Download presentation
Presentation is loading. Please wait.

1
THE PREOPERATIVE CONSULT: AN INTRODUCTION Anthony Worsham, MD Best Practices Division of Hospital Medicine Department of Internal Medicine University of New Mexico Health Sciences Center

2
PRESENTATION OUTLINE What is the preoperative consult? Organ system specific review: Cardiac Pulmonary Endocrine (Diabetes) Hematologic (Anemia) GI (Liver disease) Good practices Questions
 Hematologic (Anemia) GI (Liver disease) Good practices Questions.")
3
CORE COMPETENCIES IN HOSPITAL MEDICINE: CLINICAL CONDITIONS Clinical conditions Acute Coronary Syndrome Acute Renal Failure Alcohol and Drug Withdrawal Asthma Cardiac Arrhythmia Cellulitis Chronic Obstructive Pulmonary Disease Community Acquired Pneumonia Congestive Heart Failure Clinical conditions (cont.) Delirium and Dementia Diabetes Mellitus Gastrointestinal Bleed Hospital-Acquired Pneumonia Pain Management Perioperative Medicine Sepsis Syndrome Stroke Urinary Tract Infection Venous Thromboembolism Dressler, et. al. The Core Competencies in Hospital Medicine: Development and Methodology. Journal of Hospital Medicine 2006;1:48-56.

4
PERIOPERATIVE MEDICINE KNOWLEDGE Hospitalists should be able to: Explain the effect of anesthesia and surgical intervention on physiology. Explain the goals and components of preoperative risk assessment. Identify patients who require selective preoperative testing based on patient specific factors, type of surgery, and urgency of surgical procedure. Describe risk factors for perioperative complications. Explain risks for perioperative complications in specific patient populations. Explain pharmacologic therapies that should be modified or held prior to surgery. List widely accepted risk assessment tools and explain their value and limitations in patients undergoing nonvascular surgery. Describe the evidence supporting prophylactic perioperative β -blockade. Dressler, et. al. The Core Competencies in Hospital Medicine: Development and Methodology. Journal of Hospital Medicine 2006;1:48-56.

5
PERIOPERATIVE MEDICINE SKILLS Hospitalists should be able to: Elicit a thorough history, review the medical record and inquire about functional capacity in patients undergoing surgery. Perform a targeted physical examination, focused on the cardiovascular and pulmonary systems and other systems based on patient history. Perform a directed and cost effective diagnostic evaluation based on patient relevant history and physical examination findings. Employ published algorithms and validated clinical scoring systems, when available, to assess and risk stratify patients. Assess the urgency of the requested evaluation and provide feedback and evaluation in an appropriate timeframe. Recognize medical conditions that increase risk for perioperative complications and make specific evidence based recommendations to optimize outcomes in the perioperative period. Determine the perioperative medical management strategies required to address specific disease states. Reassess patients for postoperative complications and make medical recommendations as indicated. Dressler, et. al. The Core Competencies in Hospital Medicine: Development and Methodology. Journal of Hospital Medicine 2006;1:48-56.

6
PERIOPERATIVE MEDICINE ATTITUDES Hospitalists should be able to: Communicate with patients and families to explain the hospitalist's role in their perioperative medical care, any indicated preoperative testing related to their medical conditions or risk assessment, and any adjustment of pharmacologic therapies. Communicate with patients and families to explain any indicated perioperative prophylactic measures. Communicate with patients and families to explain the need for follow-up medical care post-discharge. Initiate indicated perioperative preventive strategies. Recommend specific prophylactic measures, which may include β -blockade, VTE prophylaxis, or aspiration precautions, to avoid complications in the perioperative period. Serve as an advocate for patients. Promote a collaborative relationship with surgical services, which includes effective communication. Assess pain in perioperative patients and make recommendations for pain management when indicated. Facilitate discharge planning early in the hospitalization, including communicating with the primary care provider, and presenting the patient and family with contact information for follow-up care. Utilize evidence based recommendations for the evaluation and treatment of patients in the perioperative period. Dressler, et. al. The Core Competencies in Hospital Medicine: Development and Methodology. Journal of Hospital Medicine 2006;1:48-56.

7
PERIOPERATIVE MEDICINE SYSTEM ORGANIZATION AND IMPROVEMENT To improve efficiency and quality within their organizations, Hospitalists should: Lead, coordinate or participate in multidisciplinary efforts to develop clinical guidelines, protocols and pathways to improve the timing and quality of perioperative care from initial preoperative evaluation through all care transitions. Lead, coordinate or participate in efforts to improve the efficiency and quality of care through innovative models, which may include co-management of surgical patients in the perioperative period. Lead, coordinate or participate in multidisciplinary initiatives to promote patient safety and optimize diagnostic and management strategies for surgical patients requiring medical evaluation. Lead, coordinate or participate in multidisciplinary protocols to promote the rapid identification, triage, and expeditious evaluation of patients requiring urgent operations. Dressler, et. al. The Core Competencies in Hospital Medicine: Development and Methodology. Journal of Hospital Medicine 2006;1:48-56.

8
WHAT IS THE PREOPERATIVE CONSULT? A consult is an opportunity for the medical consultant to provide helpful management suggestions to the operative team. A fundamental objective of a consult is to optimize a patient’s underlying disease before it is compounded by the insult of surgery. The purpose of a consult is never to “clear” a patient for surgery. Whether or not to proceed to surgery is a question for the anesthesiologist, surgeon, and patient to decide after weighing the risks and benefits once the patient’s comorbidities are optimally managed. Lubarsky and Candiotti. Giving anesthesiologists what they want: how to write a useful preoperative consult. Cleve Clin J Med. 2009 Nov;76 Suppl 4:S32-6.

9
WHAT SHOULD THE PRE-OP EVAL FOCUS ON? Consultative and Perioperative Medicine Essentials for Hospitalists Perioperative Medication Management Pulmonary Risk Management in the Perioperative Setting Perioperative Cardiac Risk Assessment Preoperative Diagnostic Testing and Utilization of Basic Statistics Perioperative Management of Anticoagulation Anesthesia for Internists Evaluation and Management of Perioperative Cirrhosis and Liver Disease Neurosurgery for the Hospitalist The Obese Patient and Bariatric Surgery Evaluation and Management of Perioperative Anemia Perioperative Care of the Patient with Cancer Perioperative Cardiac Risk Management SHM consults. http://www.shmconsults.com

10
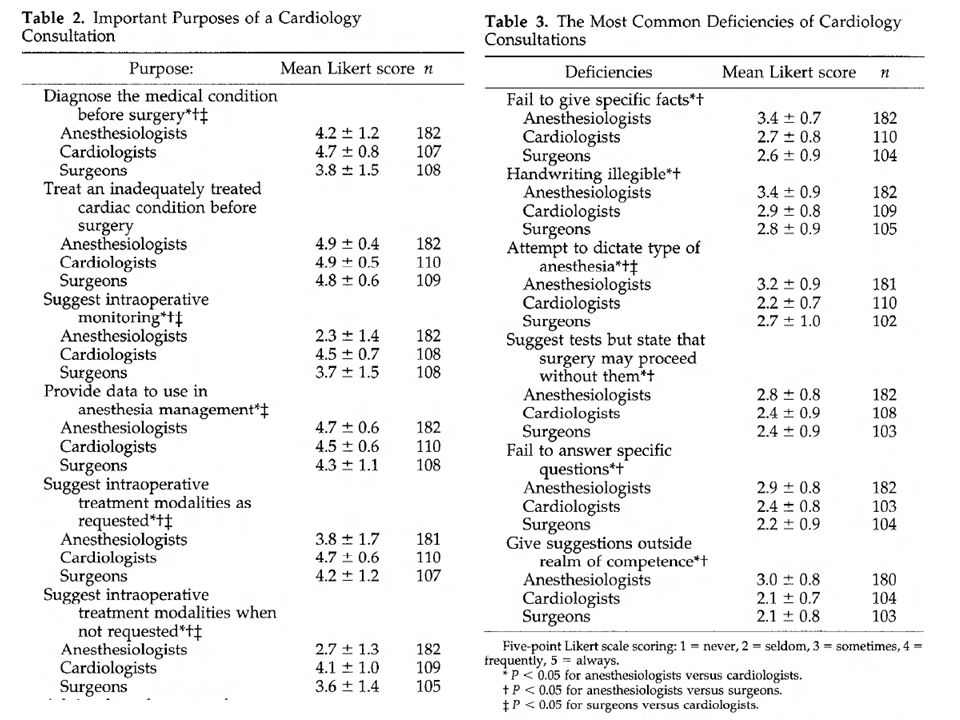
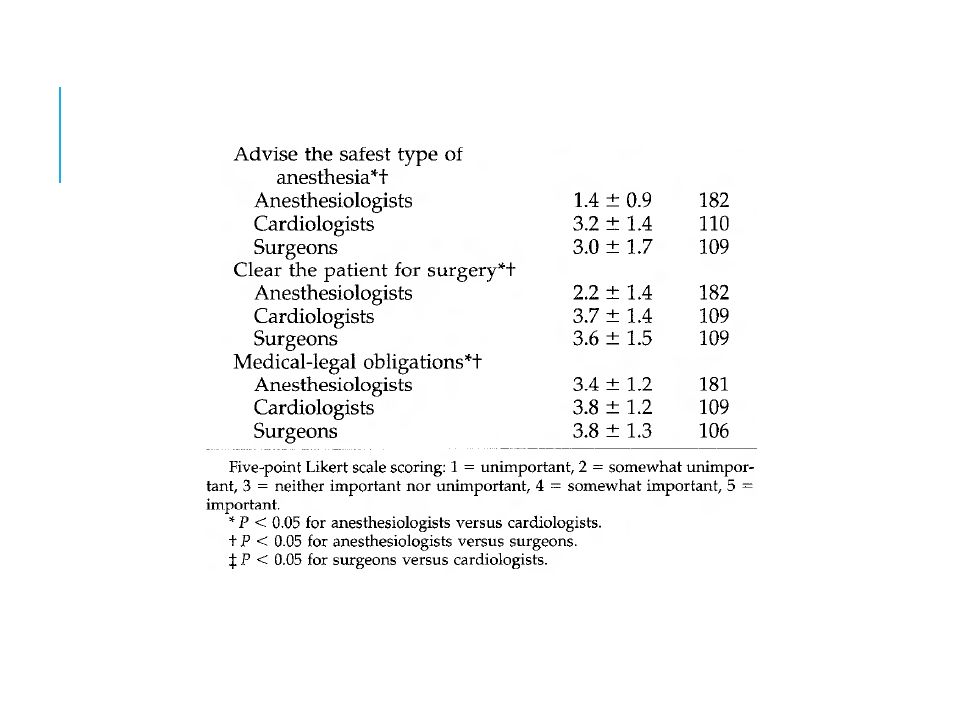
ARE PREOPERATIVE EVALUATIONS USEFUL? (1/3) survey about cardiology consultations sent to random New York anesthesiologists, surgeons, and cardiologists 400 surveys sent to each specialty 192 (48%/44%) were returned from anesthesiologists 113 (28%/26%) were returned from surgeons 129 (32%/30%) were returned from cardiologists. substantial disagreement on the importance and purposes of a cardiology consult: Intraoperative monitoring, “clearing the patient for surgery,” and advising as to the safest type of anesthesia were regarded as important by most cardiologists and surgeons but as unimportant by anesthesiologists (all P < 0.05) Most surgeons (80.2%) felt obligated to follow cardiology recommendations; few anesthesiologists (16.6%) felt so obligated (P < 0.05). Katz et al. A survey on the intended purposes and perceived utility of preoperative cardiology consultations. Anesth Analg. 1998 Oct;87(4):830-6.
 survey about cardiology consultations sent to random New York anesthesiologists, surgeons, and cardiologists 400 surveys sent to each specialty 192 (48%/44%) were returned from anesthesiologists 113 (28%/26%) were returned from surgeons 129 (32%/30%) were returned from cardiologists. substantial disagreement on the importance and purposes of a cardiology consult: Intraoperative monitoring, clearing the patient for surgery, and advising as to the safest type of anesthesia were regarded as important by most cardiologists and surgeons but as unimportant by anesthesiologists (all P < 0.05) Most surgeons (80.2%) felt obligated to follow cardiology recommendations; few anesthesiologists (16.6%) felt so obligated (P < 0.05). Katz et al. A survey on the intended purposes and perceived utility of preoperative cardiology consultations. Anesth Analg Oct;87(4):")
11
ARE PREOPERATIVE EVALUATIONS USEFUL? (2/3) charts of 55 consecutive patients aged >50 yr with preoperative cardiology consultations were examined substantial disagreement on the importance and purposes of a cardiology consult: Most commonly stated purpose of the 55 cardiology consultations examined was “preoperative evaluation.” Only 5 of these (9%) were obtained for patients in whom there was a new finding. 40% contained no recommendations other than “proceed with case,” “cleared for surgery,” or “continue current medications.” Recommendations regarding intraoperative monitoring or cardiac medications were largely ignored. Katz et al. A survey on the intended purposes and perceived utility of preoperative cardiology consultations. Anesth Analg. 1998 Oct;87(4):830-6.
 charts of 55 consecutive patients aged >50 yr with preoperative cardiology consultations were examined substantial disagreement on the importance and purposes of a cardiology consult: Most commonly stated purpose of the 55 cardiology consultations examined was preoperative evaluation. Only 5 of these (9%) were obtained for patients in whom there was a new finding. 40% contained no recommendations other than proceed with case, cleared for surgery, or continue current medications. Recommendations regarding intraoperative monitoring or cardiac medications were largely ignored. Katz et al. A survey on the intended purposes and perceived utility of preoperative cardiology consultations. Anesth Analg Oct;87(4):")
14
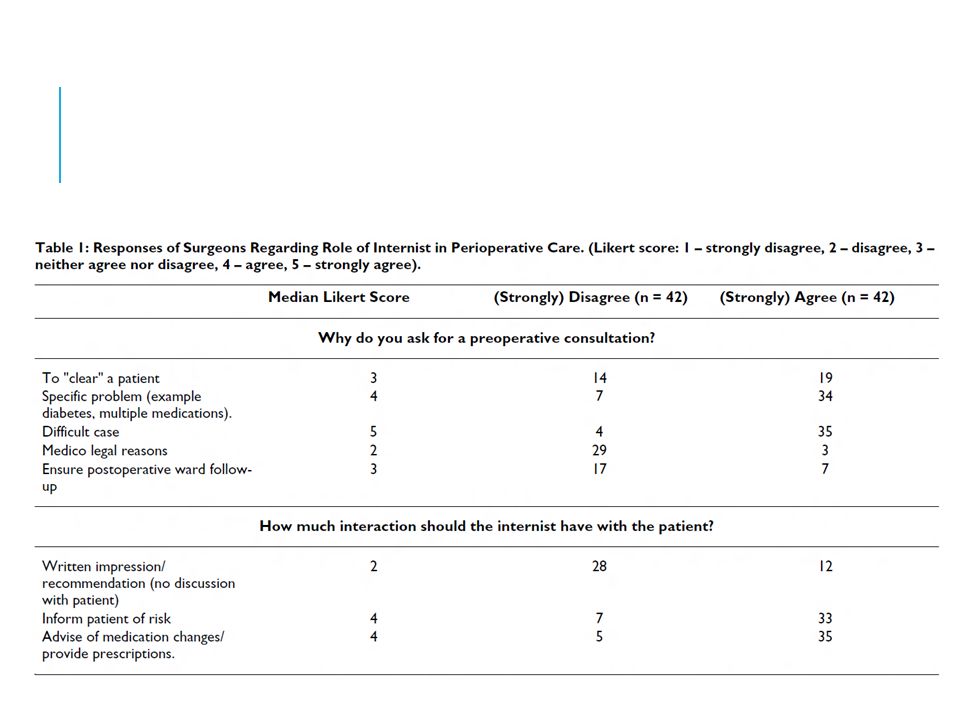
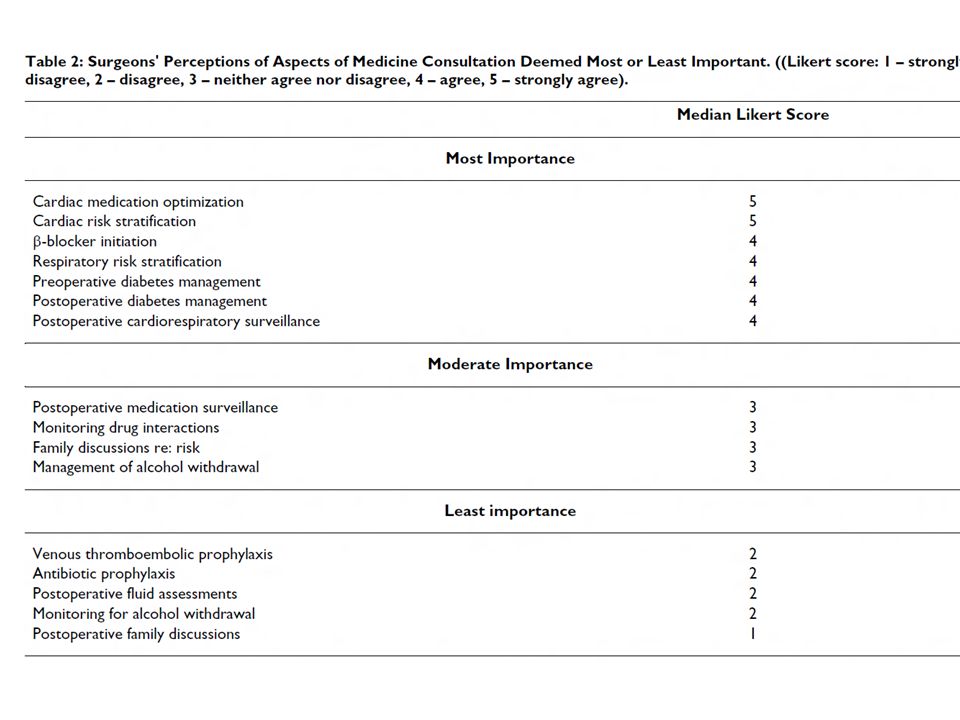
ARE PREOPERATIVE EVALUATIONS USEFUL? (3/3) Survey of surgeons in Saskatoon, Saskatchewan, Canada regarding an internist's potential role in perioperative care. Pausjenssen et al, An internist's role in perioperative medicine: a survey of surgeons' opinions. BMC Fam Pract. 2008 Jan 21;9:4.
 Survey of surgeons in Saskatoon, Saskatchewan, Canada regarding an internist s potential role in perioperative care. Pausjenssen et al, An internist s role in perioperative medicine: a survey of surgeons opinions. BMC Fam Pract Jan 21;9:4..")
17
PATHWAYS OF CARE Dhatariya et al. NHS Diabetes guideline for the perioperative management of the adult patient with diabetes. Diabet Med. 2012 Apr;29(4):420-33.
:")
18
ACC/AHA CARDIAC EVALUATION ALGORITHM Fleisher et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2007 Oct 23;116(17):e418-99.
:e")
19
ACTIVE CARDIAC CONDITIONS FOR WHICH THE PATIENT SHOULD UNDERGO EVALUATION AND TREATMENT BEFORE NONCARDIAC SURGERY (1/4) ACC/AHA Unstable coronary syndrome Decompensated HF Significant arrhythmia Severe valvular disease ESC Unstable angina pectoris Acute heart failure Significant cardiac arrhythmias Symptomatic valvular heart disease Recent MI and residual myocardial ischemia Fleisher et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2007 Oct 23;116(17):e418-99.
:e")
20
ACTIVE CARDIAC CONDITIONS FOR WHICH THE PATIENT SHOULD UNDERGO EVALUATION AND TREATMENT BEFORE NONCARDIAC SURGERY (2/4) Unstable coronary syndrome Unstable or severe angina* (CCS class III or IV)† Recent MI‡ Decompensated HF NYHA functional class IV Patients with cardiac disease resulting in inability to carry on any physical activity without discomfort. Symptoms of heart failure or the anginal syndrome may be present even at rest. If any physical activity is undertaken, discomfort increases. worsening or new-onset HF Fleisher et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2007 Oct 23;116(17):e418-99.
:e")
21
ACTIVE CARDIAC CONDITIONS FOR WHICH THE PATIENT SHOULD UNDERGO EVALUATION AND TREATMENT BEFORE NONCARDIAC SURGERY (3/4) Significant arrhythmia High-grade atrioventricular block Mobitz II atrioventricular block Third-degree atrioventricular heart block Symptomatic ventricular arrhythmias Supraventricular arrhythmias (including atrial fibrillation) with uncontrolled ventricular rate (HR greater than 100 bpm at rest) Symptomatic bradycardia Newly recognized ventricular tachycardia Fleisher et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2007 Oct 23;116(17):e418-99.
:e")
22
ACTIVE CARDIAC CONDITIONS FOR WHICH THE PATIENT SHOULD UNDERGO EVALUATION AND TREATMENT BEFORE NONCARDIAC SURGERY (4/4) Severe valvular disease Severe aortic stenosis (mean pressure gradient greater than 40 mm Hg, aortic valve area less than 1.0 cm 2, or symptomatic) Symptomatic mitral stenosis (progressive dyspnea on exertion, exertional presyncope, or HF) Fleisher et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2007 Oct 23;116(17):e418-99.
:e")
23
ACC/AHA CARDIAC EVALUATION ALGORITHM Fleisher et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2007 Oct 23;116(17):e418-99.
:e")
24
NEW YORK HEART ASSOCIATION (NYHA) FUNCTIONAL CLASSIFICATION IPatients with cardiac disease but resulting in no limitation of physical activity. Ordinary physical activity does not cause undue fatigue, palpitation, dyspnea or anginal pain. IIPatients with cardiac disease resulting in slight limitation of physical activity. They are comfortable at rest. Ordinary physical activity results in fatigue, palpitation, dyspnea or anginal pain. IIIPatients with cardiac disease resulting in marked limitation of physical activity. They are comfortable at rest. Less than ordinary activity causes fatigue, palpitation, dyspnea or anginal pain. IVPatients with cardiac disease resulting in inability to carry on any physical activity without discomfort. Symptoms of heart failure or the anginal syndrome may be present even at rest. If any physical activity is undertaken, discomfort increases.

25
CARDIAC RISK STRATIFICATION FOR NONCARDIAC SURGICAL PROCEDURES Poldermans et al. Guidelines for pre-operative cardiac risk assessment and perioperative cardiac management in non-cardiac surgery. Eur Heart J. 2009 Nov;30(22):2769-812.
:")
26
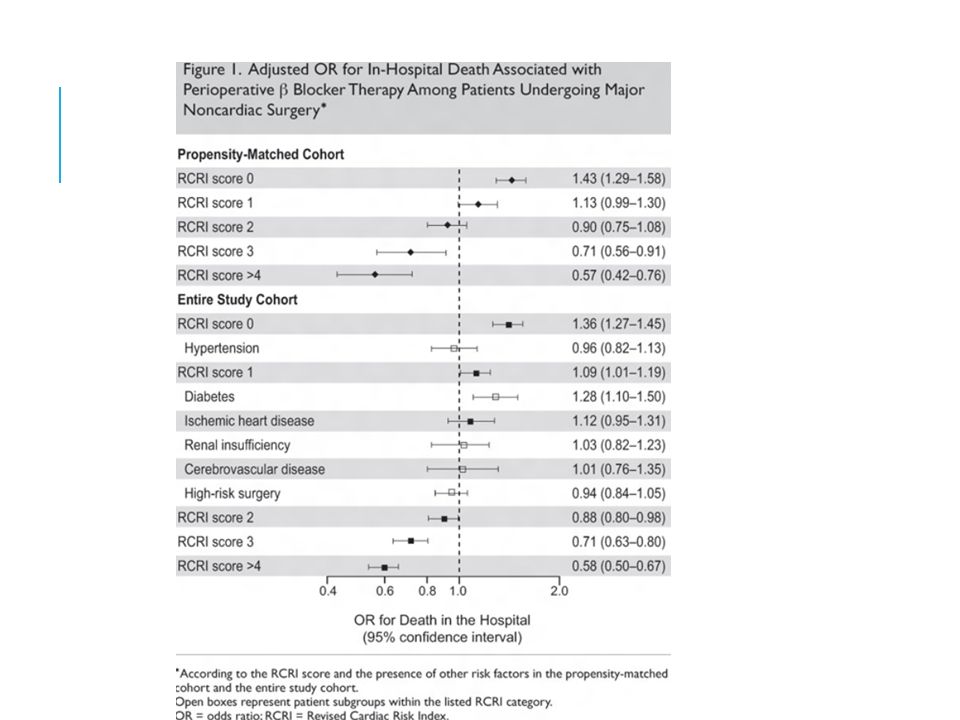
REVISED CARDIAC RISK INDEX (RCRI) Six independent predictors high-risk type of surgery history of ischemic heart disease history of congestive heart failure history of cerebrovascular disease preoperative treatment with insulin preoperative serum creatinine >2.0 mg/dL Rates of major cardiac complication 0: 0.5%-0.4% 1: 1.3%-0.9% 2: 4%-7% >=3: 9%-11% Lee et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation. 1999 Sep 7;100(10):1043-9.
:")
27
CARDIAC RISK CALCULATOR: YET ANOTHER RISK STRATIFICATION TOOL RCRI has relatively low discriminative ability 5 predictors of perioperative myocardial infarction or cardiac arrest: type of surgery, dependent functional status, abnormal creatinine, American Society of Anesthesiologists’ class, and increasing age Developed on 2007 ACS NSQIP database, validated with 2008 set Predictive performance improved over RCRI Gupta et al. Development and validation of a risk calculator for prediction of cardiac risk after surgery. Circulation. 2011 Jul 26;124(4):381-7.
:")
28
ACC/AHA CARDIAC EVALUATION ALGORITHM Fleisher et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2007 Oct 23;116(17):e418-99.
:e")
29
MET (METABOLIC EQUIVALENT) ratio of the work metabolic rate to the resting metabolic rate. One MET is defined as 1 kcal/kg/hour and is roughly equivalent to the energy cost of sitting quietly. A MET also is defined as oxygen uptake in ml/kg/min with one MET equal to the oxygen cost of sitting quietly, equivalent to 3.5 ml/kg/min. METS for common activities 1.0: lying quietly and watching television 2.3: getting ready for bed, general, standing 3.5: walking for pleasure 3.8: cleaning, sweeping, slow, moderate effort 4.0: stair climbing, slow pace 4.0: bicycling, <10 mph, leisure, to work or for pleasure 4.0: raking lawn Ainsworth et al. 2011 Compendium of Physical Activities: a second update of codes and MET values. Med Sci Sports Exerc. 2011 Aug;43(8):1575-81.
:")
30
METS AND FUNCTIONAL CAPACITY Poldermans et al. Guidelines for pre-operative cardiac risk assessment and perioperative cardiac management in non-cardiac surgery. Eur Heart J. 2009 Nov;30(22):2769-812.
:")
31
ACC/AHA CARDIAC EVALUATION ALGORITHM Fleisher et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2007 Oct 23;116(17):e418-99.
:e")
32
ACC/AHA ALGORITHM (2/2)
")
33
ESC ALGORITHM (1/3) Poldermans et al. Guidelines for pre-operative cardiac risk assessment and perioperative cardiac management in non-cardiac surgery. Eur Heart J. 2009 Nov;30(22):2769-812.
:")
34
ESC ALGORITHM (2/3) Poldermans et al. Guidelines for pre-operative cardiac risk assessment and perioperative cardiac management in non-cardiac surgery. Eur Heart J. 2009 Nov;30(22):2769-812.
:")
35
ESC ALGORITHM (3/3) Poldermans et al. Guidelines for pre-operative cardiac risk assessment and perioperative cardiac management in non-cardiac surgery. Eur Heart J. 2009 Nov;30(22):2769-812.
:")
37
BETA-BLOCKER TRIALS Poldermans et al. Guidelines for pre-operative cardiac risk assessment and perioperative cardiac management in non-cardiac surgery. Eur Heart J. 2009 Nov;30(22):2769-812.
:")
38
BETA-BLOCKER TRIALS Poldermans et al. Guidelines for pre-operative cardiac risk assessment and perioperative cardiac management in non-cardiac surgery. Eur Heart J. 2009 Nov;30(22):2769-812.
:")
39
BETA-BLOCKER RECOMMENDATIONS Siddiqui and Feldman. Perioperative Cardiac Risk Assessment. SHM Consults.

40
MEDICATION RECOMMENDATIONS Statins Continue statins for any patient already on them chronically. Start a statin at least 2 weeks ahead of time for any patient who: should be treated with one based on the NCEP guidelines, those undergoing vascular surgery, and those with 1 or more clinical risk factors who are undergoing intermediate surgery. Aspirin Continue aspirin unless difficult hemostasis expected.

41
PREOPERATIVE INTERVENTIONS PCI [percutaneous coronary intervention] before noncardiac surgery is of no value in preventing perioperative cardiac events, except in those patients in whom PCI is independently indicated for an acute coronary syndrome. A history of coronary bypass surgery reduces the cardiac event rate to 0.6% for noncardiac surgeries in the subsequent 6 years
![PREOPERATIVE INTERVENTIONS PCI [percutaneous coronary intervention] before noncardiac surgery is of no value in preventing perioperative cardiac events, except in those patients in whom PCI is independently indicated for an acute coronary syndrome.](http://images.slideplayer.com/35/10456760/slides/slide_41.jpg "A history of coronary bypass surgery reduces the cardiac event rate to 0.6% for noncardiac surgeries in the subsequent 6 years.")
42
RECOMMENDATIONS FOR TIMING OF NON-CARDIAC SURGERY AFTER PCI

43
ECGS FOR POSTOPERATIVE MONITORING In patients with high or intermediate clinical risk who have known or suspected CAD and who are undergoing high- or intermediate-risk surgical procedures, the procurement of ECGs at baseline, immediately after the surgical procedure and daily on the first 2 days after surgery appears to be the most cost-effective strategy. Studies analyzing signs and symptoms of perioperative MI have shown that chest pain can occur in as little as 10% to 20% of the patients who rule in by enzymes, ECG, or scintigraphy

44
POSTOPERATIVE PULMONARY COMPLICATIONS (PPCS) General complications Atelectasis Infection Bronchitis Pneumonia Bronchospasm Pulmonary embolism Exacerbation of underlying chronic lung disease Respiratory failure and prolonged invasive or noninvasive ventilation OSA ARDS Specific cardiothoracic surgical complications Phrenic nerve injury Pleural effusion Bronchopleural fistula Sternal wound infection and empyema Gastroesophageal anastomotic leak Postoperative arrhythmias Bapoje et al. Preoperative evaluation of the patient with pulmonary disease. Chest. 2007 Nov;132(5):1637-45.
:")
45
RISK FACTORS FOR PPCS Preoperative risk factors COPD Age Inhaled tobacco use NYHA class II pulmonary hypertension OSA Nutrition status Intraoperative risk factors Site of surgery General anesthesia Pancuronium use Duration of surgery Emergency surgery Bapoje et al. Preoperative evaluation of the patient with pulmonary disease. Chest. 2007 Nov;132(5):1637-45.
:")
47
STEPWISE APPROACH TO PREOPERATIVE PULMONARY ASSESSMENT (1/2) Bapoje et al. Preoperative evaluation of the patient with pulmonary disease. Chest. 2007 Nov;132(5):1637-45.
:")
48
STEPWISE APPROACH TO PREOPERATIVE PULMONARY ASSESSMENT (2/2) Bapoje et al. Preoperative evaluation of the patient with pulmonary disease. Chest. 2007 Nov;132(5):1637-45.
:")
49
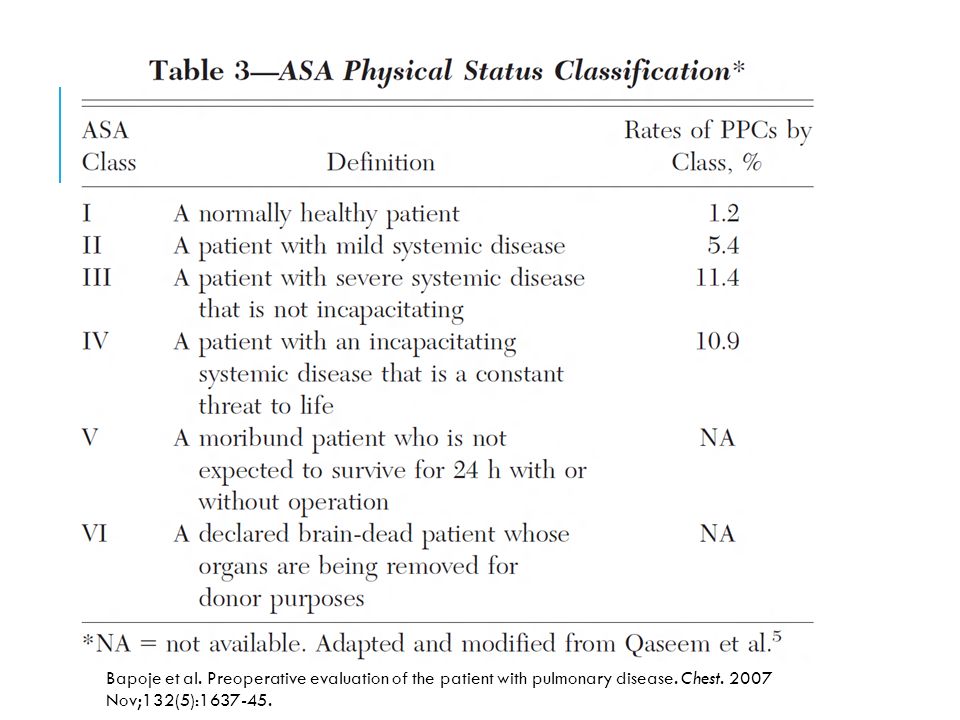
ACP GUIDELINES Recommendation 1: All patients undergoing noncardiothoracic surgery should be evaluated for the presence of the following significant risk factors for postoperative pulmonary complications in order to receive pre- and postoperative interventions to reduce pulmonary risk: chronic obstructive pulmonary disease, age older than 60 years, American Society of Anesthesiologists (ASA) class of II or greater, functionally dependent, and congestive heart failure. The following are not significant risk factors for postoperative pulmonary complications: obesity and moderate asthma. Qaseem et al. Risk assessment for and strategies to reduce perioperative pulmonary complications for patients undergoing noncardiothoracic surgery: a guideline from the American College of Physicians. Ann Intern Med. 2006 Apr 18;144(8):575-80.
:")
50
ACP GUIDELINES Recommendation 2: Patients undergoing the following procedures are at higher risk for postoperative pulmonary complications and should be evaluated for other concomitant risk factors and receive pre- and postoperative interventions to reduce pulmonary complications: prolonged surgery (3 hours), abdominal surgery, thoracic surgery, neurosurgery, head and neck surgery, vascular surgery, aortic aneurysm repair, emergency surgery, and general anesthesia. Qaseem et al. Risk assessment for and strategies to reduce perioperative pulmonary complications for patients undergoing noncardiothoracic surgery: a guideline from the American College of Physicians. Ann Intern Med. 2006 Apr 18;144(8):575-80.
:")
51
ACP GUIDELINES Recommendation 3: A low serum albumin level (35 g/L) is a powerful marker of increased risk for postoperative pulmonary complications and should be measured in all patients who are clinically suspected of having hypoalbuminemia; measurement should be considered in patients with 1 or more risk factors for perioperative pulmonary complications. Recommendation 4: All patients who after preoperative evaluation are found to be at higher risk for postoperative pulmonary complications should receive the following postoperative procedures in order to reduce postoperative pulmonary complications: 1) deep breathing exercises or incentive spirometry and 2) selective use of a nasogastric tube (as needed for postoperative nausea or vomiting, inability to tolerate oral intake, or symptomatic abdominal distention). Qaseem et al. Risk assessment for and strategies to reduce perioperative pulmonary complications for patients undergoing noncardiothoracic surgery: a guideline from the American College of Physicians. Ann Intern Med. 2006 Apr 18;144(8):575-80.
 deep breathing exercises or incentive spirometry and 2) selective use of a nasogastric tube (as needed for postoperative nausea or vomiting, inability to tolerate oral intake, or symptomatic abdominal distention). Qaseem et al. Risk assessment for and strategies to reduce perioperative pulmonary complications for patients undergoing noncardiothoracic surgery: a guideline from the American College of Physicians. Ann Intern Med Apr 18;144(8):")
52
ACP GUIDELINES Recommendation 5: Preoperative spirometry and chest radiography should not be used routinely for predicting risk for postoperative pulmonary complications. Preoperative pulmonary function testing or chest radiography may be appropriate in patients with a previous diagnosis of chronic obstructive pulmonary disease or asthma. Recommendation 6: The following procedures should not be used solely for reducing postoperative pulmonary complication risk: 1) right-heart catheterization and 2) total parenteral nutrition Qaseem et al. Risk assessment for and strategies to reduce perioperative pulmonary complications for patients undergoing noncardiothoracic surgery: a guideline from the American College of Physicians. Ann Intern Med. 2006 Apr 18;144(8):575-80.
 right-heart catheterization and 2) total parenteral nutrition Qaseem et al. Risk assessment for and strategies to reduce perioperative pulmonary complications for patients undergoing noncardiothoracic surgery: a guideline from the American College of Physicians. Ann Intern Med Apr 18;144(8):")
53
PATIENT FACTORS WITH PPCS Smetana et al. Preoperative pulmonary risk stratification for noncardiothoracic surgery: systematic review for the American College of Physicians. Ann Intern Med. 2006 Apr 18;144(8):581-95.
:")
54
PROCEDURE FACTORS WITH PPCS Smetana et al. Preoperative pulmonary risk stratification for noncardiothoracic surgery: systematic review for the American College of Physicians. Ann Intern Med. 2006 Apr 18;144(8):581-95.
:")
55
SUGGESTED RISK-REDUCTION STRATEGIES Preoperative Smoking cessation 6–8 wk before undergoing surgery Inspiratory muscle training Intraoperative Use of neuromuscular agents other than pancuronium Postoperative IS But note recent Cochrane reviews found no evidence regarding the effectiveness of the use of incentive spirometry for prevention of postoperative pulmonary complications in upper abdominal surgery (Guimarães et al 2009) and following CABG (Freitas et al 2007, Freitas et al 2012). CPAP Bapoje et al. Preoperative evaluation of the patient with pulmonary disease. Chest. 2007 Nov;132(5):1637-45.
:")
56
INTERVENTIONS TO REDUCE RISK OF POSTOPERATIVE PULMONARY COMPLICATIONS Lawrence et al. Strategies to reduce postoperative pulmonary complications after noncardiothoracic surgery: systematic review for the American College of Physicians. Ann Intern Med. 2006 Apr 18;144(8):596-608.
:")
57
POSTOPERATIVE COMPLICATIONS ASSOCIATED WITH PREOPERATIVE ANEMIA mortality delirium perioperative infections massive transfusion related risks hypothermia pulmonary microembolization increased length of stay Kumar, A. Evaluation and Management of Perioperative Anemia. SHM Consults.

58
RISK FACTORS FOR PREOPERATIVE ANEMIA Symptoms of anemia chest pain dyspnea fatigue Physical examination findings tachycardia Skin pallor Comorbid illnesses hematologic diseases chronic kidney disease liver disease alcohol abuse Kumar, A. Evaluation and Management of Perioperative Anemia. SHM Consults.

59
EXPECTED BLOOD LOSS FOR SEVERAL COMMON SURGERIES Total hip arthoplasty: 2100 mL Total knee arthroplasty: 2000 mL Spine fusion: 1000 mL Hip fracture repair: 750 mL Open prostatectomy: 750 mL Transurethral resection of prostate: 500 mL Coronary bypass grafting: 500 mL Kumar, A. Evaluation and Management of Perioperative Anemia. SHM Consults.

60
EVALUATE ANEMIA WHEN: Hemoglobin <10 g/dL Hemoglobin ≥10 g/dL but expected blood loss from surgery expected to lower hemoglobin to <8 g/dL Occult gastrointestinal blood loss suspected as cause and postoperative care will include pharmacologic VTE prophylaxis Major hematologic disorder or malignancy are suspected as cause of anemia Kumar, A. Evaluation and Management of Perioperative Anemia. SHM Consults.

61
DIFFICULTIES WITH IN-HOSPITAL PRE-OP EVALS Hgb recovers within 1 mo of starting nutritional (B12 or folate) supplementation ESAs + iron takes 1-2 weeks to be effective; goal Hgb 11-12 g/dL (NKF). Kumar, A. Evaluation and Management of Perioperative Anemia. SHM Consults.

62
RECOMMENDED CRITERIA FOR PERIOPERATIVE TRANSFUSION hemoglobin < 7 g/dL hemoglobin <10 g/dL and.. Signs or symptoms strongly suggestive of significant anemia with a chest pain dyspnea hypotension tachycardia Anticipated large blood loss Kumar, A. Evaluation and Management of Perioperative Anemia. SHM Consults.

63
RELEVANT STUDIES TRICC (1999) FOCUS American Association of Blood Banks guidelines (2012)
 FOCUS American Association of Blood Banks guidelines (2012)")
64
Red blood cell salvage collect blood from operative fields or wound sites and reinfuse the blood back into the patient. It involves collection and saline washing of blood products, removal of platelets and plasma proteins, and reinfusion. In summary, for patients at high risk for intraoperative blood loss and with no significant potential for surgical field contamination with bacteria, cancer cells or other fluids, RBC salvage is an effective technique for reducing allogeneic blood transfusion.

65
Perioperative anemia is a commonly encountered clinical problem associated with increased morbidity and mortality. Whenever possible, full evaluation of anemia should be performed prior to surgery and reversible causes corrected. Perioperative allogeneic blood transfusion may be necessary but should be minimized as much as possible due to its potential for increasing mortality, postoperative infections, and several other adverse effects. Reserving RBC transfusion for patients with a symptomatic anemia, a rapidly falling hemoglobin, or a hemoglobin of less than 7 to 8 g/dL is a reasonable approach to blood conservation. Several other modalities for blood conservation are available and may be useful for select patients. Postoperative anemia is usually due to expected surgical blood loss. Other causes should be considered, especially when the level of anemia exceeds expectations or it occurs after the first 1 to 2 days after surgery.

66
DIABETES MANAGEMENT Surgery and anesthesia can induce hormonal and inflammatory stressors that increase the risk of complications in patients with diabetes. Elevated blood glucose levels are associated with worse outcomes in surgical patients, even among those not diagnosed with diabetes. The perioperative glycemic target in critically ill patients is 140 to 180 mg/dL. Evidence for a target in patients who are not critically ill is less robust, though fasting levels less than 140 mg/dL and random levels less than 180 mg/dL are appropriate. Postoperative nutrition-related insulin needs vary by nutrition type (parenteral or enteral), but ideally all regimens should incorporate a basal/bolus approach to insulin replacement. Meneghini LF. Perioperative management of diabetes: translating evidence into practice. Cleve Clin J Med. 2009 Nov;76 Suppl 4:S53-9.
, but ideally all regimens should incorporate a basal/bolus approach to insulin replacement. Meneghini LF. Perioperative management of diabetes: translating evidence into practice. Cleve Clin J Med Nov;76 Suppl 4:S")
67
GOALS OF DIABETIC MANAGEMENT Maintenance of fluid and electrolyte balance Prevention of ketoacidosis Avoidance of marked hyperglycemia Avoidance of hypoglycemia Khan et al. Perioperative management of diabetes mellitus. UpToDate 2012.

68
INITIAL EVALUATION History and physical to include: Determination of the type of diabetes, since type 1 diabetes patients are at much higher risk of diabetic ketoacidosis Long-term complications of diabetes mellitus, including retinopathy, nephropathy, neuropathy, autonomic neuropathy, coronary heart disease, peripheral vascular disease, hypertension Assessment of baseline glycemic control, including frequency of monitoring, average blood glucose levels, range of blood glucose levels, hemoglobin A1C levels Assessment of hypoglycemia, including frequency, timing, awareness, and severity Detailed history of diabetes therapy, including insulin type, dose, and timing Other pharmacologic therapy, including type of medication, dosing, and specific timing Characteristics of surgery, including when the patient must stop eating prior to surgery, type of surgery (major or minor), timing of the operative procedure, and duration of the procedure Type of anesthetic, including epidural versus general anesthesia (epidural anesthesia has minimal effects on glucose metabolism and insulin resistance)
, timing of the operative procedure, and duration of the procedure Type of anesthetic, including epidural versus general anesthesia (epidural anesthesia has minimal effects on glucose metabolism and insulin resistance)")
69
DIABETES MEDICATION MANAGEMENT (1/2) Discontinue oral agents. Omit any short-acting insulin on the morning of surgery. For patients who take insulin only in the morning, give between one- half to two-thirds of their usual total morning insulin dose (both intermediate and short-acting insulin) as intermediate or long-acting insulin to provide basal insulin during the procedure and prevent ketosis. For patients who take insulin two or more times per day, give between one-third to one-half of the total morning dose (both intermediate and short-acting insulin) as intermediate acting insulin only. Khan et al. Perioperative management of diabetes mellitus. UpToDate 2012.
 as intermediate or long-acting insulin to provide basal insulin during the procedure and prevent ketosis. For patients who take insulin two or more times per day, give between one-third to one-half of the total morning dose (both intermediate and short-acting insulin) as intermediate acting insulin only. Khan et al. Perioperative management of diabetes mellitus. UpToDate")
70
DIABETES MEDICATION MANAGEMENT Patients on continuous insulin infusion may continue with their usual basal infusion rate. Start dextrose containing intravenous solution (either dextrose with water or one-half isotonic saline) at a rate of 75 to 125 cc/hour to provide 3.75 to 6.25 g glucose/hour to avoid the metabolic changes of starvation. Khan et al. Perioperative management of diabetes mellitus. UpToDate 2012.
 at a rate of 75 to 125 cc/hour to provide 3.75 to 6.25 g glucose/hour to avoid the metabolic changes of starvation. Khan et al. Perioperative management of diabetes mellitus. UpToDate")
71
MANAGEMENT OF LIVER DISEASE Goals Evaluate whether liver disease severity influences perioperative morbidity and mortality. Outline the risk associated with different types of surgery in patients with cirrhosis. Identify the elements of the preoperative evaluation for a patient with cirrhosis including how to manage medications on the day of surgery. Formulate a perioperative care plan for the patient with cirrhosis based on the underlying severity of disease including how to manage medications. Qamar, A. Evaluation and Management of Perioperative Cirrhosis and Liver Disease. SHM Consults.

72
MANAGEMENT OF LIVER DISEASE Acute hepatitis, especially alcoholic hepatitis, and decompensated cirrhosis are contraindications to elective surgery. Qamar, A. Evaluation and Management of Perioperative Cirrhosis and Liver Disease. SHM Consults.

73
RISK ASSESSMENT IN CIRRHOSIS CHILD-PUGH SCORE Qamar, A. Evaluation and Management of Perioperative Cirrhosis and Liver Disease. SHM Consults.

74
RISK ASSESSMENT IN CIRRHOSIS MELD SCORE Qamar, A. Evaluation and Management of Perioperative Cirrhosis and Liver Disease. SHM Consults.

75
OPERATIVE FACTORS ASSOCIATED WITH INCREASED RISK WITH SURGERY IN PATIENTS WITH CIRRHOSIS type of surgery emergency surgery upper abdominal and cardiovascular surgery (75% perioperative mortality rate in Child-Pugh class C) intraoperative hypotension perioperative hemorrhage use of vasopressor support use of prolonged cardiac bypass type of anesthetic
 intraoperative hypotension perioperative hemorrhage use of vasopressor support use of prolonged cardiac bypass type of anesthetic")
76
SUGGESTED PREOPERATIVE ALGORITHM FOR PATIENTS WITH CIRRHOSIS Etiology of liver disease Presence or absence of cirrhosis Evidence of synthetic dysfunction or portal hypertension Use of medications Calculate MELD and Child-Pugh score Imaging for new symptoms or no recent studies Qamar, A. Evaluation and Management of Perioperative Cirrhosis and Liver Disease. SHM Consults.

77
DRUG MANAGEMENT Hepatitis B: continue nucleoside and nucleotide analogues. Hepatitis C: complete therapy prior to elective surgery; hold therapy until complete recovery from emergent surgery. Alcoholic hepatitis: complete therapy first due to high baseline postoperative risk Autoimmune hepatitis: continue steroids or azathioprine + possible stress- dose steriods PBC/PSC: continue ursodeoxycholic acid Wilson’s disease: half penicillamine dose due to impaired wound healing Cirrhosis: hold b-blocker on day of surgery; continue lactulose/rifaximin; ?hold diuretics to optimize fluid status; ?albumin prophylaxis esp. with ascites loss during surgery; ?transfuse to Hgb 25% to prevent overtransfusion in pts with varices, PLT 50-100K, INR >1.5; Qamar, A. Evaluation and Management of Perioperative Cirrhosis and Liver Disease. SHM Consults.

78
LIVER DISEASE MANAGEMENT Qamar, A. Evaluation and Management of Perioperative Cirrhosis and Liver Disease. SHM Consults.

79
ASA PHYSICAL STATUS CLASSIFICATION FOR SURGICAL CANDIDATES I: Normal healthy patient II: Patient with mild systemic disease III: Patient with severe systemic disease IV: Patient with severe systemic disease that is a constant threat to life V: Moribund patient who is not expected to survive without the operation

80
USEFUL INFORMATION TO INCLUDE IN PREOPERATIVE CONSULTS (1/3) How to preoperatively optimize function of an unhealthy organ system Guidance on managing oral drug regimens First-line and second-line agents Initial dosage and titration; recommended combinations How to manage side effects Expected time until patient is optimized for the procedure if above management is followed Tests that might be indicated preoperatively to direct therapy to optimize function Lubarsky and Candiotti. Giving anesthesiologists what they want: how to write a useful preoperative consult. Cleve Clin J Med. 2009 Nov;76 Suppl 4:S32-6.

81
USEFUL INFORMATION TO INCLUDE IN PREOPERATIVE CONSULTS (2/3) Additional interventions indicated by the patient’s disease, and appropriate timing (pre-, intra-, postoperatively) Include assurance that consultant will follow up with specified nonurgent postoperative care without prompting Current pertinent anticoagulation recommendations Details on coronary stents—when placed, where placed, and type (drug-eluting or bare metal) Focused information on cardiac defibrillators and other implanted devices, specifically: Whether patient is pacer-dependent Effect of magnet placement Has battery recently been checked? Lubarsky and Candiotti. Giving anesthesiologists what they want: how to write a useful preoperative consult. Cleve Clin J Med. 2009 Nov;76 Suppl 4:S32-6.

82
USEFUL INFORMATION TO INCLUDE IN PREOPERATIVE CONSULTS (3/3) Recommendations on intra-/perioperative management of: Rare diseases Blood disorders, especially coagulation abnormalities Brittle diabetes (loading doses, optimal make-up of infusions, treatment targets) Endocrine disorders (eg, perioperative dosing of thyroid drugs) Newer recommendations/data (< 5 years old) on acute medical management, especially in patients with complex comorbidities Explanations/references when recommendations deviate from accepted guidelines Legible contact information, including an emergency phone number to ensure access prior to early-morning procedures In all cases, be as specific as possible and favor quantitative over qualitative information when possible.
 Recommendations on intra-/perioperative management of: Rare diseases Blood disorders, especially coagulation abnormalities Brittle diabetes (loading doses, optimal make-up of infusions, treatment targets) Endocrine disorders (eg, perioperative dosing of thyroid drugs) Newer recommendations/data (< 5 years old) on acute medical management, especially in patients with complex comorbidities Explanations/references when recommendations deviate from accepted guidelines Legible contact information, including an emergency phone number to ensure access prior to early-morning procedures In all cases, be as specific as possible and favor quantitative over qualitative information when possible.")
83
A FINAL END USER: THE PLAINTIFF’S ATTORNEY A poorly written consult may benefit plaintiffs’ lawyers. Consults should never give absolute instructions; it is better to use such phrases as “Strongly consider…” or “The current literature strongly suggests…” Otherwise, the surgical team is placed in an awkward position if it does not follow your recommendations, even if for good reason. If a certain recommendation absolutely must be followed, then direct oral communication from the consultant to the attending anesthesiologist (or surgeon) is best. Lubarsky and Candiotti. Giving anesthesiologists what they want: how to write a useful preoperative consult. Cleve Clin J Med. 2009 Nov;76 Suppl 4:S32-6.
 is best. Lubarsky and Candiotti. Giving anesthesiologists what they want: how to write a useful preoperative consult. Cleve Clin J Med Nov;76 Suppl 4:S")
84
QUESTIONS FOR THE GROUP Should we continue to follow patients after an initial preoperative consult? When do you defer a consult to a more specific specialty? Would a separate consult service be helpful? Are the consult questions specific enough to form a useful consult? Do surgery and anesthesia find our consults to be useful? Are our recommendations acted upon? Would co-management be useful? What is your threshold for delaying surgery? Do you perform a preoperative evaluation on your own patients?

85
POSSIBLE ACTION ITEMS Survey surgeons, anesthesiologists, hospitalists, and residents regarding expectations and attitudes about preoperative evaluation Develop preoperative consult worksheet and/or template Fund enough FTE and secure sufficient residents for a dedicated consult service Develop a hospital medicine consult curriculum Mandate completion of the SHM consult series

Similar presentations
 trial.>")


















