Download presentation
Presentation is loading. Please wait.

1
Anterior abdominal wall (IRS)
Objectives Describe the anterior abdominal wall: musculature and fascial layers formation of rectus sheath and its contents relevance to surgical incisions; Describe the dermatomes and concept of referred pain Describe the deep and superficial inguinal rings Describe the boundaries of inguinal canal

2
Anterior abdominal wall
DR. WAI WAI KYI Feb 2012

3
The abdominal wall Boundaries of the abdomen Superior - diaphragm Inferior - pelvic inlet Anterior - anterior abdominal wall Posterior - lumbar vertebrae, upper part of bony pelvis, psoas and quadratus lumborum muscles.

4
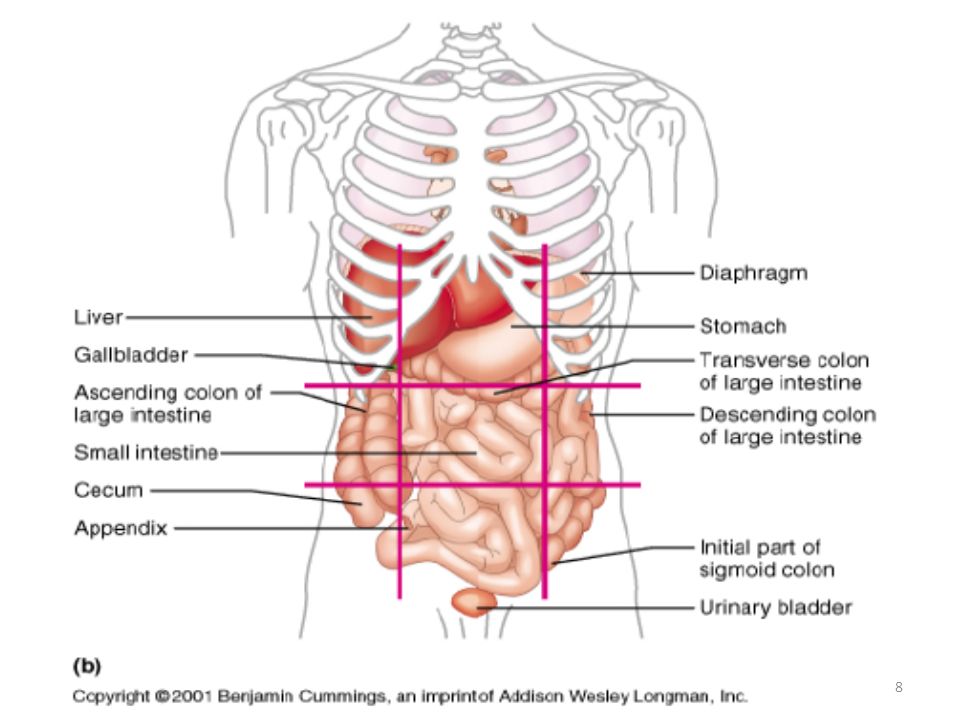
Organs by Abdominal Quadrant
Right Left Upper Small and Large Intestine Lower part of Kidney Half of Bladder, Female Reproductive Organs Small and Large Intestine Lower part of Kidney Half of Bladder, Appendix, Female Reproductive Organs Stomach, Tail of Pancreas Tail of Liver Small and Large Intestine Upper Part of Kidney Liver, Gallbladder, Stomach (Small Part) Small and Large Intestine Head of Pancreas Upper Part of Kidney Lower
 Small and Large Intestine Head of Pancreas Upper Part of Kidney. Lower.")
5
Layers of anterior abdominal wall
Skin Fascia Camper's fascia - fatty superficial layer. Scarpa's fascia - deep fibrous layer. Muscle Rectus abdominis External oblique muscle Internal oblique muscle Transverse abdominal muscle Fascia transversalis Peritoneum

6
Four Quadrants: Midsaggital or median plane Transumbilical plane - passes through the umbilicus and disc between L3 and L4

7
To describe the location of
organs easily, the abdominopelvic cavity may be divided into nine regions by drawing four imaginary lines. Nine Regions: Subcostal plane - passing thro’ the inf. border of the 10th costal cartilages (LV3). Transtubercular plane – passing thro’ the tubercles of the iliac crests (LV5). Transpyloric plane- Sometimes used; halfway between the jugular notch and the upper border of the symphysis pubis. Midclavicular plane
. Transtubercular plane – passing thro’ the tubercles of. the iliac crests (LV5). Transpyloric plane- Sometimes. used; halfway between the. jugular notch and the upper. border of the symphysis pubis. Midclavicular plane.")
9
Layers of the anterior abdominal wall
Skin Superficial fascia Camper's fascia dartos muscle Scarpa's fascia Colles' fascia Muscle External oblique Internal oblique Transversalis abdominus Transversalis fascia Peritoneum

11
Superficial fascia is divided
into: Superficial fatty layer (Camper's) Deep membranous layer (Scarpa's) • Camper's s fascia is continous with superficial fascia over the rest of body • Scarpa's fascia fades out laterally and above
 Deep membranous layer (Scarpa s) • Camper s s fascia is continous with superficial fascia over the rest of. body. • Scarpa s fascia fades out laterally and above.")
12
Superficial veins of anterolateral abdominal wall
Superficial fatty (Camper's) contains superficial veins. Above - via lateral thoracic vein into axillary vein Below via superficial epigastric + great saphenous veins into femoral vein Paraumbilical portal
 contains superficial veins. Above - via lateral thoracic vein into axillary vein. Below via superficial epigastric + great saphenous veins into femoral vein. Paraumbilical portal.")
13
Lateral thoracic Thoracoepigastric Paraumbilical Sup. circumflex iliac Sup. epigastric

14
Superficial lymphatics of anterolateral abdominal wall
Superior to the umbilicus drain to the axillary lymph nodes; a few drain medially and deeply to the parasternal and anterior diaphragmatic lymph nodes. Inferior to the umbilicus drain to the superficial inguinal lymph nodes.

16
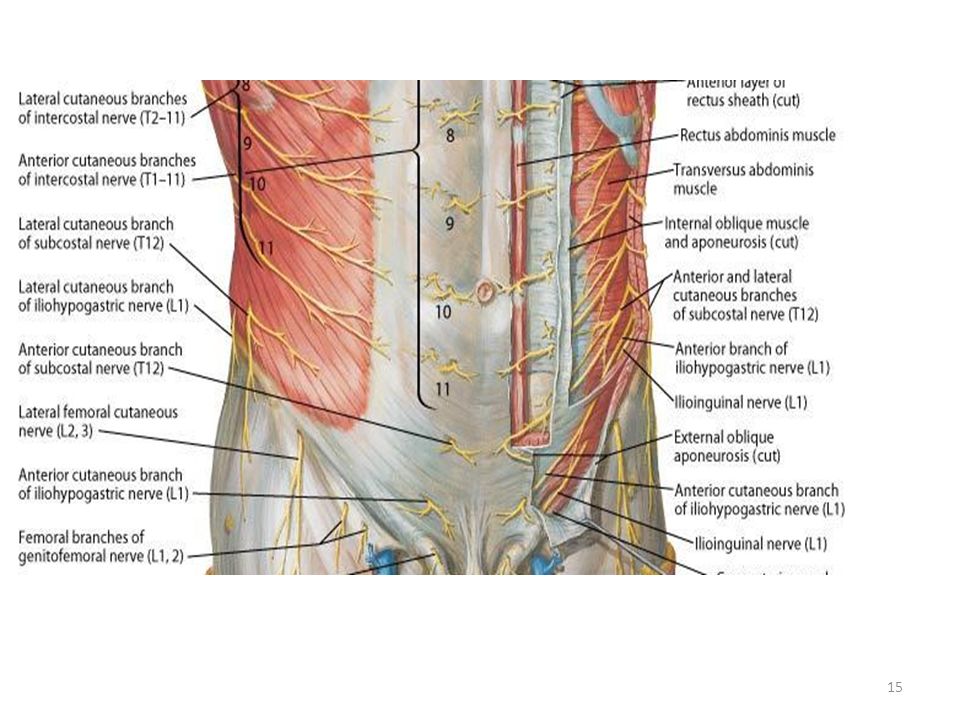
Cutaneous nerve supply to anterior abdominal wall
Anterior rami of lower 6 thoracic (T7-T12) lower 5 intercostal + subcostal nerves 1st lumber nerves iliohypogastric + ilioinguinal
 lower 5 intercostal + subcostal nerves. 1st lumber nerves iliohypogastric + ilioinguinal.")
17
Arteries 5 intercostal arteries subcostal arteries 4 lumbar arteries
Superior epigastric artery—internal thoracic artery Inferior epigastric artery -external iliac artery Deep iliac circumflex artery- external iliac artery

18
Langer's lines of the skin
Langer's lines, also called cleavage lines correspond to the alignment of collagen fibers within the dermis. Usually, a surgical cut is carried out in the direction of Langer's lines, and incisions made parallel to Langer's lines generally heal better and produce less scarring.

19
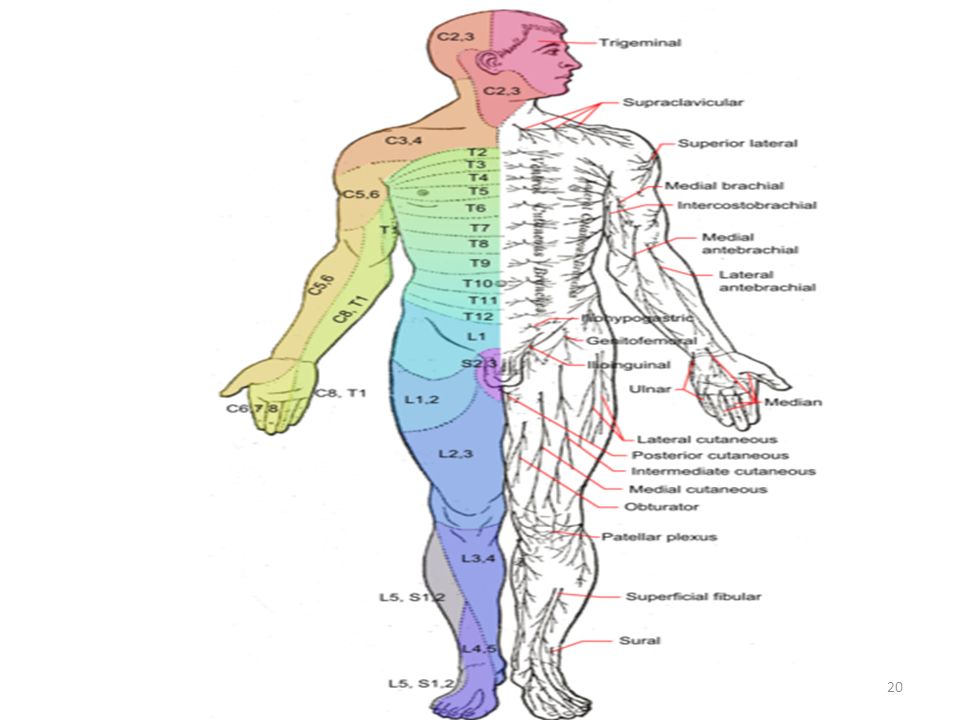
Dermatomes - Relationship between the spinal nerve & skin
Myotomes - Relationship between the spinal nerve & muscle Spinal Cord Segmental Dermatomes Dermatome ( Greek word= skin cutting. A dermatome is an area of the skin supplied by nerve fibers originating from a single dorsal nerve root. The dermatomes are supplied as follows: T7 - epigastrium T10 - umbilicus L1 - inguinal ligament

22
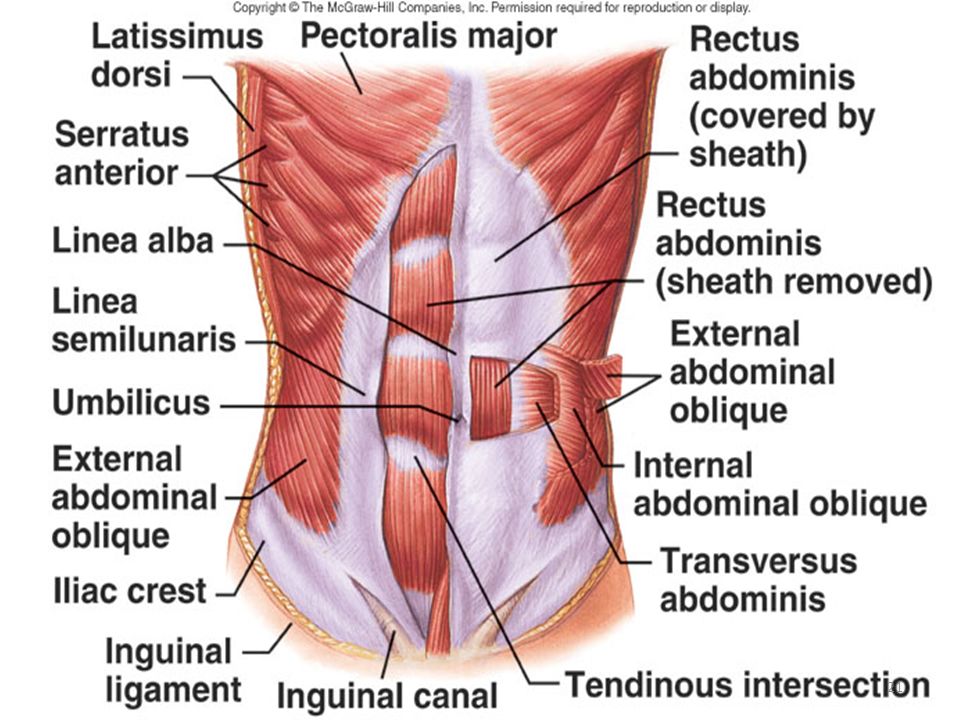
Muscles of the Anterolateral Abdominal Wall

23
Muscles The muscles of the anterior and lateral abdominal walls are:
External oblique Internal oblique Transversus abdominis Rectus abdominis Pyramidalis

24
Rectus abdominis muscle
This is a long, broad, strap-like muscle and is the principle vertical muscle of the anterior abdominal wall. O: pubic symphysis and pubic crest. I: xiphoid process and 5th to 7th costal cartilages. N: ventral rami of inferior six thoracic nerves. Act: Flexes vertebral column, depresses ribs and compresses abdomen. The two muscles are separated by the linea alba and lie close together inferiorly. The rectus abdominis is three times as wide superiorly as it is inferiorly.

25
Rectus abdominis muscle ( Cont.)
Linea semilunaris is a curved line or groove (convex laterally) that extends from the 9th costal cartilage to the pubic tubercle. This indicates the lateral border of the rectus abdominis muscle. Enclosed in the rectus sheath The anterior layer of the rectus sheath is firmly attached to the rectus muscle at three or more tendinous intersections.They are usually located at the level of the xiphoid process, umbilicus, and halfway between this structures.
 that extends from the 9th costal cartilage to the pubic tubercle. This indicates the lateral border of the rectus abdominis muscle. Enclosed in the rectus sheath. The anterior layer of the rectus sheath is firmly attached to the rectus muscle at three or more tendinous intersections.They are usually located at the level of the xiphoid process, umbilicus, and halfway between this structures.")
26
External oblique muscle
O: External surfaces of 5th to 12th ribs. I: Linea alba, pubic tubercle and anterior half of the iliac crest. N: Inferior six thoracic nerves and subcostal nerves. Act.Compresses abdomen; depresses ribs; Jointly: flex vertebral column; Individually: rotation and lateral flexion. Muscle fiber direction is antero-inferior (like external intercostals - hands in pocket). EO aponeurosis ends medially in the linea alba. Inferiorly form the inguinal ligament between the anterior superior iliac spine and the pubic tubercle. superficial inguinal ring.an opening in the aponeurosis Just superior to the medial part of the inguinal ligament. Some fibres of the inguinal ligament cross the linea alba and attach to the opposite pubic crest. These fibres form the reflex inguinal ligament.
. EO aponeurosis ends medially in the linea alba. Inferiorly form the inguinal ligament between the anterior superior iliac spine and the pubic tubercle. superficial inguinal ring.an opening in the aponeurosis Just superior to the medial part of the inguinal ligament. Some fibres of the inguinal ligament cross the linea alba and attach to the opposite pubic crest. These fibres form the reflex inguinal ligament.")
27
- It arches over spermatic cord (or round lig. of uterus), then
The Internal Oblique Muscle O: thoracolumbar fascia, anterior two-thirds of iliac crest, and lateral half of inguinal ligament. I: inferior borders of last three ribs, linea alba, and the pubic crest via the conjoint tendon. N: ventral rami of inferior six thoracic and first lumbar nerves. Act. The same as EO muscle The aponeurosis splits to form a sheath for the rectus abdominis muscle. Lower, free border of IO - It arches over spermatic cord (or round lig. of uterus), then descend behind to attach to pubic crest and pectineal line - Near their insertion it is joined by lowest tendinous fibres fromTA to form conjoint tendon Function of conjoint tendon -to strengthen the medial 1/2 of posterior wall of inguinal canal.
, then. descend behind to attach to pubic crest and pectineal line. - Near their insertion it is joined by lowest tendinous fibres. fromTA to form conjoint tendon. Function of conjoint tendon -to strengthen the medial 1/2 of. posterior wall of inguinal canal.")
28
Transversus abdominis This is the innermost of the three flat abdominal muscles. O: Internal surfaces of 7th to 12th costal cartilages, thoracolumbar fascia, iliac crest, and lateral third of inguinal ligament. I: Linea alba (with aponeurosis of internal oblique), pubic crest, and pecten pubis (via conjoint tendon). N: Ventral rami of inferior six thoracic and first lumbar nerves. A. Compresses abdominal cavity
, pubic crest, and pecten pubis (via conjoint tendon). N: Ventral rami of inferior six thoracic and first lumbar nerves. A. Compresses abdominal cavity .")
29
Pubic Symphysis

30
Layers of the Abdominal Wall

32
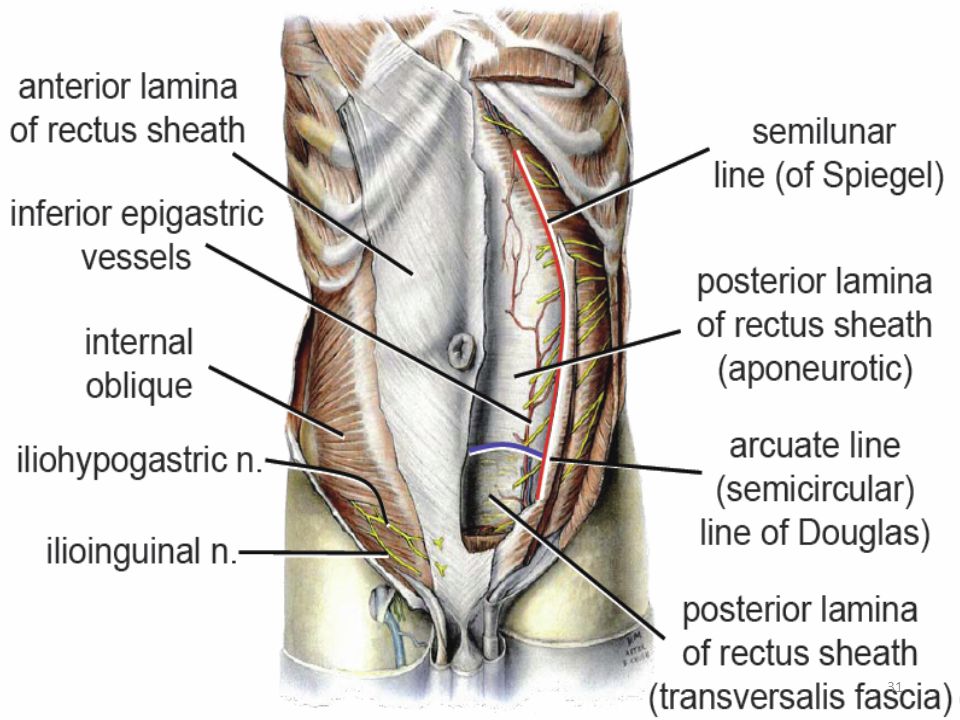
Rectus sheath Long fibrous sheath which encloses rectus abodminis and pyramidalis (if present) Rectus sheath is formed by: aponeuroses of 3 lateral abdominal muscles Aponeurosis of IO splits into 2 • anterior lamina fuses with aponeurosis of EO • posterior lamina fuses with aponeuorsis of TA Above the Arcuate line (at level of anterior superior iliac spine) All 3 aponeuroses pass anteriorly to rectus muscle so, sheath deficient posteriorly below this level. Posterior wall of rectus sheath it's not attached to rectus abdominis muscle.
 All 3 aponeuroses pass anteriorly to rectus muscle so, sheath deficient posteriorly below this level. Posterior wall of rectus sheath. it s not attached to rectus abdominis muscle.")
33
Rectus sheath Above semicircular line of Douglas/Arcuate line (midway between symphysis pubis and umbilicus): Anterior rectus sheath = external oblique aponeurosis and anterior lamina of internal oblique aponeurosis. Posterior rectus sheath = posterior lamina of internal oblique aponeurosis and aponeuorsis of TA.

34
Below semicircular line of Douglas: Anterior rectus sheath = aponeurosis of external, internal oblique, transversus Posteriorly- deficient below this level, only transversalis fascia is present. Arteries: Superior epigastric (branch of internal thoracic), inferior epigastric (branch of external iliac), both arteries anastomose and lie behind the rectus muscle.
, inferior epigastric (branch of external iliac), both arteries anastomose and lie behind the rectus muscle.")
35
Rectus sheath contains:
Rectus sheath encloses rectus abdominis and pyramidalis muscle (if present) Contains anterior rami of lower six thoracic nerves Also contains superior epigastric artery (continuation of the internal thoracic artery) and inferior epigastric artery (from external iliac artery). Lymph vessels
 Contains anterior rami of lower six thoracic nerves. Also contains superior epigastric artery (continuation of the internal thoracic artery) and inferior epigastric artery (from external iliac artery). Lymph vessels.")
36
Arcuate line lower, crescent-shaped edge of the posterior wall of rectus sheath. At this level inferior epigastric vessels enter the rectus sheath Linea alba A fibrous band, made by the fusion of all 3 aponeuroses with their fellows of opposite side in middle Extends from xiphoid to pubic symphisis

38
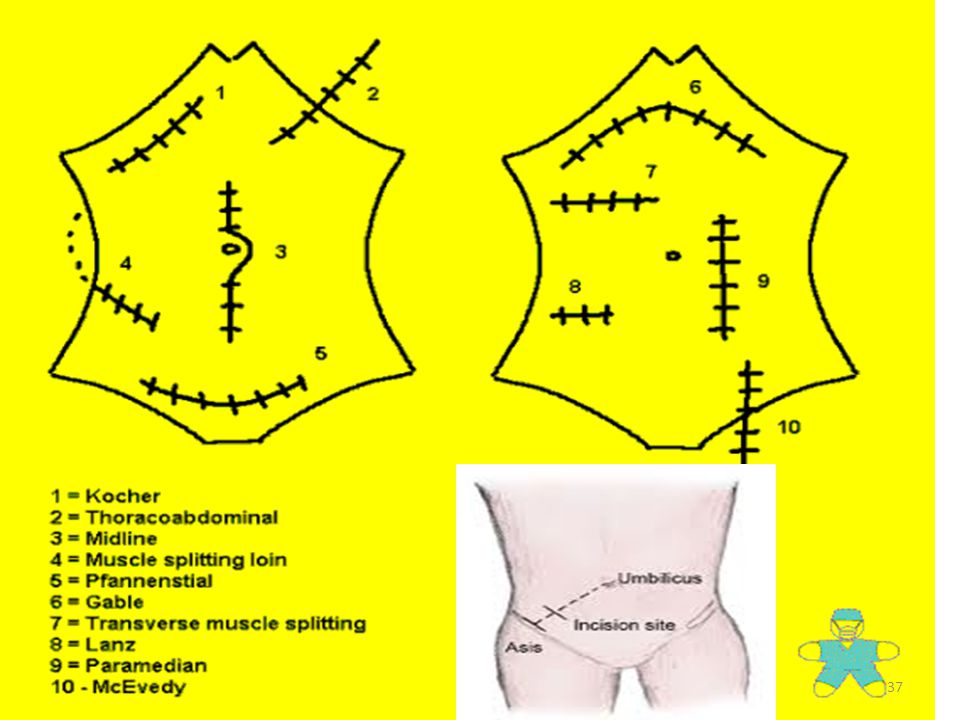
Midline General access. Usually skirts the umbilicus
Midline General access. Usually skirts the umbilicus. Quick and bloodless Paramedian General access. Left or right according to requirements. Kocher (Subcostal) Biliary or hepatic procedures. May be extended across to a left subcostal incision to give useful access to the stomach and pancreas. McBurney – 1/3 of the way along the line from the anterior superior iliac spine to the umbilicus Appendicectomy. Muscle layers are split, rather than cut. Transverse Skin incision crosses fewer dermatomes General access. Almost always used in infants, and often in adults. Rutherford Morison Access to sigmoid colon and pelvis, particularly if the midline is very scarred from previous surgery. Pfannenstiel For Caesarian sections and urological surgery. Good cosmetic result but gives no access outside the pelvis
 Biliary or hepatic procedures. May be extended across to a left subcostal incision to give useful access to the stomach and pancreas. McBurney – 1/3 of the way along the line from the anterior superior iliac spine to the umbilicus Appendicectomy. Muscle layers are split, rather than cut. Transverse Skin incision crosses fewer dermatomes General access. Almost always used in infants, and often in adults. Rutherford Morison Access to sigmoid colon and pelvis, particularly if the midline is very scarred from previous surgery. Pfannenstiel For Caesarian sections and urological surgery. Good cosmetic result but gives no access outside the pelvis")
39
Layers of the abdominal wall, inguinal canal and their relations to
the spermatic cord and testies

40
Descent of Testis Through Inguinal Canal to Scrotum
Transversalis fascia– deep ring/internal spermatic fascia Peritoneum forming processus vaginalis/tunica vaginalis testis Transversus abdominis Internal oblique— cremaster muscle External oblique— superficial ring/ external spermatic fascia Gubernaculum

41
Layers of scrotum skin dartos muscle external spermatic fascia cremastric fascia internal spermatic fascia peritoneum, tunica vaginalis Coverings of spermatic cord (Spermatic fascia) 3 concentric layers of fascia derived from layers of anterior abdominal wall: • external spermatic fascia -derived from EO • cremasteric fascia -derived from IO • internal spermatic fascia- derived from fascia transversalis attached to margins of deep inguinal ring
 3 concentric layers of fascia derived from layers of anterior. abdominal wall: • external spermatic fascia -derived from EO • cremasteric fascia -derived from IO • internal spermatic fascia- derived from fascia transversalis. attached to margins of deep inguinal. ring.")
42
Structures of spermatic cord • vas deferens • artery of the ductus deferens (from the inferior vesical artery ) • testicular artery (from aorta) • testicular veins (pampiniform plexus) • testicular lymph vessels • autonomic nerves • remains of processus vaginalis • cremasteric artery (from the inferior epigastric artery). • genital branch of genitofemoral nerve (supplies cremaster muscle)
 .")
44
The Inguinal Region

45
4cm tunnel in lower, anterior abdominal muscles and lies
The Inguinal Region It is an area of weakness in the anterior abdominal wall because of the prenatal penetration of the wall by the testis and the spermatic cord. . Inguinal canal 4cm tunnel in lower, anterior abdominal muscles and lies parallel to and immediately above, the inguinal ligament. It runs downwards and medially between the deep and superficial rings. Walls of the Inguinal Canal: Anterior Posterior Superior Inferior

46
Inguinal (Hesselbach's) triangle
An anatomic area of the abdominal wall bounded by: Suprolateral: inferior epigastric vessels Medial: lateral margin of the rectus muscle Inferior: The inguinal ligament /Poupart's ligament Clinical significance Direct inguinal hernias leave the abdomen through this triangle.

47
Contents of Inguinal Canal
Spermatic Cord (male) or Round ligament (female) Ilioinguinal nerve Genital branch of the genitofemoral nerve.
 or Round ligament (female) Ilioinguinal nerve. Genital branch of the genitofemoral nerve.")
48
Superficial Inguinal Ring
Triangular -shaped defect in the aponeurosis of the external oblique Immediately above and medial to the pubic tubercle Margins give origin to the external spermatic fascia Physical exam - to differentiate bet. direct & indirect inguinal hernias

49
Deep Inguinal Ring 3cm superior to the midpoint of the inguinal ligament. Lateral to the inferior epigastric vessels Margins of ring give origin to the internal spermatic fascia

50
Inguinal Anatomy

51
Walls of the inguinal canal
Anterior wall Aponeurosis of ext. oblique ♦ Reinforced laterally by the fibres of the internal oblique ■ Strongest where it lies opposite the weakest part of the posterior wall (deep ring).
.")
52
Walls of the Inguinal Canal
Posterior wall Formed throughout by the transversalis fascia ♦ reinforced medially by the conjoint tendon. ■ Strongest where it lies opposite the weakest part of the anterior wall (superficial ring).
.")
53
Walls of the Inguinal Canal
Inferior (floor) The superior surface of the inguinal ligament and the lacunar ligament. Superior (roof) Arching lowest fibers of the Int. oblique and transversus abdominis muscles.
 The superior surface of the inguinal ligament and the lacunar ligament. Superior (roof) Arching lowest fibers of the Int. oblique and transversus. abdominis muscles.")
54
Lacunar ligament (Gimbernat’s ligament)
Medial curved fibres of inguinal ligament that pass upwards and backwards to attach to pectineal line . Pectineal ligament A thickening of periosteum

55
Two important physiolgical mechanismsShutter and Closure mechanims protect the formation of inguinal herniae with increased abdominal pressure. The arching fibres of the internal oblique and transversus abdominis contract when the muscles of the abdomen contract. This acts as a shutter on the posterior wall to protect it from herniation. This is termed the Shutter Mechanism. In addition this contraction also narrows the deep ring. The narrowing of the deep ring is termed the Closure Mechanism.

56
Indirect Inguinal Hernia through Inguinal Canal
Congenital (or adult) Through inguinal canal (and deep ring) Lateral to inferior epigastric artery Could be in patent processus vaginalis
 Through inguinal canal. (and deep ring) Lateral to inferior. epigastric artery. Could be in patent. processus vaginalis.")
57
Direct inguinal hernia
Enter the inguinal triangle NOT through the inguinal canal Medial to inferior epigastric artery X

58
Above and medial to the pubic tubercle
The hernial sac thus lies inferior and lateral to the pubic tubercle

59
Inguinal (Hasselbach's) triangle
 triangle")
60
b

61
Urinary extravasation
Rupture of spongy urethra is common in straddle injury that results in extraperitoneal extravasation of urine within the superficial perineal pouch and extending into the scrotal, penile, and fatty layer of subcutaneous connective of the lower anterior abdominal wall areas. Any fluid (blood, urine, or pus) that is within the superficial pouch will be limited by Colle’s fascia and its attachments. Urinary extravasation
 that is within the superficial pouch will be limited by Colle’s fascia and its attachments. Urinary extravasation.")
62
THANK YOU

Similar presentations