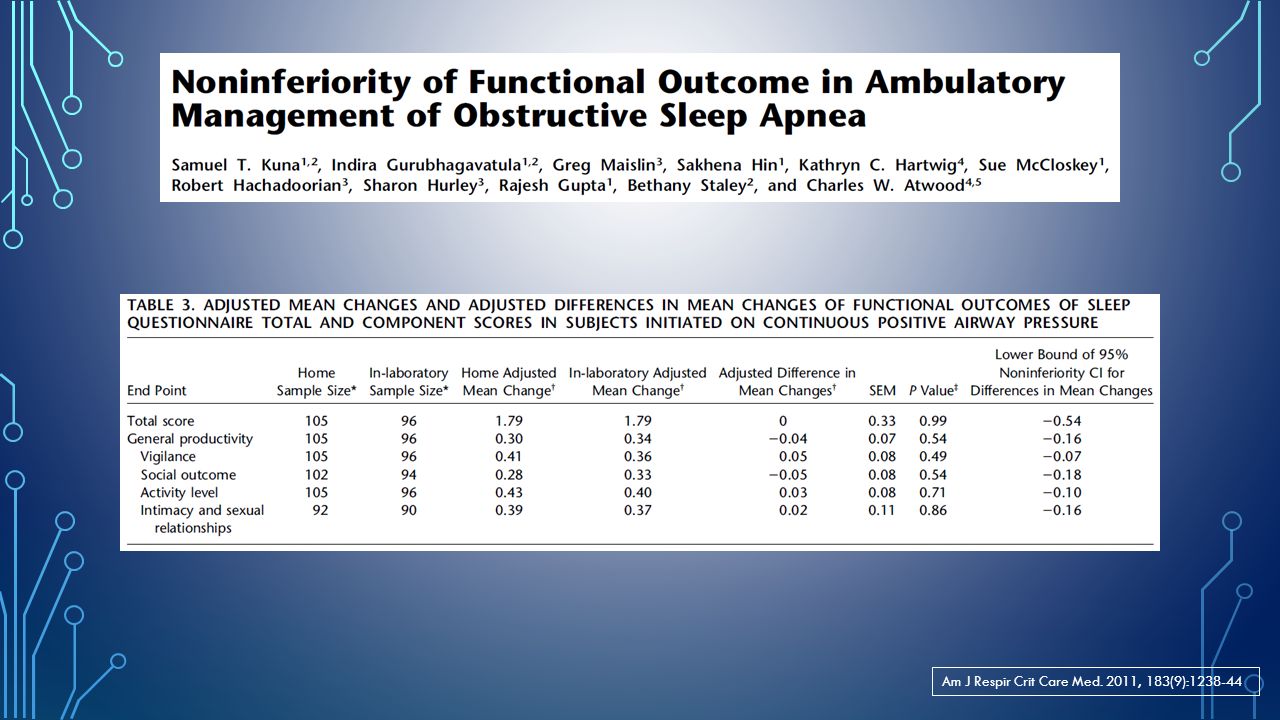
35
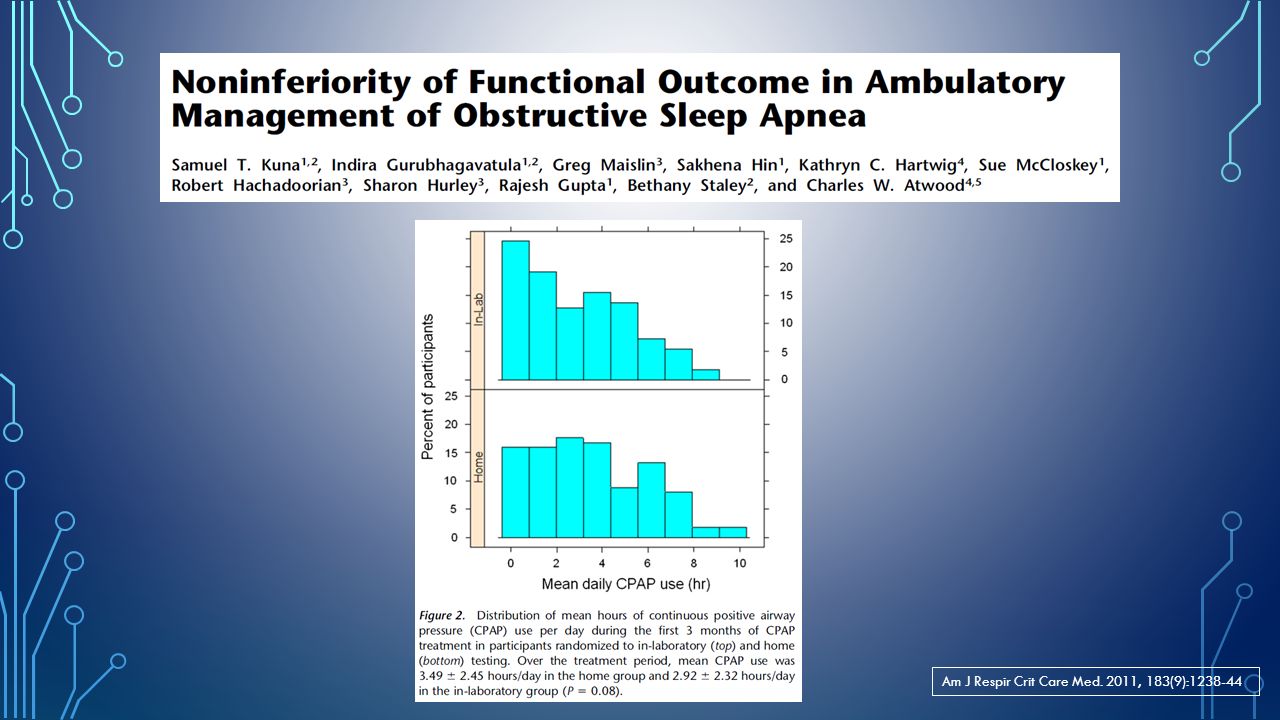
Am J Respir Crit Care Med. 2011, 183(9):1238-44
:")
40
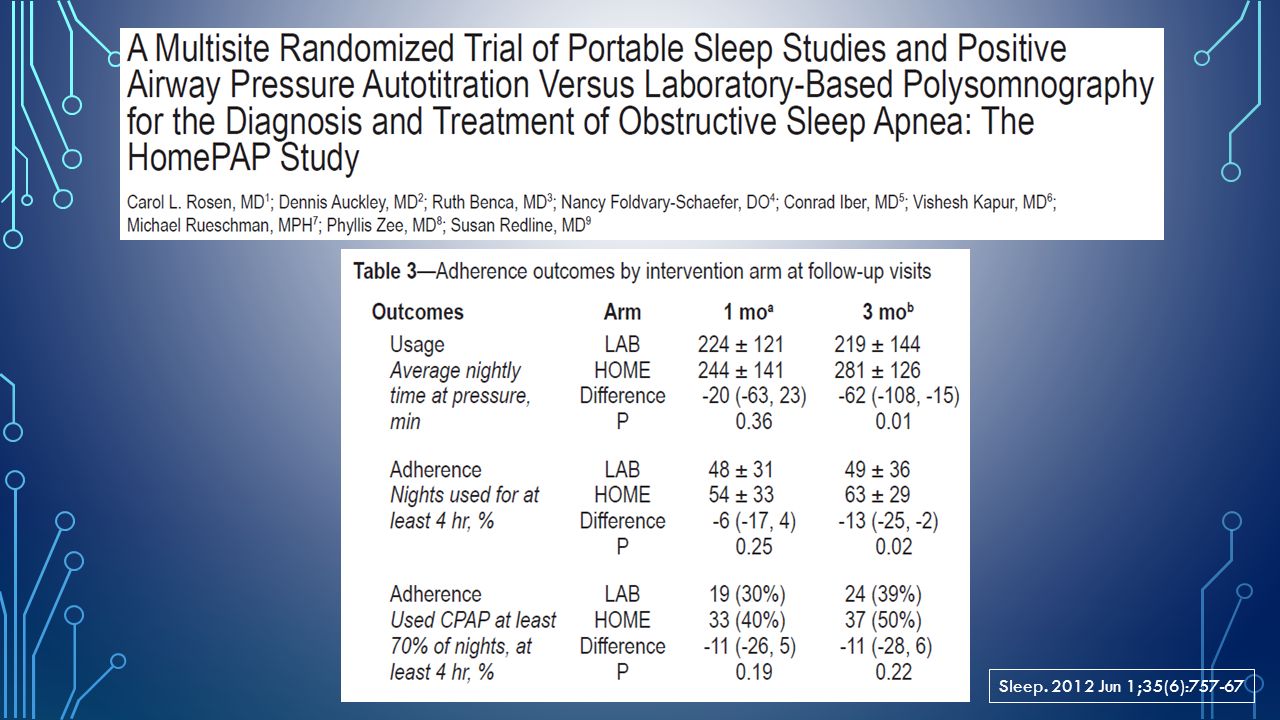
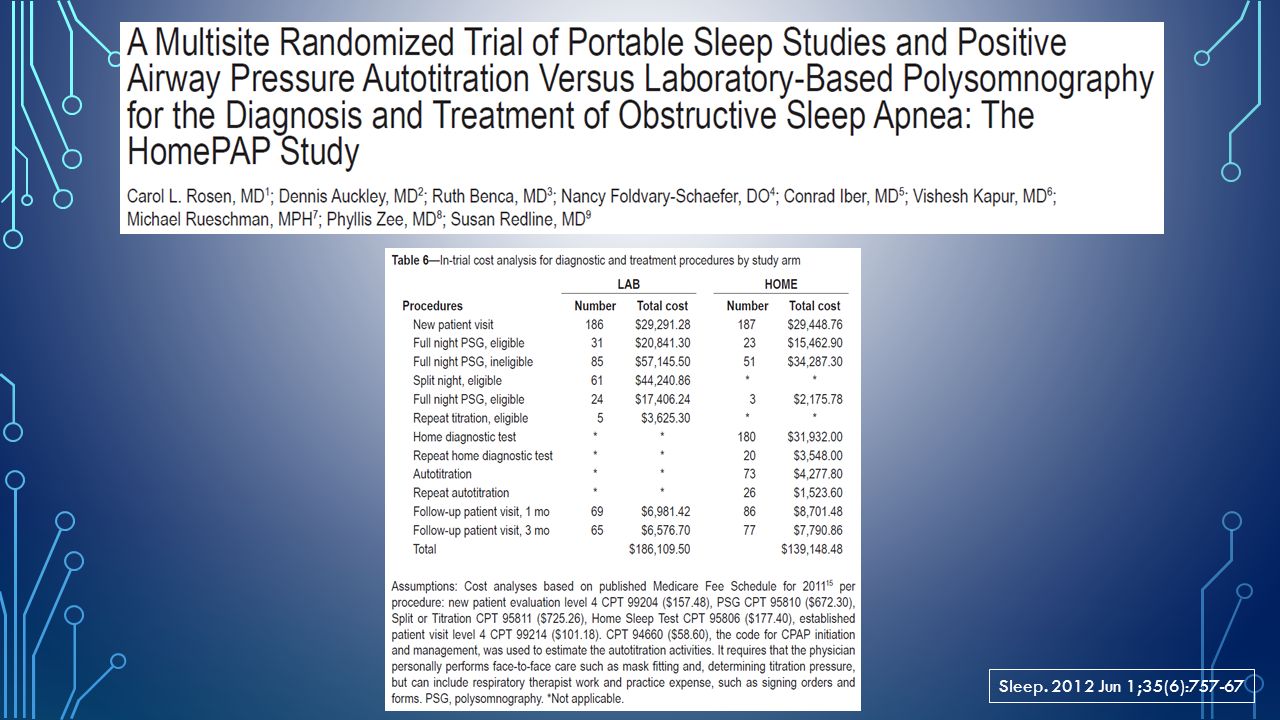
Sleep. 2012 Jun 1;35(6):757-67
:757-67")
43
Take home messages… PM has become an important tool in the armamentarium used to manage sleep disordered breathing. In out-patient setting, PM/HST algorithms are non-inferior to laboratory-based diagnosis of OSA and titration of PAP therapy. For appropriately selected patients- with moderate to high clinical suspicion of obstructive sleep apnea and without significant co-morbid conditions, HST can be used effectively to diagnose and auto-PAP to treat OSA. Patients with normal AHI on HST but high pre-test clinical suspicion for OSA should undergo in-laboratory PSG.

44
Cooksey JA. Chest 2016; 149(4):1074-1081
:")
Similar presentations





”>")





? Isadore Tarantino 1, Tim Quinn 1, Larry Dall 1, Nurry.>")










