Download presentation
Presentation is loading. Please wait.

1
Heart Failure Dr Nidhi Bhargava

2
Cardiac Failure Clinical syndrome that can result from any structural or functional cardiac disorder that impairs the ability of the ventricle to fill or eject blood.(AHA/ACC HF guidelines 2001)
")
3
Economic burden- 1.2-2% of all healthcare costs and 60-75% of these costs relate to hospital burden NYHA classes 1-1V All class HF mortality- 50% in 5 years NYHA Class 1V- 1 year survival -50%

4
NYHA (New York Heart Association Classification) Class 1 Cardiac disease but no limitation in ordinary physical activity, e.g. no SOB when walking, climbing stairs etc. Class 2 Mild symptoms ( mild SOB and or angina) and slight limitation during ordinary activity Class 3 Marked limitation in activity due to symptoms, even during less than ordinary activity, e.g. walking short distances (20-100 m) Comfortable only at rest. Class 4 Severe Limitations. Experiences symptoms even at rest. Mostly bedbound patients
 and slight limitation during ordinary activity Class 3 Marked limitation in activity due to symptoms, even during less than ordinary activity, e.g. walking short distances ( m) Comfortable only at rest. Class 4 Severe Limitations. Experiences symptoms even at rest. Mostly bedbound patients.")
5
Causes of death 40% Sudden 50% pump failure 30-40% are in NYHA class 111- 1V Rehospitalisation rates 2% at 2 days 20% at 1 month 50% at 6 months

6
Causes 1. Myocardial Dysfunction (IHD, DCM) 2. Volume overload (AR, MR) 3. Obstruction (AS, MS, HOCM) 4. Diastolic Dysfunction (Constriction) 5. Mechanical Problems (LV aneurysm) 6. Rhythm Disturbance (AF) 7. High Output (anaemia, shunts, thyrotoxicosis) 8. IHD and HT-most common disease processes often in combination causing myocardial damage
 4. Diastolic Dysfunction (Constriction) 5. Mechanical Problems (LV aneurysm) 6. Rhythm Disturbance (AF) 7. High Output (anaemia, shunts, thyrotoxicosis) 8. IHD and HT-most common disease processes often in combination causing myocardial damage.")
7
Pathophysiology Large MI CO BP Compensatory Mechanisms Neuroendocrine activation Renin angiotensin Aldosterone

8
Pathophysiology Neuroendocrine Activation- Increased HR and contractility Aldosterone System-Na retention and hence water retention Renin angiotensin system- vasoconstriction

9
Pathophysiology An increase in LVED volume Starling’s law- increased LVED volume and hence increased stroke volume Hence increased stress on the left ventricular wall- further thinning of the infarcted wall and expansion of infarcted region The normal wall can compensate for the rest of infarcted area- compensatory mechanism otherwise LV dilatation and LVSD-worse than original infarct

10
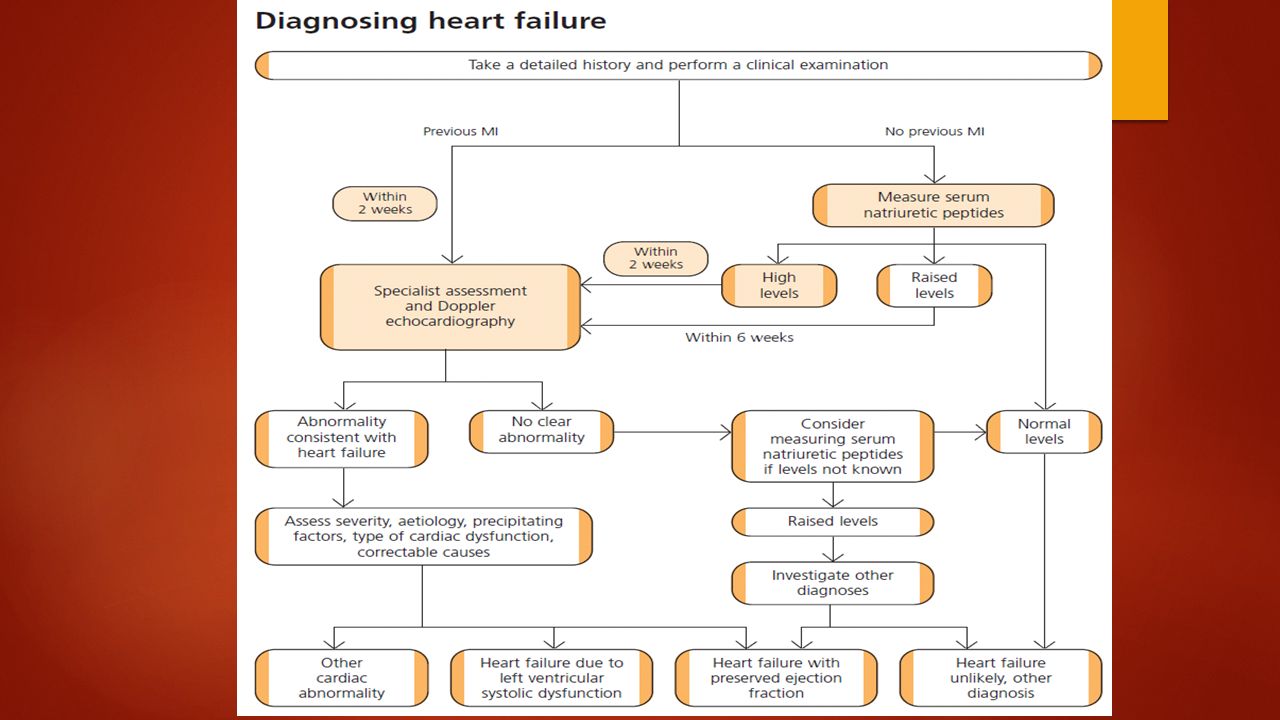
Signs and Symptoms of Heart failure ESC guidelines Essential features-SOB, ankle swelling, objective evidence of cardiac dysfunction at rest using echo Non essential features- Response to treatment directed at HF (if diagnosis in doubt)
")
11
Symptoms 1. Exertional Dyspnoea 2. Orthopnoea 3. PND 4. Ankle swelling 5. Anorexia and wt loss 6. Cold peripheries 7. Tiredness

12
Signs Tachycardia Hypotension Raised JVP 3 rd heart sound PSM of MR Basal crackles Ankle oedema

14
Investigations ECG- If normal chances of LVSD are very low (<5%)- LBBB, Q waves, non specific ST/T waves changes CXR- cardiomegaly, Pulmonary oedema BNP- elevated in both systolic and diastolic dysfunction, results affected by obesity, diuretics and ACEi, blockers, spironolactone-all decerase the levels. LVH, ischaemia and tachycardia, PE, eGFR < 60, COPD, sepsis will increase the levels Echo-confirmatory test- systolic dysfunction/any valvular disease/ischaemic aetiology or regional wall motion abnormality/diastolic dysfunction Nuclear imaging Stress echocardiography Cardiac catheterisation Lung function tests

16
Treatment Acute HF Sit up, high dose O2, i/v diamorphine, i/v GTN, intubation Treat intercurrent infection Systolic BP<80 –poor prognosis Ionotropes to increase BP and help orgn perfusion

17
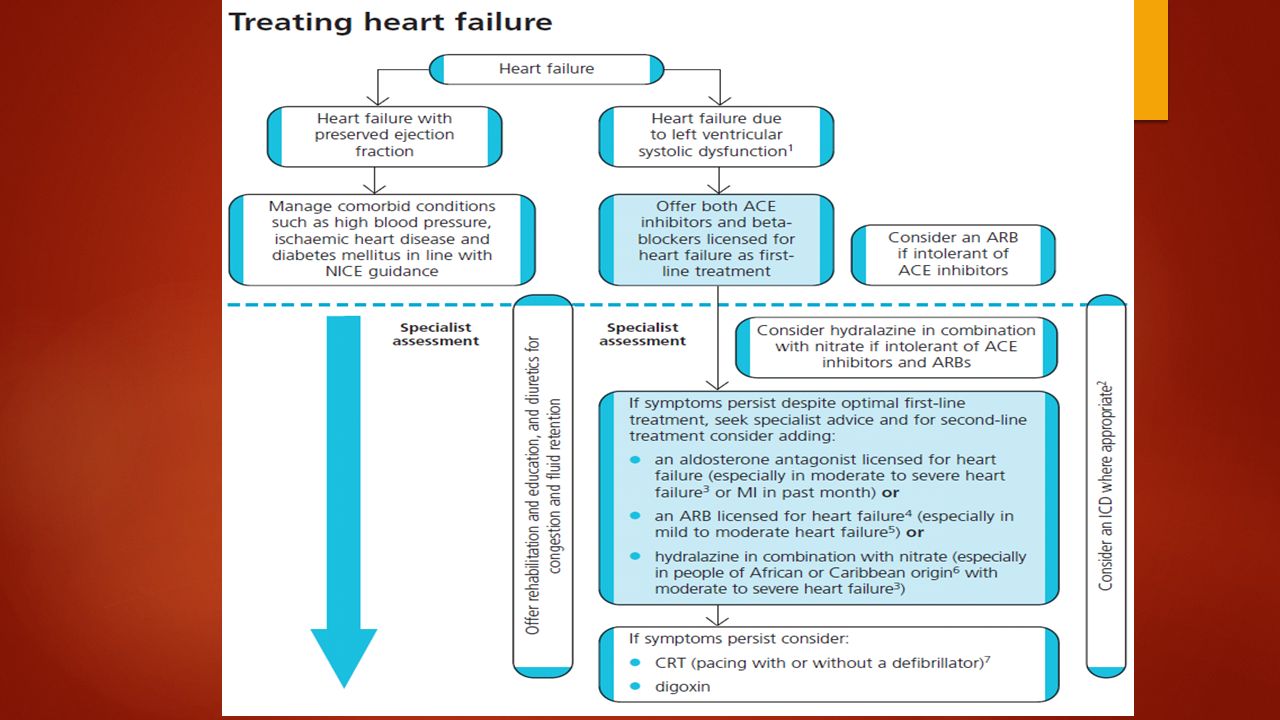
Treatment Chronic HF Non pharmacological- restrict salt and fluid intake, encourage exercise, decrease or abstain from alcohol Flu vaccination Tight BP control Loop diuretcis-frusemide 40-80mgs or bumetanide 1-2mgs

18
Non Coronary Interventions Pacing- broad QRS+ LBBB Defibrillators-ventricular arrhythmias Valvular surgery-Mitral valve repair Heart Transplant- otherwise fit individuals Left ventricular assist devices- as a bridge to transplantation

19
Treatment ACEi – improve prognosis and symptoms, optimise dose, slow titration every 2 weeks with UEs monitoring ARBs- role not confirmed (to be used if unable to tolerate ACEi) Hydralazines and nitrates- improve diagnosis and prognosis (consensus study), first line or 2 nd line (NYHA 111-1V), Africo carribean population blockers- Improve prognosis and symptoms. Assess HR and BP at each titration, use those licensed for HF (even in pts with COPD) Spironolactone- NYHA 111-1V, monitor K levels and eGFR Ivabradine- in pts with NYHA class 2-4 stable CHF with systolic dysfunction, in sinus rhythm, HR ≥ 75/min and given in combination with other HF treatment or when beta blocker is contraindicated, LVEF ≤ 35% aftre stabilisation with other treatement for at least 4 weeks.
 Spironolactone- NYHA 111-1V, monitor K levels and eGFR Ivabradine- in pts with NYHA class 2-4 stable CHF with systolic dysfunction, in sinus rhythm, HR ≥ 75/min and given in combination with other HF treatment or when beta blocker is contraindicated, LVEF ≤ 35% aftre stabilisation with other treatement for at least 4 weeks..")
20
Treatment Rehabilatation- supervised group exercises- rehab programme Psychological and educational support-role of community heart failure nurses

21
CRT (cardiac resynchronisation therapy) Moderate to severe LVSD NYHA 111-1V No revascularisation or surgery strategy Stable and optimal medical regime QRS ≥ 130ms EF≤ 35% LVED dimension ≥ 55mm
 Moderate to severe LVSD NYHA 111-1V No revascularisation or surgery strategy Stable and optimal medical regime QRS ≥ 130ms EF≤ 35% LVED dimension ≥ 55mm")
22
Case 1 73 years old female Recent onset of orthopnoea PMH-HT diagnosed 3 years ago Medication-atenolol o/e- b/l basal crepts ? Suspected diagnosis Tests needed to confirm diagnosis Treatment

23
Case 2 71 years old male P/C- breathlessness and fatigue, gradually worsening PMH- Type 1 DM, angina o/e- irregular pulse (possibly AF), low volume ? Heart failure Tests for confirmation

24
Case 3 68 years old female P/C- exertional breathlessness, ankle swelling, cough PMH- Type 2 DM o/e- ankle oedema, high BP and 2cms hepatomegaly ? Heart failure Tests Treatment

25
Case 4 80 years old female P/C- fatigue, weight loss, feels stomach always bloated PMH-chronic bronchitis o/e- raised JVP, PSM in the lower sternal edge, 3 rd HS, ascites ? Heart failure Tests

26
Case 5 62 years old male P/C- breathlessness and orthopnoea PMH-COPD o/e- b/l basal crepitations and tachycardia ? Exacerbation of COPD or possible heart failure Tests

27
Case 6 65 years old female of Africo-Caribbean ethinicity P/C- 3/52 of exertional breathlessness PMH- Hypertension and obesity o/e- b/l basal crepitations, laterally displaced apical impulse ? Heart failure Tests Treatment After 6 months pt presents again with worsening breathlessness Treatment Pt returns after 4 months with breathlessness at rest

28
Case 7 57 years old male smoker P/C- 3/52 cough PMH- LVSD Current medication-Bisoprolol 10mgs and Ramipril 7.5mgs o/e- chest clear, no signs of fluid overload CXR normal, renal function normal Review the previous diagnosis of heart failure Repeat BNP

29
Case 8 64 years olf female P/C- 2/7 breathlessness PMH- HT, STEMI 8/7 treated with PCI Medications- aspirin 75mgs, clopidogrel 75mgs, atenolol 25mgs, Ramipril 3.75mgs o/e- b/l crepts in lower 1/3 of lungs, raised JVP, 3 rd HS, normal Ues Suspected HF secondary to MI Treatment

30
Case 8 continued… Echo- moderately severe systolic dysfunction Aldosterone antagonist licensed for HF following MI Eplerenone 25mgs – monitor UE and K levels Change atenolol to Bisoprolol 1.25mgs Titrate Bisoprolol once signs of congestion cleared

Similar presentations
 Heart failure is the pathophysiological state in which an abnormality of cardiac function is responsible for failure of the heart to.>")













 failure is the state in which the heart is unable to pump blood.>")
, means your heart can't pump enough blood to meet your body's.>")



