Download presentation
Presentation is loading. Please wait.

1
Managing neglected stone disease Wahjoe Djatisoesanto Department of Urology, Faculty of Medicine Airlangga University- Soetomo General Hospital Surabaya

2
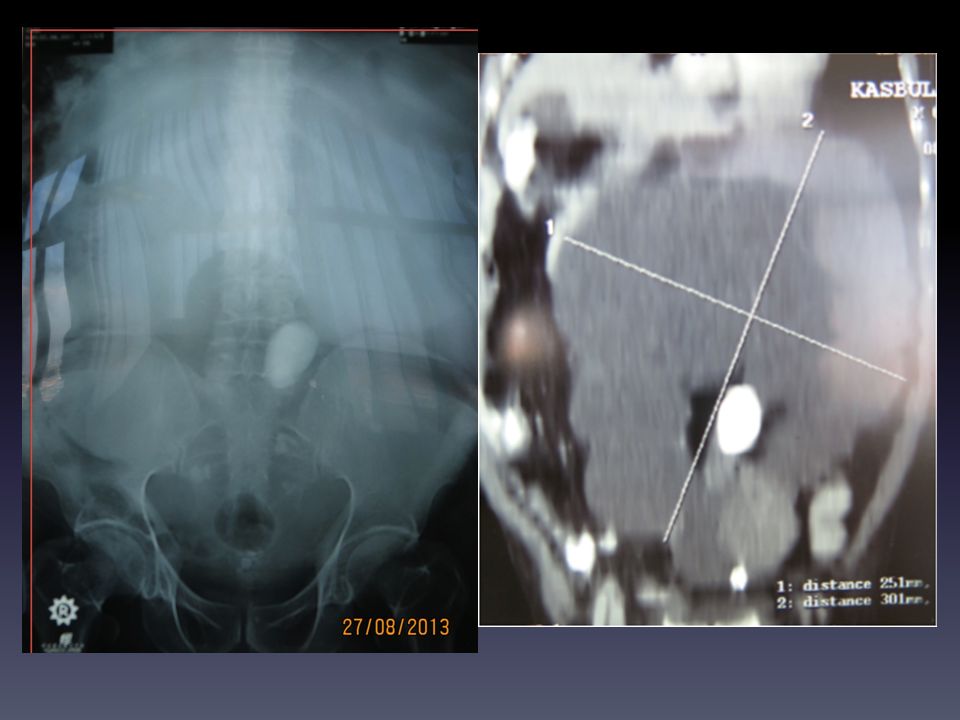
Introduction Urolithiasis has remained a mayor problem in Indonesia. The effective management of urolithiasis has witnessed a revolutionary change in recent years. There still remains the problem of neglected, asymptomatic large and/or staghorn stones associated with renal failure. These require a multifaceted approach where the mainstay of treatment remains open surgery.

3
Introduction The reason for neglected treatment: – The patient most often fear of and unwillingness to undergo surgery. – Practitioners of folklore medicine or rival system of medicine that they had some medicine to dissolve the stone. The majority of the patients in the third, fourth and fifth decades. Neglected renal calculi is a different entity in Indonesia: There is increasing incidence of stone disease The inadequate facilities for treatment

4
Formation and Incidence of kidney stones Nephrolithiasis is a condition in which hard masses(kidney stones) form within the urinary tract. Formation of kidney stones may occur when: – The urinary concentration of crystal-forming substances (e.g. calcium, oxalate, uric acid) is high. – The urinary concentration of substances that inhibit stone formation (e.g. citrate) is low. The lifetime incidence of kidney stones is approximately 13% for men and 7% for women. Among adults with kidney stones, approximately 80% consist predominately of calcium oxalate and/or calcium phosphate stones. Fink HA, Wilt TJ, Eidman KE, et al. AHRQ Comparative Effectiveness Review No. 61.
 is high. – The urinary concentration of substances that inhibit stone formation (e.g. citrate) is low. The lifetime incidence of kidney stones is approximately 13% for men and 7% for women. Among adults with kidney stones, approximately 80% consist predominately of calcium oxalate and/or calcium phosphate stones. Fink HA, Wilt TJ, Eidman KE, et al. AHRQ Comparative Effectiveness Review No")
5
Symptoms and signs Symptoms Flank pain Frequency and dysuria Nausea and vomiting Hematuria Intermittent fever Stone passage History of hypertension Oliguria or Anuria Signs Anemia Renal angle tenderness Hypertension Kidney mass Fluid overload Dehydration

6
Complications Anemia Hydronephrosis Chronic pyelonephritis Urinary infection Chronic renal failure Hypertension Pyonephrosis Non-functioning kidney Fluid overload Acute renal failure

7
Stone disease is not only the cause of pain and infection, carries a significant morbidity and mortality

8
Although various endourologic methods can be applied to make these patients stone-free, open surgery remains cost-effective. Literatur review shows that the problem of renal failure due to stone disease also exists in other developing countries, such as India and China but rarely in Western countries Gopalakrishnan G, Curr Opin Urol. 2007;17:132-5 Yang S, Qian H, Song C, J Endourol.2010;24:1721-4 Rule AD, Bergstralh EJ, Clin J Am Soc Nephrol.2009;4:804-11

9
Patients with large and/or staghorn stones and renal failure pose difficult problem a.Difficult to treat with ESWL or in combination with PCNL. b.For prevention of recurrence, complete removal is essential which is not possible with ESWL or PCNL. c.Kidney with impaired function cannot expel fragments after ESWL or PCNL. d.Associated infection can only be adequately controlled after complete removal of stones. e.Adhesions of kidney to perirenal fat and fascia and surrounding structures make PCNL difficult. In view of these factors open surgery is the main treatment for large and/or staghorn stones with the associated diseases..

10
During the periode of admission Daily complete blood test, blood urea and SC. Electrolytes were done and imbalance was corrected accordingly. Pre operative antibiotics should be given and changed according to culture and sensitivity of blood and urine. Hypertension and diabetes mellitus should be managed properly.

11
Comparison of co-morbids, congenital anomalies, and radiolucency in the study and the control groups. Hussain M,Hashmi AH et al; Endourology and stone disease; 10.2: 848-55

12
Comparison of side stones in the study and the control groups.

15
Management Management of each patient has had to be individualized. Patients admitted with renal failure (acute and/or chronic), have needed: – Initial workup to determine size and distribution of stone and biochemical status. – Correction of fluid balance – Hemodialysis as indicated before appropriate surgery could be performed.
, have needed: – Initial workup to determine size and distribution of stone and biochemical status. – Correction of fluid balance – Hemodialysis as indicated before appropriate surgery could be performed..")
16
Management Problems in the surgical management of neglected kidney stones: – Multiplicity of stones – Adhesions of the kidney to the perirenal fat and fascia making surgery difficult and hazardous. – Renal failure – Presence sometimes of only one functioning kidney. – Renal surgical hystory.

17
Management Principles of renal calculus surgery: – Strictly observed for removal of calculi. – Sterilize the urine with appropriate antibiotics – Appropriate dietetic and medical therapy (depend on stone chemical composition)
.")
18
Management Principles of renal calculus surgery: – Strictly observed for removal of calculi. – Sterilize the urine with appropriate antibiotics – Appropriate dietetic and medical therapy (depend on stone chemical composition)
.")
19
Definitive surgical procedures Initial management: PNS, ureteric catheterization followed by DJ stent and dialysis. Patients with fluid overload, hyperkalemia, acidosis, high blood urea and SC were initially dialized. Decision for PNS was made on the basis of biochemical tests and ultrasound findings.

20
Definitive surgical procedures Carried out when the patients became fit for surgery after initial resuscitation. The type of surgery varied according to site, size, number of stones, type of renal pelvis and general condition of the patient.

21
Management of stones with renal failure Stone analysis in the study group Hussain M,Hashmi AH et al; Endourology and stone disease; 10.2: 848-55

22
Interventions for preventing kidney stone recurrence Dietary interventions that are suggested to prevent stone recurrence by altering concentrations of crystal-forming or crystal- inhibiting substances in urine include: – Increasing water intake, reducing dietary oxalate, reducing dietary animal protein and other purines, and maintaining normal dietary calcium. Pharmacological interventions that are suggested to prevent stone recorrence include: – Thiazide diuretics, citrate, indapamide(a thiazide-likediuretic), allopurinol, magnesium hydroxide, and acetohydroxamic acid. Fink HA, Wilt TJ, Eidman KE, et al. AHRQ Comparative Effectiveness Review No. 61.
, allopurinol, magnesium hydroxide, and acetohydroxamic acid. Fink HA, Wilt TJ, Eidman KE, et al. AHRQ Comparative Effectiveness Review No")
25
Current guidelines on the role of open surgery Complex stone burden. Treatment failure of minimal invasive procedures. Intrarenal anatomical abnormalities or ectopic kidney. Morbid obesity. Skeletal deformity, contractures and fixed deformities of hips and legs. Comorbid medical disease. Concomitant open surgery. Non-functioning lower pole and/or kidney. Patient’s choice following failed minimally invasive procedures.

26
The role of open stone surgery in developing countries Countries in the Afro-Asian stone belt have a high incidence of urolithiasis. 30-50% of population live below the poverty line, and the gross national product is low. Poor nutritional status and inadequate health facilities. 40-50% of the urological workload in hospitals. A specific problem of this region is neglected asymptomatic large and/or staghorn calculi, and present with renal failure

27
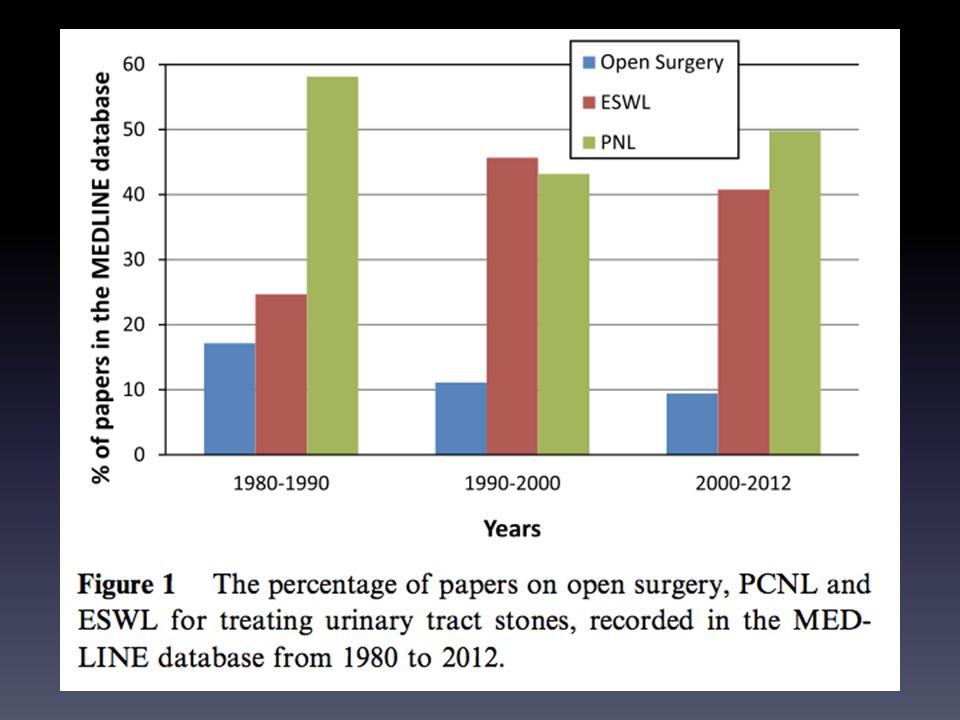
The role of open stone surgery in developing countries The incidence of open stone surgery: 1.5% in developed countries, but in developing countries has decreased from as high as 26% to 3.5%. The scope of open surgery will remain much wider in developing countries, because of – The pattern of stone disease. – Patient volume and overall economy.

28
Tamer El-Husseiny, Noor Buchholz. The role of open stone surgery. Arab Journal of Urology (2012) 10, 284-288. AUA recommendations in open surgery
 10, AUA recommendations in open surgery.")
29
Conclusion The results of neglect in the treatment of renal stones can be disastrous even. The type of treatment now being offered has improved greatly from that of several years ago. The morbidity and mortality is far higher than where renal stones are treated on time.

30
Conclusion The case of neglected renal calculi presenting very late for management, is challenge and on the other hand, a tragedy. This problem can be avoided by organizing public awareness programs in print and electronic media to educate the patients to seek early consultation. Education programs should be organized for family physicians for early diagnosis, treatment and referral to tertiary care urologic centers.

31
Thank you

Similar presentations


 Calcium phosphate stones (2) Magnesium ammonium phosphate stones (3)Calcium oxalate stones >")












 Triple phosphate237 (26.4%) Phosphate119 (13.4%) Uric.>")




