Download presentation
Presentation is loading. Please wait.

1
Multi-Slice CT for Coronary Calcium Scoring and Coronary Angiography John D. Symanski, M.D., F.A.C.C The Sanger Clinic, PA and Carolinas Medical Center No Disclosures

4
Objectives Show lots of pretty pictures Overview fundamental principles of MSCT technology Review strengths and limitations of MSCT Raise awareness of current indications and clinical scenarios for which to consider CT angiography

5
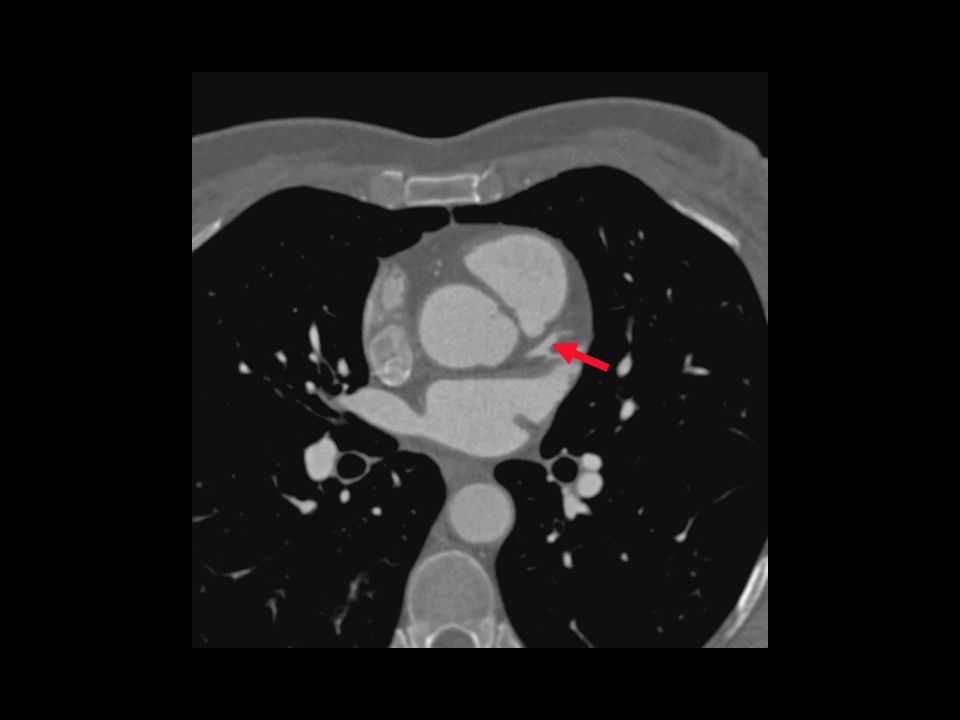
Case Presentation 64-year-old female with stage 1 CLL Dyslipidemia (untreated); No HTN, diabetes, or tobacco use Negative stress echo previously Atypical chest pain Stress echo: septal hypokinesis at rest, LVEF: 50% Referred for calcium scoring and CTA
; No HTN, diabetes, or tobacco use Negative stress echo previously Atypical chest pain Stress echo: septal hypokinesis at rest, LVEF: 50% Referred for calcium scoring and CTA")
11
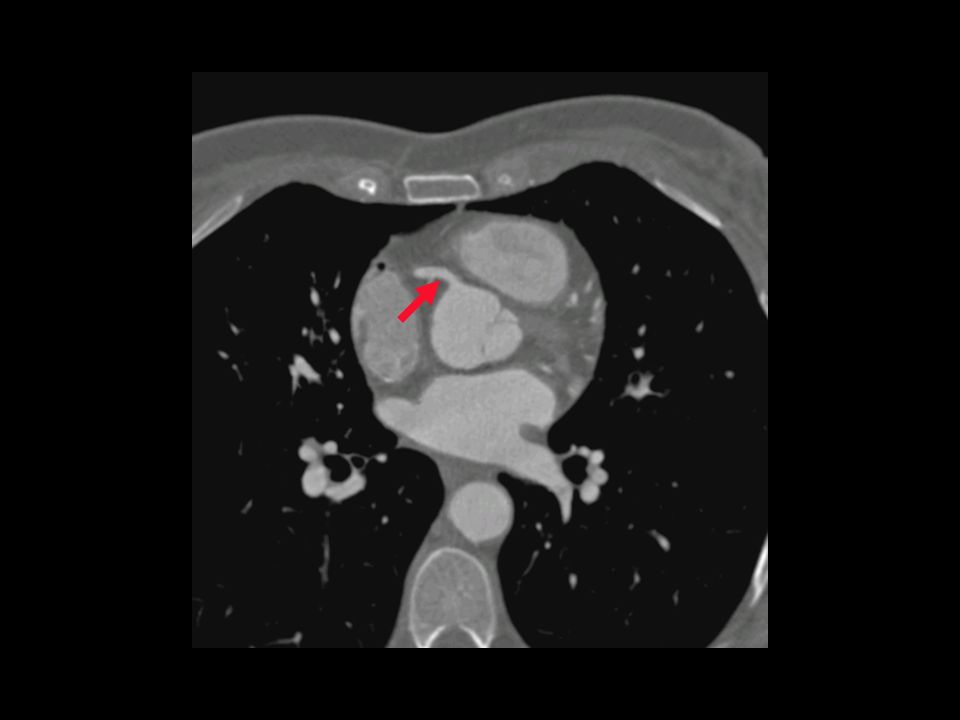
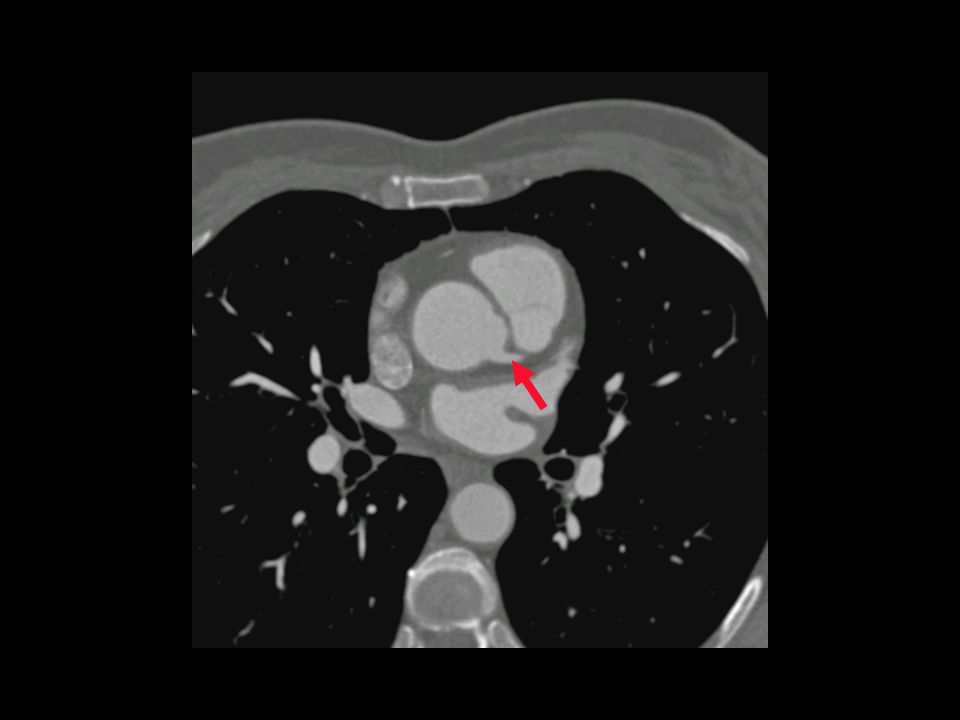
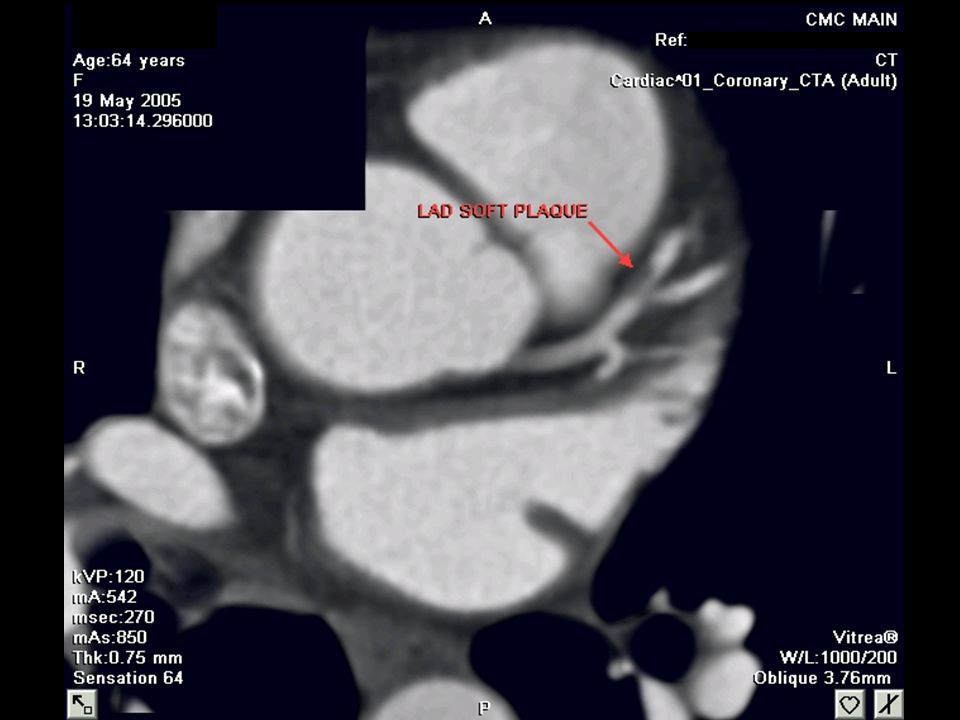
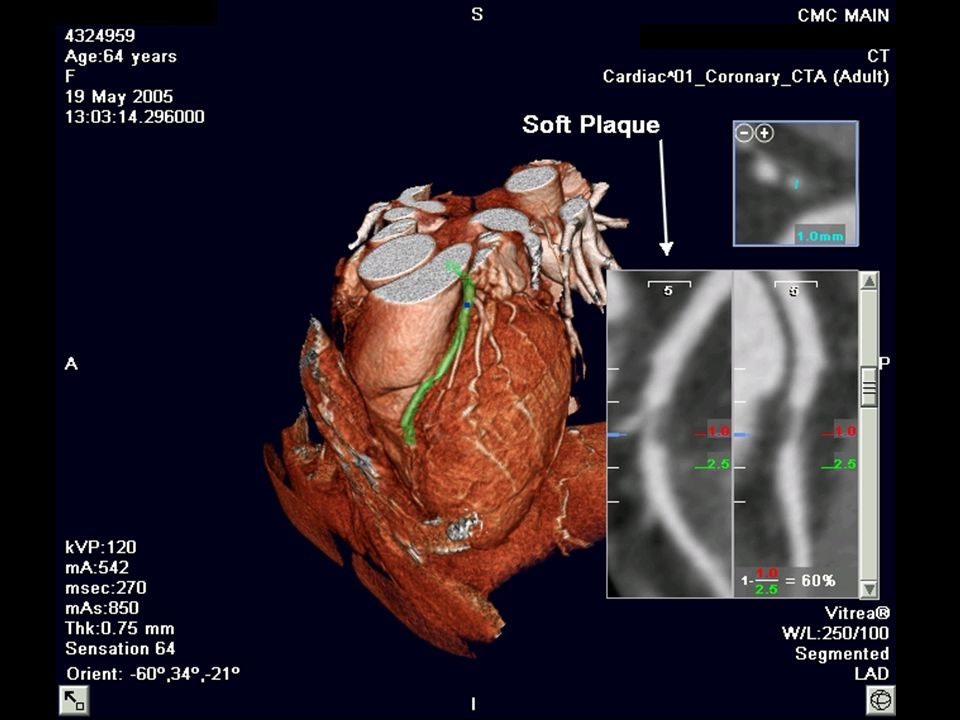
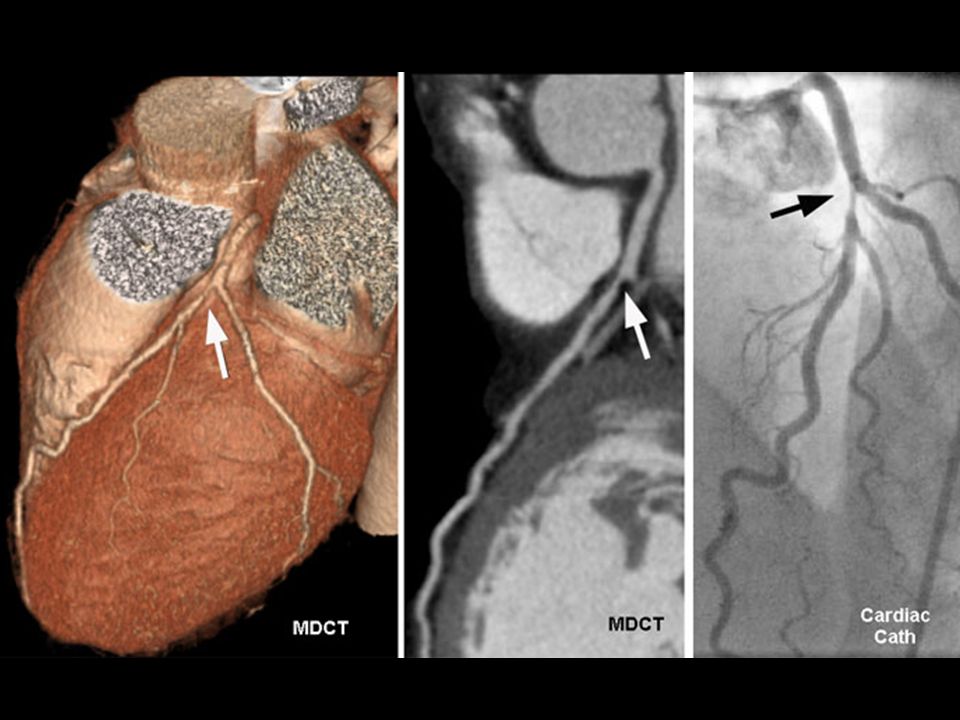
CT Angiogram Interpretation Calcium Volume Score: ZERO CT angiography: –Left Main, Circumflex, and Right coronary arteries: normal –LAD: eccentric, soft plaque adjacent to origin of first diagonal (~60% stenosis) Correlation recommended
 Correlation recommended")
14
Summary Cardiovascular Imaging - State of the Art Multi-slice CT (MSCT) not likely to replace conventional angiography Post-processing of images for MSCT angiography time & labor intensive Major strength of CTA is its high negative predictive value CMR to become the preferred cardiac imaging modality in the future
 not likely to replace conventional angiography Post-processing of images for MSCT angiography time & labor intensive Major strength of CTA is its high negative predictive value CMR to become the preferred cardiac imaging modality in the future")
15
Which Test for Which Patient? All modalities are improving No single modality fits all applications and all patients Choice of initial test depends on the specific clinical question in individual patient

16
Cardiac Magnetic Resonance

17
Viability Assessment CMR Delayed Hyper-Enhancement

18
Hazards of MRI Magnet-Seeking Projectiles

19
First whole-body CT cross-section through a human thorax, generated by Ledley et al in 1974 (Science 1974;186:207)
")
21
The Examination

22
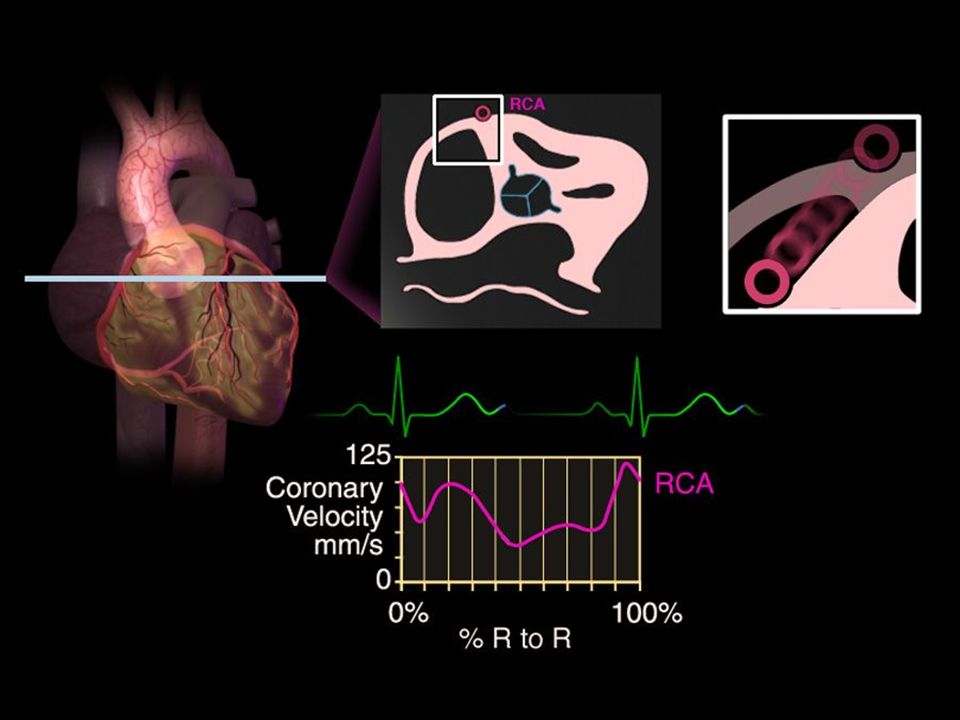
Current Generation Scanners Spatial resolution 0.4 mm - conventional coronary angiography 0.15-0.25 mm Temporal resolution (shutter speed) improved to 166 msec with faster gantry rotation (330 msec) – conventional angiography 6 msec Up to 64 slices in one rotation
 improved to 166 msec with faster gantry rotation (330 msec) – conventional angiography 6 msec Up to 64 slices in one rotation")
23
4 to 64 Slice Scans Five Heart Beats 10 mm detector Pitch ~0.25 3 cm in 5 sec 20 mm detector Pitch ~0.25 6.2 cm in 5 sec 40 mm detector Pitch ~0.25 12.5 cm in 5 sec

24
64-Slice CT Scanner More coverage (volume) with each heart beat Entire heart imaged in 5-15 seconds Less contrast required No increase in rotation speed, but with overlapping slices, can use segments from different heart beats to improve temporal resolution
 with each heart beat Entire heart imaged in 5-15 seconds Less contrast required No increase in rotation speed, but with overlapping slices, can use segments from different heart beats to improve temporal resolution")
25
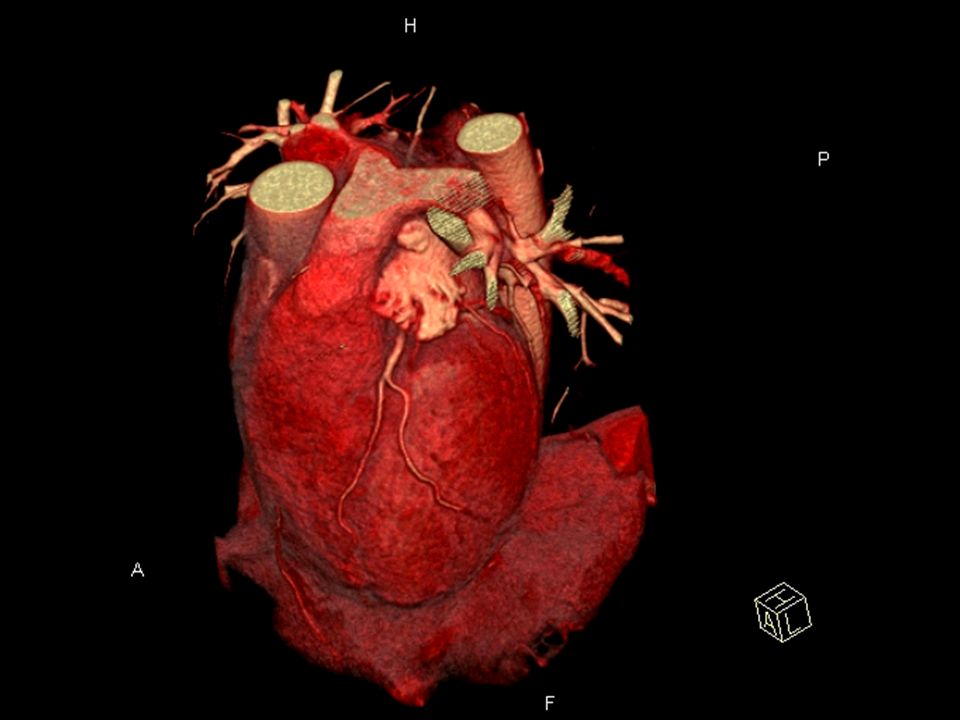
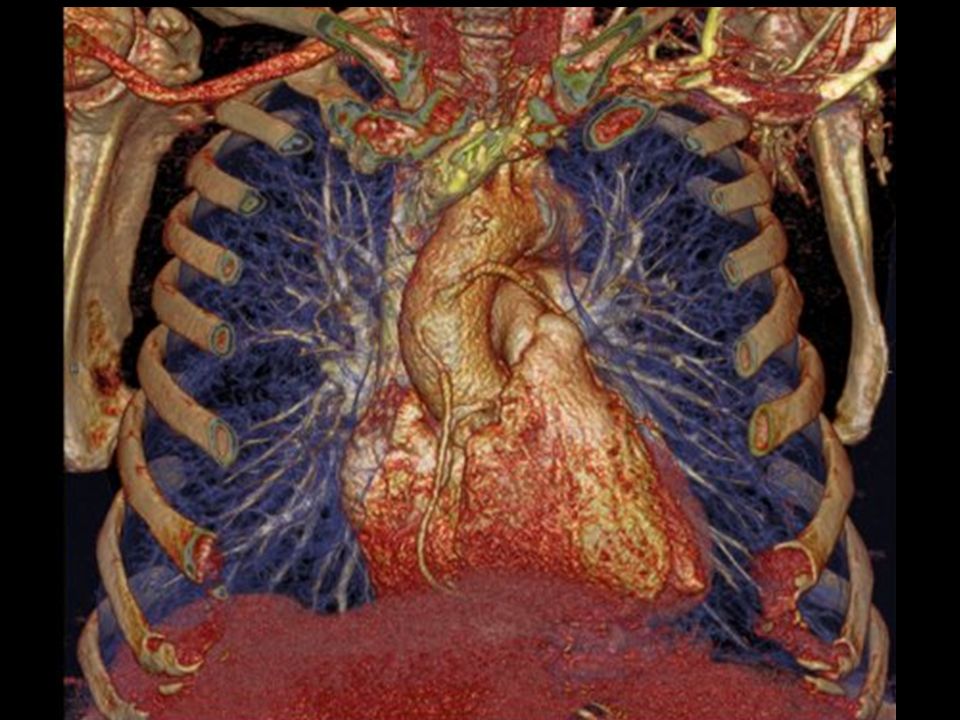
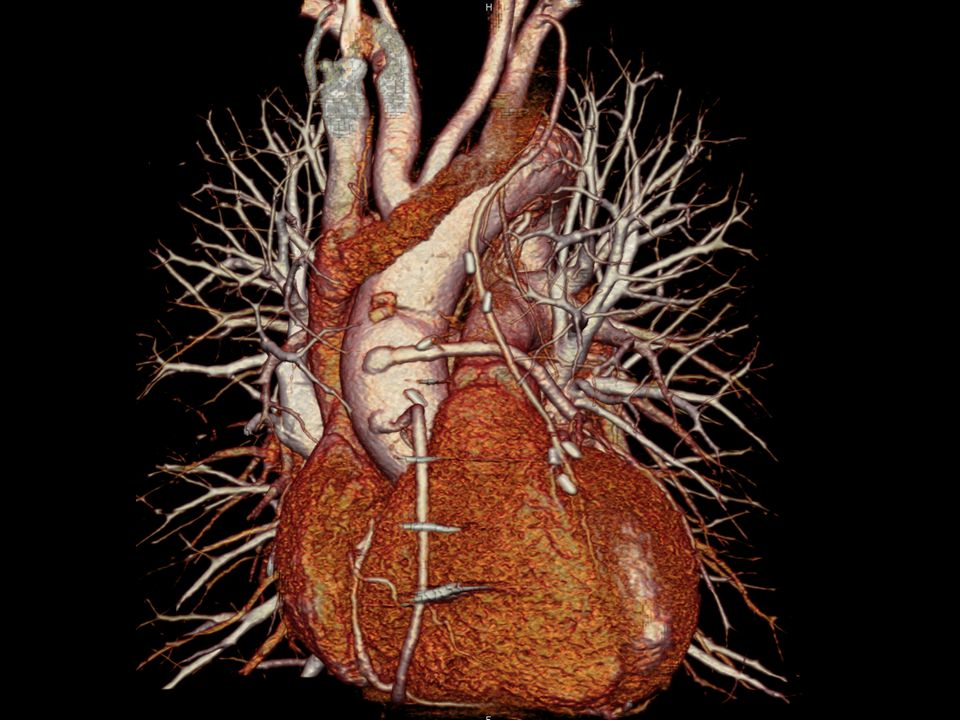
3-D Volume Rendered Image

26
Maximum Intensity Projection Soft Plaque in Proximal LAD

27
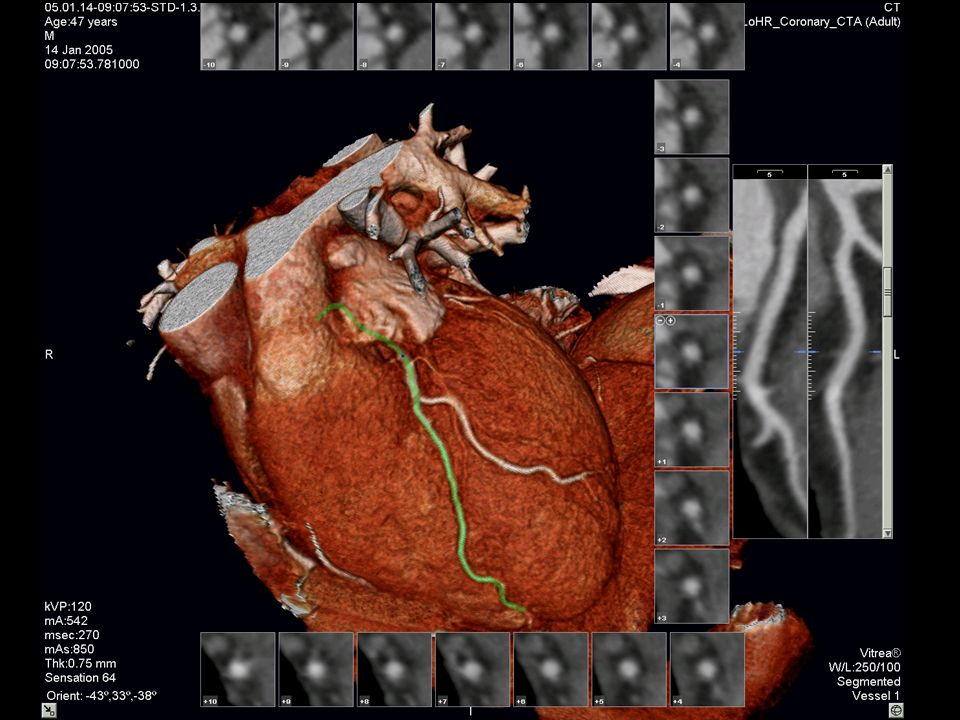
Curved Planar Image

31
Quantification of Obstructive and Nonobstructive Coronary Lesions by 64-Slice Computed Tomography 59 patients with stable angina subjected to CTA before catheter-based angio Diagnostic image quality in 55 of 59 Sensitivity for detection of stenosis 50%, and >75%: (79%, 73%, and 80%, respectively) Excellent accuracy with proximal lesions Leber AW et al. J Am Coll Cardiol. July 5, 2005;46:147-54

32
Diagnostic Accuracy of Noninvasive Coronary Angiography Using 64-Slice Spiral Computed Tomography 70 patients undergoing invasive cath Of 1,065 segments, 935 evaluated (88%) Quantitative assessment in 773 of 935 segments by MSCT and QCA Sensitivity, specificity, (+) PV, (-) PV: –By segment-(86%, 95%, 66%, and 98%) –By artery-(91%, 92%, 80%, and 97%) –By patient-(95%, 90%, 93%, and 93%) Raff GL et al. J Am Coll Cardiol. Aug 2, 2005;46:552-7.

33
Coronary Calcium Scoring Initial ACC/AHA guidelines “may be useful in selected patients”… Added prognostic power to conventional risk stratification tools (Framingham) Revised guidelines (and reimbursement for service) likely forthcoming
 Revised guidelines (and reimbursement for service) likely forthcoming")
35
Hn x-factor (Agatston Scoring) 130-199 1 200-299 2 300-399 3 >400 4 Area = 15 mm 2 Peak CT = 450 Score = 15 x 4 = 60 Area = 8 mm 2 Peak CT = 290 Score = 8 x 2 = 16 Total Score = S Calcium Volume Scoring
 >400 4 Area = 15 mm 2 Peak CT = 450 Score = 15 x 4 = 60 Area = 8 mm 2 Peak CT = 290 Score = 8 x 2 = 16 Total Score = S Calcium Volume Scoring")
36
The Calcium Scale The calcium scale is a linear scale with 4 calcium score categories: 0 none 1–99 mild 100–400 moderate >400 severe *Calcium score correlates directly with risk of events and likelihood of obstructive CAD*

37
Ethnic Differences in Coronary Calcification The Multi-Ethnic Study of Atherosclerosis (MESA) Bild DE et al. Circulation. 2005;111:1313-1320. 6814 men and women aged 45-84 years

38
Five-Year Mortality Rates in Framingham Risk Subsets by Coronary Calcium Score Shaw et al. Radiology 2003; 228:826-833 * * * *p<0.001

39
MI in 41 pts during 3.2 + 0.7 years LDL levels similar in MI and non-MI pts Relative risk of MI in presence of CAC progression was 17.2-fold higher (P<0.0001) Progression of Coronary Artery Calcium and Risk of First MI 495 Asymptomatic Patients Started on Statin Therapy Raggi P et al. Arterioscler Thromb Vasc Biol. 2004;24:1272-77.

40
Coronary Disease Progression ? Role for CTA >60% stenosis (+) stress/imaging Calcified Plaque Detected by CT
 stress/imaging Calcified Plaque Detected by CT.")
41
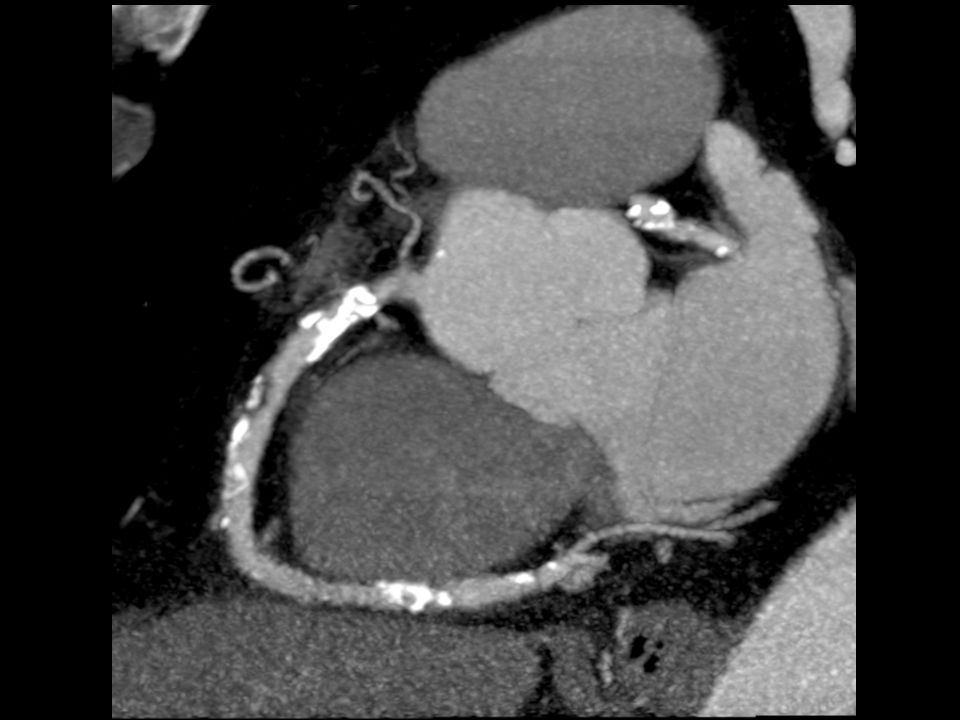
Soft Plaque Visualization

42
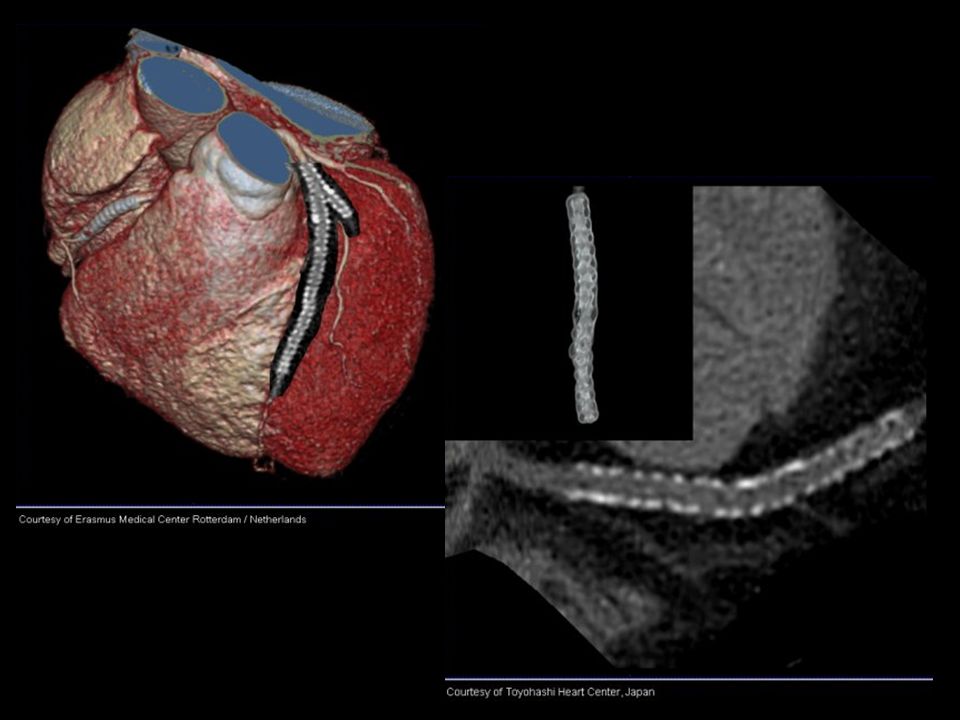
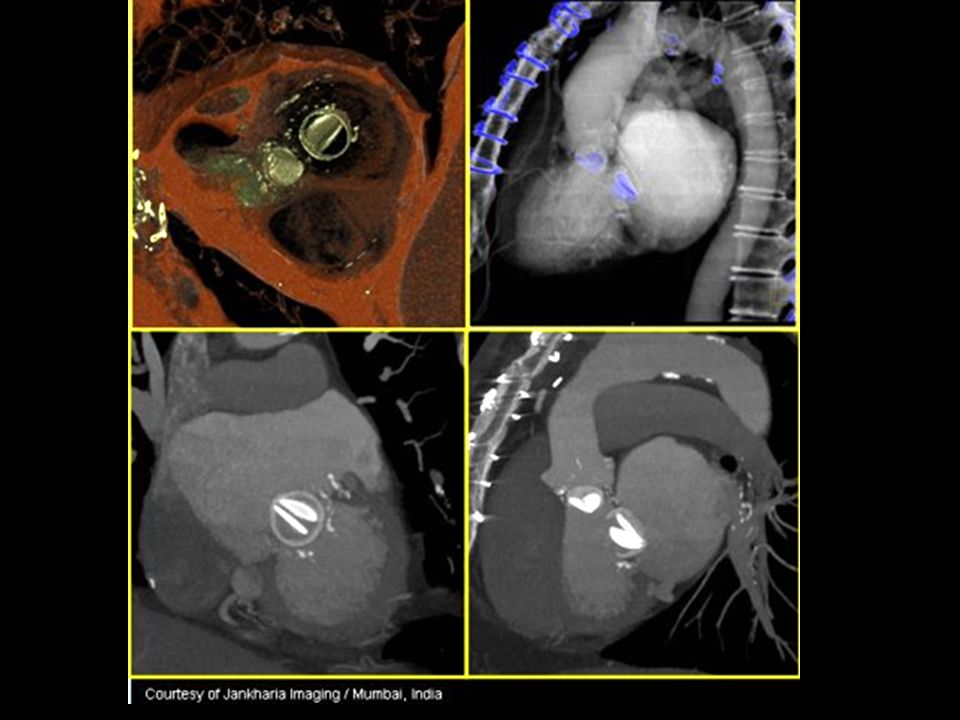
CTA Limitations Rapid (>80 bpm) and irregular HR High calcium scores (>800-1000) Stents Contrast requirements (Cr > 2.0 mg/dl) Small vessels (<1.5 mm) and collaterals Obese and uncooperative patients RADIATION EXPOSURE
 and irregular HR High calcium scores (> ) Stents Contrast requirements (Cr > 2.0 mg/dl) Small vessels (<1.5 mm) and collaterals Obese and uncooperative patients RADIATION EXPOSURE")
48
Effective Dose of Selected Radiologic Examinations PA/Lateral CXR 0.04-0.06 mSv Head CT 1-2 mSv Chest CT 5-7 mSv Abd/Pelvis CT 8-11 mSv Diagnostic Cor Angiogram 3-5 mSv MSCT angiography 9.3-11.3 mSv Morin et al. Circulation 2003;107:917-22. *Average annual background radiation in U.S ~ 3.6 mSv

49
Radiation Risks Exact quantification of harmful effects of radiation difficult to ascertain For a child under age 15, the risk of cancer death from a single CT scan is approximately 1 in 500 For a 45 year old adult, the risk of death from cancer from a single CT exam is about 1 in 1,250 Brenner et al. Radiology, 231(2):440-445.
:")
50
Clinical Indications for MSCT Calcium Scoring (CS) - risk stratification in the intermediate risk patient Non-invasive coronary angiography (CTA) in the symptomatic low-risk patient or asymptomatic intermediate- risk patient *A negative test (normal CTA) has a 98% chance of revealing normal coronary arteries on invasive angiography*
 - risk stratification in the intermediate risk patient Non-invasive coronary angiography (CTA) in the symptomatic low-risk patient or asymptomatic intermediate- risk patient *A negative test (normal CTA) has a 98% chance of revealing normal coronary arteries on invasive angiography*")
51
Test Selection According to Pretest Probability of CAD

52
Association for the Eradication of Heart Attacks (AEHA.org)
")
53
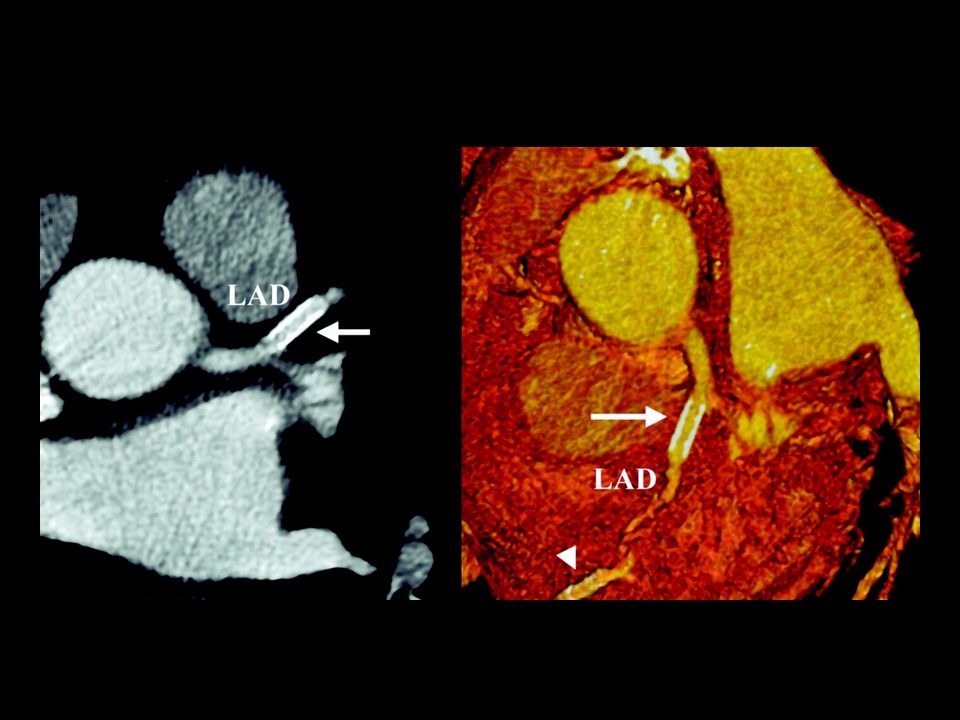
When to Consider MSCT Equivocal stress test or persistent symptoms despite negative stress test Prior to non-coronary cardiac surgery (valve or congenital repair) Patients with difficult access or on therapeutic warfarin Suspected coronary anomalies
 Patients with difficult access or on therapeutic warfarin Suspected coronary anomalies")
54
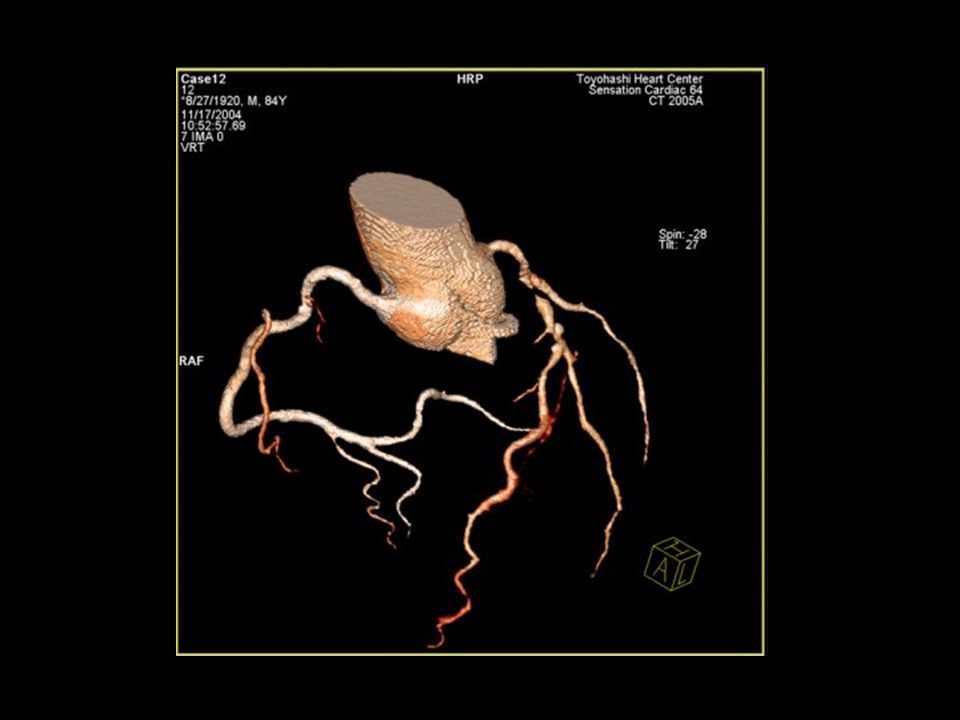
Lt Main CFX RCA LAD

55
Idiopathic dilated cardiomyopathy Cardiac transplant evaluation Patients to undergo electrophysiologic intervention (AF ablation, BiV pacing) Selected patients pre- and post-bypass surgery (aortic pathology, graft patency) When to Consider MSCT (continued)
 Selected patients pre- and post-bypass surgery (aortic pathology, graft patency) When to Consider MSCT (continued)")
56
Mikaelian BJ et al. Circulation. 2005;112:e35-e36.

57
Pulmonary Vein Stenosis Vasamreddy et al. Heart Rhythm (2004) 1, 78-81.
 1,")
59
Aortic Coarctation Visualized by 16-Row Detector MSCT Fröhlich, G et al. Circulation. 2005;112:e81.

60
Pericardial Calcification Multi-Slice CT Scanning Superior to MRI Hoffmann et al. Circulation 108 (7): 48e Figure IG1
: 48e Figure IG1.")
61
Nikolaou et al. Cardiology Clinics. 21;(2003):639-655. Future Indications
: Future Indications")
62
The Great Promise of MSCT The “Triple Rule-Out”

63
“an appropriate imaging study is one in which the expected incremental information together with clinical judgment exceed the expected negative consequences* by a sufficiently wide margin that the procedure is generally considered acceptable care and a reasonable approach for the indication.” Appropriateness Criteria * include risks of the procedure and the downstream impact of poor test performance such as delay in diagnosis (false -) or inappropriate diagnosis (false +)
 or inappropriate diagnosis (false +)")
Similar presentations




>")







 Dynamic scanning implies 15 or more scans in rapid sequence within one.>")






