Download presentation
Presentation is loading. Please wait.

1
Objectives: Anorexia/Cachexia/Fatigue 1.Describe the anorexia-cachexia syndrome in advanced illness, and it’s potential causes 2.Describe the clinical implications of the pathophysiological mechanisms of cachexia and anorexia in patients with advanced cancer and AIDS. 3.List three pharmacological agents that could improve appetite in patients with advanced cancer or AIDS. 4.Describe causes of cancer-related fatigue. 5.Discuss evidence based management of fatigue in patients with advanced cancer.

3
Cancer Cachexia Cancer cachexia is a multi-factorial syndrome defined by an ongoing loss of skeletal muscle mass (with or without loss of fat mass) that cannot be fully reversed by conventional nutritional support and leads to progressive functional impairment. The pathophysiology is characterized by a negative protein and energy balance driven by a variable combination of reduced food intake and abnormal metabolism. EPCRC Fearon et al. Lancet Oncology online 05 Feb 2011

5
Immune cells regulating tumor growth Stimulate Cancer Growth Innate immune cells neutrophils macrophage (M2) myeloid-derived suppressor cells Adaptive immune cells Th2 CD4 + T cell CD4 + T regulatory cell B lymphocytes Adapted – Disis – JCOOct 10 2010 Inhibit Cancer Growth macrophage (M1) Cytotoxic CD8 + T cell Th1 CD4 + T cell TH17 CD4 + T cell
 myeloid-derived suppressor cells Adaptive immune cells Th2 CD4 + T cell CD4 + T regulatory cell B lymphocytes Adapted – Disis – JCOOct Inhibit Cancer Growth macrophage (M1) Cytotoxic CD8 + T cell Th1 CD4 + T cell TH17 CD4 + T cell")
6
Metabolic changes in tumour related weight loss insulin resistance diminished lipogenesis increased lipolysis increased protein anabolism – liver acute phase protein response – CRP inflammatory cytokines (Il-1β, Il-6, Il-10, others – innate immune system) REE
 REE")
7
Fat Metabolism zinc α-1 glycoprotein catecholamine sensitivity Lipase activity (ATGL – HSL) FFA fat loss muscle muscle wasting
 FFA fat loss muscle muscle wasting")
8
Inflammation Immuno-neuroendocrine aberrations 1. CRF – cortisol 2. sympathetic activity Cytokine activity Pulse –REE Psychosocial stress 3. testosterone Hypogonadism sex drive activity

10
STRESS HPA Cortisol Autonomic tone Norepinephrine and Metastatic Risk Tumor Growth Inflammatory Factors (Modeled on Lutgendorf et al, JCO - 2010; 28-4094 )
")
11
Catecholamines Advanced cancer – Stressful! Nor-eph and eph Animal Tumour growth Metastases Inflammation (Innate side) Humans REE Effects on cachexia ? Effects on tumours?
 Humans REE Effects on cachexia . Effects on tumours .")
12
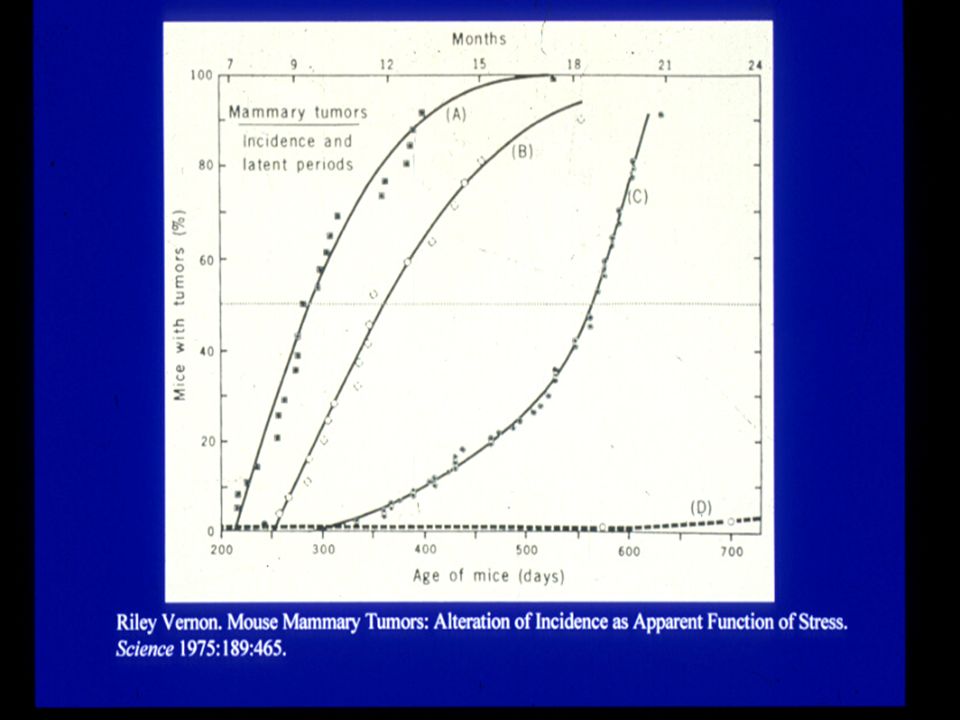
Stress Basic data Yang et al …………………………………. Cytokines Tumor cell lines Human melanoma Ben Eliyahu ……………………………… Survival Mouse tumor models Post surgery Etodolac and Propanolol Lee et al……………………………………….. Human Ovarian nude mice Propranolol Reiche et al………………………………….. Stress hormone Switch from Th1 to Th2 immune response

13
Activation of microglial cytokines CNS Hypothalamus MC4 Sympathetic tone REE Norepinephrine Circulating cytokines Balance Vagal Input anorexia

14
SatietyAppetite Hypothalamus MC4R leptin vagus Food Intake POMC ghrelin vagus Neuropeptide Y AGRP Food Intake Cerebrum (Hedonistic Centre Cerebrum Hedonistic Centre? STN

15
CHRONIC INFLAMMATION LIVER ↑AFP (note CRP) ↓drug metabolism MUSCLE ↓synthesis ↑proteolysis HYPOTHALAMUS ↓appetite ↑sympathetic activity ↑REE ↑cortisol ↓testosterone GUT early satiety BRAIN depression FAT ↑lipolysis ↓lipoprotein lipase TUMOUR CRP
 ↓drug metabolism MUSCLE ↓synthesis ↑proteolysis HYPOTHALAMUS ↓appetite ↑sympathetic activity ↑REE ↑cortisol ↓testosterone GUT early satiety BRAIN depression FAT ↑lipolysis ↓lipoprotein lipase TUMOUR CRP")
17
21.519.915.78.4 14.211.910.510.6 10.76.89.26.7 8.1 6.25.4 BMI kg/m 2 Weight loss % 28 25 22 20 2.5 6 11 15 7.8 4.7 4.4 4.13.74.74.87.1 13.5 Risk of Mortality is a Simultaneous Function of Body Mass Index and Weight Loss in Patients with Advanced Solid Tumors Martin et al J Clin Oncol 2014 Median survival, months Different colors denote p<0.001 adjusted for age, sex, site, stage and Performance Status N=8160 N= 150-750 in each of 25 cells

18
Median survival by CRP Trajectory Median survival (months) 95% CI Normal Normal 21.611.9-31.6 Normal Abnormal 12.36.5-18.1 Abnormal Normal 10.77.6-13.5 Abnormal Abnormal 8.37.0-9.5 Log Rank (Mantel-Cox)<0.001 JCO suppl. 2009 abstract 8092

19
Chronic Inflammation - Cancer Immune response often facilitates tumor progress Tumor cells produce inflammatory chemical mediators assisting growth Inflammatory mediators enhance many cancer symptoms Early evidence – anti-inflammatory agents may modify the course of cancer Will anti-inflammatory (palliative) therapies improve life quality and quantity? Relief of cachexia - survival?

21
Mechanisms of secondary cachexia Impaired oral intake – cognitive impairment, delirium – depression, fatigue – pain, dyspnoea, other uncontrolled symptoms – stomatitis, taste alteration – dry mouth – dysphagia, odynophagia – gastric stasis – bowel obstruction – nausea & vomiting – severe constipation

22
Anorexia Drugs I Corticosteroids Dexamethasone (Decadron) Action – general anti-inflammatory Use – limited in our practice – Highly catabolic Progestational agen ts
 Action – general anti-inflammatory Use – limited in our practice – Highly catabolic Progestational agen ts")
23
Anorexia Drugs III Cannabinoids – marijuana, dronabinol, cesamet Action - multiple actions? – “reward centres” Use – underutilized – Increases taste and food enjoyment

24
Cachexia Drugs I - Anabolic Agents SARMS– Selective Androgen Receptor Modulators Action – ‘Pure Anabolic’ Use – 1. Definite LBM 2. Safe 3. Increased Function? Status – Limbo – Phase III trials ± Future – Combine with exercise, nutrition

25
Cachexia Drugs Ghrelin (Hormone) Action – anti – inflammatory – Appetite (hypothalamus) – Gastric Motility – REE – LBM Risk - !! – stimulate cancer? inhibit cancer? 2016 – NSCLC trial (Lancet) LBM – Weight But not Hand Grip
 LBM – Weight But not Hand Grip.")
26
Exercise Endurance Animals tumour size food intake Human- survivors fatigue muscle and function Resistance Elderly +++ Cancer cachexia FOXO action MyoD Myostatin Antioxidant activity

27
Anorexia-cachexia Program Therapies reflect physiology Multimodal approach Cancer therapy – Cachexia therapy paired Introduce early – at the time of 1 st diagnosis

28
PHYSICIAN ONCOLOGISTS Medical Intervention PHYSIOTHERAPIST Functional Evaluation and Rehabilitation DIETITIAN Nutritional Evaluation and Recommendations NURSING, PSYCHOLOGIST, OCCUPATIONAL THERAPIST, SOCIAL WORKER PATIENT AND FAMILY Slide courtesy Nelda Swinton

29
Program 8 – 10 weeks with clear initial and end evaluation Nutritional counselling Basic intervention= physio 1-2 times /week 1 visit / 2 weeks other team members Caregiver information Weekly psycho-education groups – meet once /week x 9 rotating sessions

30
Workup Questionnaires ESAS Distress PG-SGA CHAMPS CRP WBC Testosterone - bioavailable Thyroid

31
Expected Benefits from Exercise Physical Benefits Muscle mass, muscle strength, flexibility, cardiovascular fitness and fatigue Psychological Benefits Stress, anxiety, sleep quality, depression Sociological Benefits Self esteem, efficacy, connectedness, ADL’s & QoL General Health Benefits Circulation, immune response, lipid profiles

32
Program Assessment 1.Symptom Control 2.Muscle – Strength Static Function Dynamic Function 3.Psychosocial Function 4.Anorexia – Weight 5.Quality of Life 6.Patient – Family Satisfaction

33
Changes in Activity Function N = 65N = 67 * * * p < 0.05 vs. Initial

34
Changes in Weight N = 122

35
Changes in Psychosocial Function Note: Higher scores indicate worse symptoms N = 126 * * p < 0.05 vs. Initial

36
Changes in Symptom Severity N = 130 Note: Higher scores indicate worse symptoms * p < 0.05 vs. Initial

37
Changes in Family – Patient Satisfaction Testimonial I feel I have been remiss in not writing to you sooner. I cannot say enough about how positive I felt being involved with your team. The thing that impressed me most was your profound respect for me. I think that this was only surpassed by the admiration and respect you had for each other. This allowed me to open up and be more trusting. I knew that anything I shared of value and significance was relayed to other team members. My wife and I were no longer on our own. Simple things seemed to take on profound meaning "you need to eat more", "don't feel guilty about resting" "You don't have to endure the pain, that's why we give you medication", are a few of the things that come to mind. As I write I realize that the most important thing was that WE felt we were part of a team and that made all the difference. Thank you all so much

38
Evaluation High patient satisfaction Advanced cancer patients can exercise CRP status determines completion of an exercise program Significant improvement in: -symptoms -nutrition -function -psychosocial factors

39
*p<0.05 **p<0.01 ***p<0.001 *Baseline is sig higher than other timepoints **Baseline is sig higher than other timepoints

40
*p<0.05 **p<0.01 ***p<0.001 Baseline is sig higher than completion* and 3-month follow-up**

41
Case 1 Mr DB is a 64-year-old man with unresectable pancreatic cancer. He was diagnosed four months previously and received palliative gemcitabine chemotherapy. The chemotherapy has been helpful for his pain but he has become very cachectic and has lost 15 kg in weight in the last three months. He has no appetite and feels very fatigued. His wife is distressed. She asks of you: “He does not eat and will starve to death! Can’t you feed him intravenously?” LEAP version 1.1 – Canadian Pallium Project

42
Case 2 (Part 1 of 2) Mrs ML is a 56-year-old woman who was diagnosed with throat cancer two years ago. She underwent surgery (laryngectomy) and high-dose radiotherapy with curative intent. She did well for about 18 months but then discovered a mass in her left neck. Further tests showed this to be recurrence of her disease only in her neck. Her oncologist and surgeon have told her that curative treatment is not possible but she can have palliative chemotherapy to extend her life and help control symptoms. The cancer is localized and there are no metastases. LEAP version 1.1 – Canadian Pallium Project
 and high-dose radiotherapy with curative intent. She did well for about 18 months but then discovered a mass in her left neck. Further tests showed this to be recurrence of her disease only in her neck. Her oncologist and surgeon have told her that curative treatment is not possible but she can have palliative chemotherapy to extend her life and help control symptoms. The cancer is localized and there are no metastases. LEAP version 1.1 – Canadian Pallium Project.")
43
Case 2 (Part 2 of 2) In the last two months Mrs ML has been experiencing increased pain in her neck and has difficulties swallowing, particularly solid foods. She has lost 1 kg of her weight in the last month. Her husband is concerned and asks us to do something about her eating, otherwise she will “starve to death”! Mrs ML is also concerned about her weight loss as she is still very much involved in life and awaiting the birth of her first grandchild in four months. LEAP version 1.1 – Canadian Pallium Project

44
Case 3 (Part 1 of 2) Mrs AB is a 41-year-old mother of three children (aged 6, 8 and 11). She has advanced ovarian cancer for which she has undergone debulking surgery and extensive chemotherapy. She now has widespread peritoneal metastases and ultrasound evidence of liver metastases. She has developed complete bowel obstruction. The surgeon deems this to be inoperable and irreversible. She has lost 10 kg in the last three months. She feels hungry. She is very distressed and wants everything done to prolong her life. “I cannot die yet. Look how young my children are!” LEAP version 1.1 – Canadian Pallium Project

45
Case 3 (Part 2 of 2) Mrs AB’s liver function tests are normal. She has no metastases outside the abdomen. She looks cachectic. Her albumin level is 23 g/L. Her ECOG performance status is 2 but she has remained at home with her family and is still very much involved with her children. She has read about TPN and wants to have this to extend her life at least until Christmas, which is two months away. LEAP version 1.1 – Canadian Pallium Project

46
Fatigue in palliative care

47
Fatigue Cancer-related fatigue (asthenia) – Distressing, persistent, subjective sense of tiredness or exhaustion – Not proportional to activities – Interferes with usual function – Over 70% of cancer patients experience fatigue Dr Martin Chasen and Dr Ravi Bhargava
 – Distressing, persistent, subjective sense of tiredness or exhaustion – Not proportional to activities – Interferes with usual function – Over 70% of cancer patients experience fatigue Dr Martin Chasen and Dr Ravi Bhargava")
48
Symptom control in palliative care – Part II: Cachexia/anorexia and Fatigue Fabbro et al. Journal of Palliative Med, 9(2), 2006
,")
49
Management of Fatigue Rx causes if possible Multi-disciplinary team approach Exercise – Intervention with the best evidence of effectiveness – Reduces fatigue and emotional distress, improves function and QOL Education Psychosocial

50
Pharmacological agents Stimulants – Methylphenidate Usually for ADHD Possible improvement in cancer related fatigue, depressive Sx, somnolence and cognitive abnormalities – Modafinil Usually for treatment of narcolepsy Still being investigated…some evidence for patients receiving chemotherapy and with severe fatigue Corticosteroids – Temporary – Many side-effects

51
Cancer - 2016 Impeccable symptom assessment and management from point of diagnosis Symptom care married with other anti-chronic illness approaches from time of diagnosis Access to nutrition – rehabilitation programmes geared to strengthen and maintain function and control fatigue from point of diagnosis A change in research and educational priorities to reflect the above changes in the care of chronic illness A commitment to interdisciplinary collaboration to optimize patient outcomes

Similar presentations


 Dr Geraldine Swift and Dr Sonia Mangwana.>")











. - FM is one of the main causes of Chronic Widespread Pain (CWP).>")




, MBBS, FRACP MEDICAL ONCOLOGIST CONJOINT LECTURER, UNSW ST GEORGE PRIVATE HOSPITAL, KOGARAH.>")
