Download presentation
Presentation is loading. Please wait.

1
GI Motility Part 1 L-8

2
Learning objectives Learning objectives Role of enteric nervous system (ENS) in gastrointestinal motility Role of enteric nervous system (ENS) in gastrointestinal motility Types of motility & their functions Types of motility & their functions Mastication Mastication Deglutition Deglutition Motor functions of the stomach (Gastric peristalsis, gastric emptying,) Motor functions of the stomach (Gastric peristalsis, gastric emptying,) The mechanism of vomiting- causes, consequences of protracted vomiting The mechanism of vomiting- causes, consequences of protracted vomiting
 in gastrointestinal motility Role of enteric nervous system (ENS) in gastrointestinal motility Types of motility & their functions Types of motility & their functions Mastication Mastication Deglutition Deglutition Motor functions of the stomach (Gastric peristalsis, gastric emptying,) Motor functions of the stomach (Gastric peristalsis, gastric emptying,) The mechanism of vomiting- causes, consequences of protracted vomiting The mechanism of vomiting- causes, consequences of protracted vomiting")
3
Learning outcomes Learning outcomes 8.1 Briefly describe the function of ENS in GI motility 8.1 Briefly describe the function of ENS in GI motility 8.2 Briefly describe the mechanism of deglutition 8.2 Briefly describe the mechanism of deglutition 8.3 Outline the basic physiologic mechanism preventing or minimizing gastro esophageal reflux 8.3 Outline the basic physiologic mechanism preventing or minimizing gastro esophageal reflux

4
Learning outcomes contd Learning outcomes contd 8.4 State the basic physiologic defect in Achalasia 8.4 State the basic physiologic defect in Achalasia 8.5 Briefly describe the motor functions of the stomach 8.5 Briefly describe the motor functions of the stomach 8.6 Briefly describe how gastric emptying is regulated ? 8.6 Briefly describe how gastric emptying is regulated ? 8.7 Briefly describe the basic physiologic mechanism of vomiting 8.7 Briefly describe the basic physiologic mechanism of vomiting

5
MASTCATION or Chewing MASTCATION or Chewing First mechanical process to which food is subjected in the mouth. It’s an voluntary act. First mechanical process to which food is subjected in the mouth. It’s an voluntary act. Muscles of mastication are: Muscles of mastication are: Masseter, internal and external pterygoids, temporal muscles and buccinator. Masseter, internal and external pterygoids, temporal muscles and buccinator. Movements of upper & lower jaw by these muscles bring about the apposition of two rows of teeth, which grinds or breaks the food. Tongue helps in rolling over the food. Movements of upper & lower jaw by these muscles bring about the apposition of two rows of teeth, which grinds or breaks the food. Tongue helps in rolling over the food.

6
Purpose served by mastication Purpose served by mastication -solid, large food particles are broken & reduced to a size convenient for swallowing. -solid, large food particles are broken & reduced to a size convenient for swallowing. - helps to break the indigestible cellulose covering in fruits & vegetables. - helps to break the indigestible cellulose covering in fruits & vegetables. - chewing results in reflex salivation - chewing results in reflex salivation

7
- serves to mix food with saliva, so as to moisten & lubricate & thereby facilitate act of swallowing. - serves to mix food with saliva, so as to moisten & lubricate & thereby facilitate act of swallowing. - Helps to mix with digestive components of saliva. - Helps to mix with digestive components of saliva. Physical act of chewing thus helps in taste, smell and appreciation of other sensory qualities of the food. Physical act of chewing thus helps in taste, smell and appreciation of other sensory qualities of the food. By mastication finally the bolus is formed. By mastication finally the bolus is formed.

8
DEGLUTITION DEGLUTITION It is the act of swallowing. The passage of bolus from the oesophagus to stomach. It is the act of swallowing. The passage of bolus from the oesophagus to stomach. Process is complicated since pharynx forms a common passage for both respiration & food passage. Process is complicated since pharynx forms a common passage for both respiration & food passage. Divided into 3 stages: Divided into 3 stages: 1. Oral Phase (voluntary) 1. Oral Phase (voluntary) 2. Pharyngeal phase (involuntary) 2. Pharyngeal phase (involuntary) 3. Oesophageal phase (involuntary) 3. Oesophageal phase (involuntary)
 1. Oral Phase (voluntary) 2. Pharyngeal phase (involuntary) 2. Pharyngeal phase (involuntary) 3. Oesophageal phase (involuntary) 3. Oesophageal phase (involuntary).")
9
Deglutiion (act of swallowing) Is a sequentially programmed reflex Initiated voluntarily Multiple responses triggered in a specific timed sequence Involves highly coordinated contraction of several muscles Swallowing center located in the medulla Receptors in the pharyngeal wall
 Is a sequentially programmed reflex Initiated voluntarily Multiple responses triggered in a specific timed sequence Involves highly coordinated contraction of several muscles Swallowing center located in the medulla Receptors in the pharyngeal wall")
10
Oral phase Oral phase When the bolus is ready for swallowing, it is voluntarily squeezed or rolled posteriorly into the pharynx by pressure of the tongue upwards & backwards against the hard palate. When the bolus is ready for swallowing, it is voluntarily squeezed or rolled posteriorly into the pharynx by pressure of the tongue upwards & backwards against the hard palate.

11
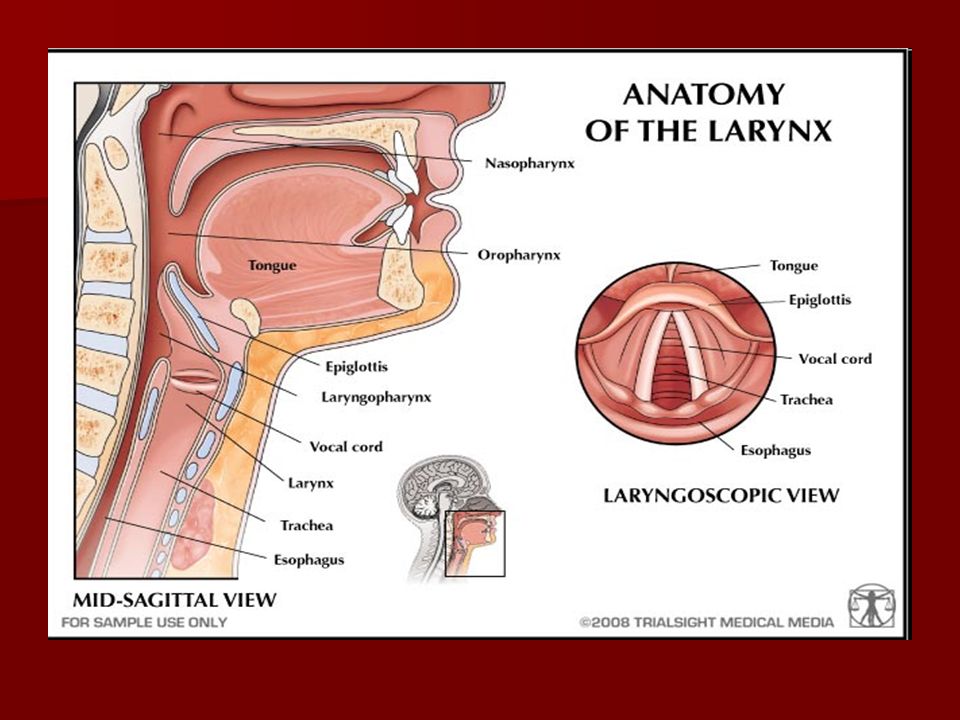
Pharyngeal phase Pharyngeal phase As bolus enters posterior aspect of oral cavity, around pharynx, receptors get stimulated & send impulses to medullary deglutition center, which initiates series of coordinated automatic pharyngeal muscle contractions. As bolus enters posterior aspect of oral cavity, around pharynx, receptors get stimulated & send impulses to medullary deglutition center, which initiates series of coordinated automatic pharyngeal muscle contractions. Now the bolus can enter into nasal cavities, trachea or oesophagus. So first two entries has to be blocked. Now the bolus can enter into nasal cavities, trachea or oesophagus. So first two entries has to be blocked. 1. soft palate is pulled upwards to close the posterior nares, which prevents reflux of food into nasal cavities. 1. soft palate is pulled upwards to close the posterior nares, which prevents reflux of food into nasal cavities.

12
2. Vocal cords of the larynx are strongly approximated, and larynx is pulled upwards & anterior by the neck muscles. 2. Vocal cords of the larynx are strongly approximated, and larynx is pulled upwards & anterior by the neck muscles. These actions cause the epiglottis to swing backwards over the opening of larynx, which prevents entry of food into trachea. These actions cause the epiglottis to swing backwards over the opening of larynx, which prevents entry of food into trachea.

14
3. Palatopharyngeal folds pulled medially to approximate each other. These folds form a saggital slit through which food passes, this selectively allows only properly masticated food. 3. Palatopharyngeal folds pulled medially to approximate each other. These folds form a saggital slit through which food passes, this selectively allows only properly masticated food. What is deglutition apnoea ? What is deglutition apnoea ?

15
4. Upward movement of larynx also pulls up & enlarges the opening of the esophagus. At the same time pharyngoesophageal sphincter relaxes, thus allowing bolus to move freely into oesophagus from pharynx. 4. Upward movement of larynx also pulls up & enlarges the opening of the esophagus. At the same time pharyngoesophageal sphincter relaxes, thus allowing bolus to move freely into oesophagus from pharynx. 5. Peristalsis starts in superior part of the pharynx then spreads over downward. 5. Peristalsis starts in superior part of the pharynx then spreads over downward.

16
Pharyngeal phase Tongue pressed against hard palate Uvula elevated, touches posterior pharyngeal wall Elevation of larynx Epiglottis swings backwards Closure of vocal folds Food prevented from re-entering mouth Food prevented from re-entering mouth Seals off nasal passage Seals off nasal passage Food prevented from re-entering respiratory passage Food prevented from re-entering respiratory passage

17
1 2 5 3 4 Tongue Uvula Bolus Epiglottis Laryngeal opening Esophagus

18
Deglutition reflex Receptors: Pressure receptors on the pharyngeal wall, especially on the tonsillar pillars Receptors: Pressure receptors on the pharyngeal wall, especially on the tonsillar pillars Afferents: V, IX, X nerves Afferents: V, IX, X nerves Center: Medulla oblongata (deglutition Center: Medulla oblongata (deglutition centre) centre) Efferents: V, IX, X, XII nerves Efferents: V, IX, X, XII nerves Effectors: Muscles of tongue, pharynx, Effectors: Muscles of tongue, pharynx, larynx larynx
 centre) Efferents: V, IX, X, XII nerves Efferents: V, IX, X, XII nerves Effectors: Muscles of tongue, pharynx, Effectors: Muscles of tongue, pharynx, larynx larynx")
19
Define Pristalisis Define Pristalisis constriction behind the bolus and relaxation appears in front of the bolus which results in forward movement of bolus (oral to aboral direction). constriction behind the bolus and relaxation appears in front of the bolus which results in forward movement of bolus (oral to aboral direction).
..")
20
Peristalsis constriction relaxation

21
Peristalsis Peristalsis Stimulus: Stretch of the gut wall Stimulus: Stretch of the gut wall Speed: variable 2-25cm /min Speed: variable 2-25cm /min Regulation: enteric NS (myentric plexus) is must, modulated by extrinsic nerves i.e sympathetic inhibits & parasympathetic stimulates. Can be blocked by atropine. Regulation: enteric NS (myentric plexus) is must, modulated by extrinsic nerves i.e sympathetic inhibits & parasympathetic stimulates. Can be blocked by atropine. Function: propulsion of chyme from oral to aboral direction. Function: propulsion of chyme from oral to aboral direction.
 is must, modulated by extrinsic nerves i.e sympathetic inhibits & parasympathetic stimulates. Can be blocked by atropine. Function: propulsion of chyme from oral to aboral direction. Function: propulsion of chyme from oral to aboral direction..")
22
Oesophageal stage Oesophageal stage Exhibits primary peristalsis, mostly continuation from pharynx, which passes all the way to stomach. Exhibits primary peristalsis, mostly continuation from pharynx, which passes all the way to stomach. If it fails reaching stomach, sec peristalisis starts from distended portion of oesophagus where food is retained. If it fails reaching stomach, sec peristalisis starts from distended portion of oesophagus where food is retained. Receptive relaxation of lower oesophageal sphincter(normally under tonic contraction with intramural pressure of 30 mm Hg) occurs ahead of the peristalitic wave, allows food to enter stomach. Receptive relaxation of lower oesophageal sphincter(normally under tonic contraction with intramural pressure of 30 mm Hg) occurs ahead of the peristalitic wave, allows food to enter stomach. Receptive relaxation of stomach also occurs. Receptive relaxation of stomach also occurs.
 occurs ahead of the peristalitic wave, allows food to enter stomach. Receptive relaxation of lower oesophageal sphincter(normally under tonic contraction with intramural pressure of 30 mm Hg) occurs ahead of the peristalitic wave, allows food to enter stomach. Receptive relaxation of stomach also occurs. Receptive relaxation of stomach also occurs..")
23
Applied aspects Applied aspects Gastro esophageal reflux disease (GERD) Gastro esophageal reflux disease (GERD) Frequent reflux of gastric contents into esophagus, due to incompetence of LES (sphincter not having tone). Symptom is heart burn, & this is the commonest cause of unexplained chest pain. Achalasia LES fails in receptive relaxation, so bolus gets held up in esophagus. Dysphagia Difficulty in swallowing. Esophageal muscles contract in a uncoordinated manner, may be due to neural disorders.

24
MOTILITY IN STOMACH MOTILITY IN STOMACH For purpose of describing movements stomach is visualized to be consisting of 2 parts- Orad (fundus & body), Caudad (lower part) For purpose of describing movements stomach is visualized to be consisting of 2 parts- Orad (fundus & body), Caudad (lower part) 1. Receptive relaxation 1. Receptive relaxation 2. Mixing & churning 2. Mixing & churning 3. Gastric emptying 3. Gastric emptying All these observed when stomach is full. All these observed when stomach is full.

25
Receptive relaxation Receptive relaxation To receive bolus orad part of stomach relaxes. Due to vagally mediated reflex when the bolus reaches LES. To receive bolus orad part of stomach relaxes. Due to vagally mediated reflex when the bolus reaches LES. Advantages of relaxation: Advantages of relaxation: As digestive processes are slow, stomach can act as reservoir, gets sufficient time for digestive juices to act. As digestive processes are slow, stomach can act as reservoir, gets sufficient time for digestive juices to act. Intragastric pressure doesn’t rise much ( if increases gastroesophageal reflux will occur). Intragastric pressure doesn’t rise much ( if increases gastroesophageal reflux will occur).
. Intragastric pressure doesn’t rise much ( if increases gastroesophageal reflux will occur)..")
26
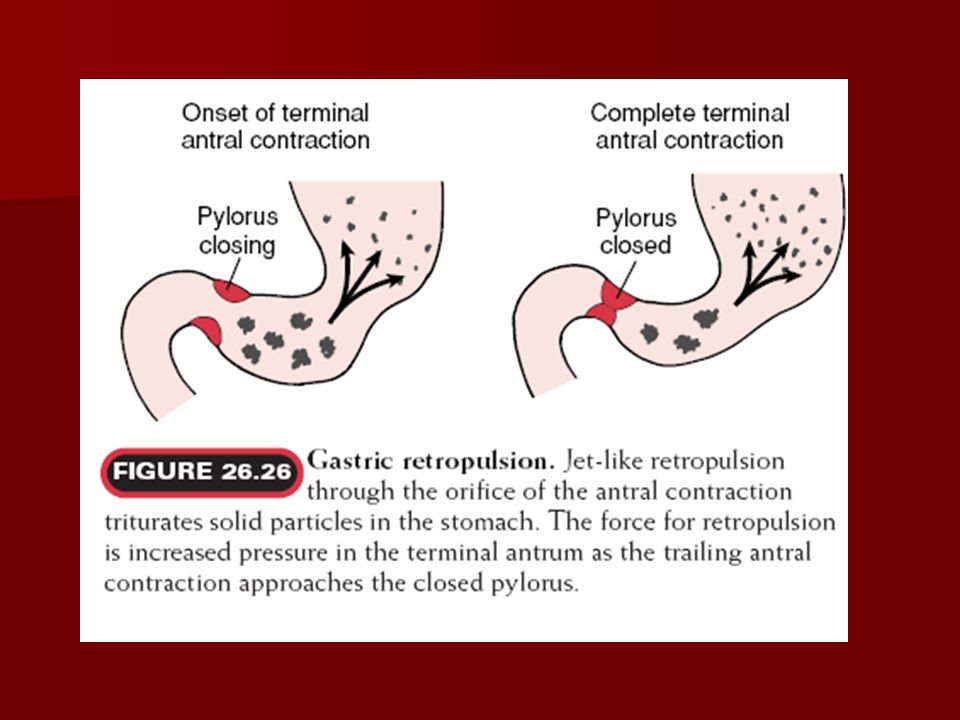
2. Mixing & churning 2. Mixing & churning These movements achieved by gastric peristalisis ( at a rate of 3/min) + closure of the pyloric sphincter. These movements achieved by gastric peristalisis ( at a rate of 3/min) + closure of the pyloric sphincter. Effects of these movements are- Effects of these movements are- Breaking down of coarse food chunks Breaking down of coarse food chunks Thorough mixing of gastric juice with food Thorough mixing of gastric juice with food Squirting of gastric chyme into duodenum (ejecting of small volume of chyme in thin spurt) Squirting of gastric chyme into duodenum (ejecting of small volume of chyme in thin spurt)
 + closure of the pyloric sphincter. These movements achieved by gastric peristalisis ( at a rate of 3/min) + closure of the pyloric sphincter. Effects of these movements are- Effects of these movements are- Breaking down of coarse food chunks Breaking down of coarse food chunks Thorough mixing of gastric juice with food Thorough mixing of gastric juice with food Squirting of gastric chyme into duodenum (ejecting of small volume of chyme in thin spurt) Squirting of gastric chyme into duodenum (ejecting of small volume of chyme in thin spurt).")
28
3.Gastric emptying 3.Gastric emptying Emptying occurs due to above explained mechanisms (gastric peristalsis with partially closed pyloric sphincter) Emptying occurs due to above explained mechanisms (gastric peristalsis with partially closed pyloric sphincter) Factors regulating gastric emptying- Neural- symp closes pyloric sphincter Factors regulating gastric emptying- Neural- symp closes pyloric sphincter VIP relaxes sphincter. VIP relaxes sphincter. Hormones & nature of chyme: Hormones & nature of chyme: Secretin, CCK, GIP, Gastrin, products of fat, protein digestion, highly acidic pH & hypertonicity of duodenal contents, distension of duodenum etc - delays gastric emptying ( Enterogastric reflex- if reflex is aroused from intestine ) Secretin, CCK, GIP, Gastrin, products of fat, protein digestion, highly acidic pH & hypertonicity of duodenal contents, distension of duodenum etc - delays gastric emptying ( Enterogastric reflex- if reflex is aroused from intestine )
 Secretin, CCK, GIP, Gastrin, products of fat, protein digestion, highly acidic pH & hypertonicity of duodenal contents, distension of duodenum etc - delays gastric emptying ( Enterogastric reflex- if reflex is aroused from intestine ).")
29
Enterogastric reflex: inhibitory reflex arising from duodenum which prevents gastric emptying Enterogastric reflex: inhibitory reflex arising from duodenum which prevents gastric emptying 1. Degree of distension of duodenum 1. Degree of distension of duodenum 2. Degree of irritation of duodenum 2. Degree of irritation of duodenum 3. Degree of acidity of duodenum 3. Degree of acidity of duodenum (pH<3.5) (pH<3.5) 4. degree of osmolarity of chyme 4. degree of osmolarity of chyme 5. Breakdown products of 5. Breakdown products of chyme especially protein, next fat. chyme especially protein, next fat.
 (pH<3.5) 4. degree of osmolarity of chyme 4. degree of osmolarity of chyme 5. Breakdown products of 5. Breakdown products of chyme especially protein, next fat. chyme especially protein, next fat..")
30
Gastric motility disorders: delayed gastric emptying (gastroparesis), rapid gastric emptying (dumping syndrome. Gastric motility disorders: delayed gastric emptying (gastroparesis), rapid gastric emptying (dumping syndrome. Reasons of abnormally delayed gastric emptying: Reasons of abnormally delayed gastric emptying: 1) Pylorus and duodenum may be obstructed by an ulcer or tumor, or by something large and indigestible that was swallowed. 1) Pylorus and duodenum may be obstructed by an ulcer or tumor, or by something large and indigestible that was swallowed. (2) The pyloric sphincter at the exit of the stomach may not open enough or at the right times to allow food to pass through. These reflexes depend on nerves that sometimes become damaged. (2) The pyloric sphincter at the exit of the stomach may not open enough or at the right times to allow food to pass through. These reflexes depend on nerves that sometimes become damaged. (3) The normally rhythmic, 3/min contractions of the lower part of the stomach can become disorganized so that the contents of the stomach are not pushed towards the pyloric sphincter (3) The normally rhythmic, 3/min contractions of the lower part of the stomach can become disorganized so that the contents of the stomach are not pushed towards the pyloric sphincter
, rapid gastric emptying (dumping syndrome. Reasons of abnormally delayed gastric emptying: Reasons of abnormally delayed gastric emptying: 1) Pylorus and duodenum may be obstructed by an ulcer or tumor, or by something large and indigestible that was swallowed. 1) Pylorus and duodenum may be obstructed by an ulcer or tumor, or by something large and indigestible that was swallowed. (2) The pyloric sphincter at the exit of the stomach may not open enough or at the right times to allow food to pass through. These reflexes depend on nerves that sometimes become damaged. (2) The pyloric sphincter at the exit of the stomach may not open enough or at the right times to allow food to pass through. These reflexes depend on nerves that sometimes become damaged. (3) The normally rhythmic, 3/min contractions of the lower part of the stomach can become disorganized so that the contents of the stomach are not pushed towards the pyloric sphincter (3) The normally rhythmic, 3/min contractions of the lower part of the stomach can become disorganized so that the contents of the stomach are not pushed towards the pyloric sphincter.")
32
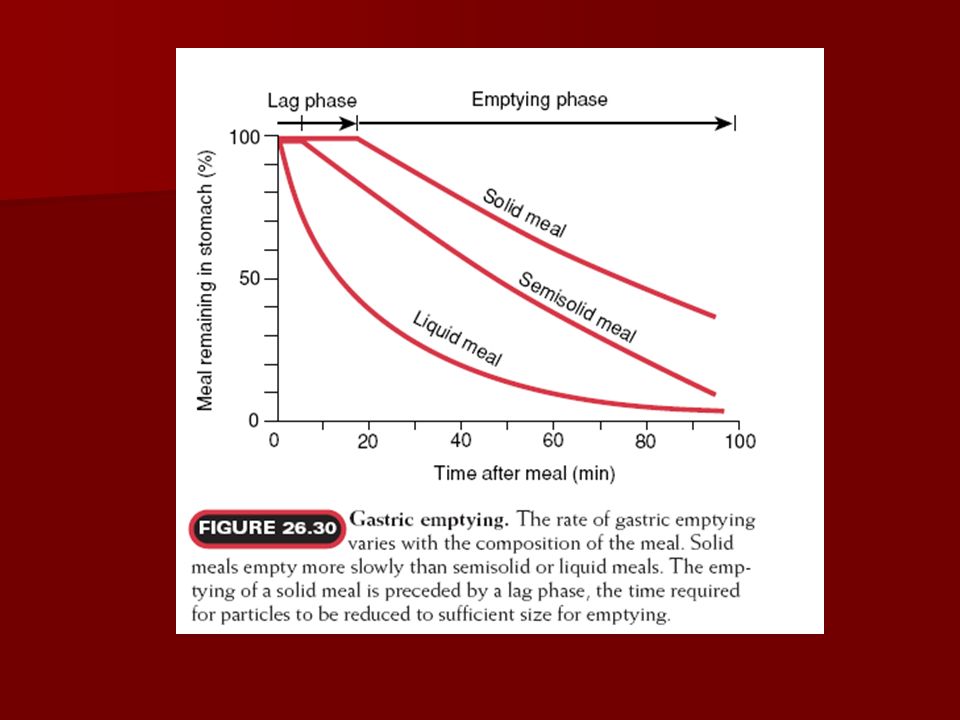
Rate of emptying stomach into duodenum based on the type of food

33
Gastric peristalisis in empty stomach (Migrating myoelectric complex MMC) Gastric peristalisis in empty stomach (Migrating myoelectric complex MMC) Empty stomach remains quiescent for 75-90 mins, after this a MMC develops. Empty stomach remains quiescent for 75-90 mins, after this a MMC develops. MMC is a wave of depolarization which is immediately followed by an wave of muscular contraction (hunger contractions). MMC is a wave of depolarization which is immediately followed by an wave of muscular contraction (hunger contractions). MMC sweeps the whole stomach, then travels duodenum, rest part of intestine, terminates at terminal part of ileum taking about 10 mins. MMC sweeps the whole stomach, then travels duodenum, rest part of intestine, terminates at terminal part of ileum taking about 10 mins. Again stomach rests for 75-90 mins then the MMC repeats. Again stomach rests for 75-90 mins then the MMC repeats.
. MMC is a wave of depolarization which is immediately followed by an wave of muscular contraction (hunger contractions). MMC sweeps the whole stomach, then travels duodenum, rest part of intestine, terminates at terminal part of ileum taking about 10 mins. MMC sweeps the whole stomach, then travels duodenum, rest part of intestine, terminates at terminal part of ileum taking about 10 mins. Again stomach rests for mins then the MMC repeats. Again stomach rests for mins then the MMC repeats..")
34
Functions of MMC Functions of MMC Drives out remnants of food in stomach Drives out remnants of food in stomach Jejunal & ileal content are mostly bacteria free, however some bacteria which would have entered from colon to ileum, has to be driven back to the colon otherwise leads to diarrhea, malabsorption Jejunal & ileal content are mostly bacteria free, however some bacteria which would have entered from colon to ileum, has to be driven back to the colon otherwise leads to diarrhea, malabsorption Helps in driving out bacteria into colon. Helps in driving out bacteria into colon.

35
Vomiting (emesis) Oral expulsion of upper GI contents resulting from contractions of the gut and muscles of the thorax and abdomen. Oral expulsion of upper GI contents resulting from contractions of the gut and muscles of the thorax and abdomen. Retrograde or reverse peristalsis Retrograde or reverse peristalsis

36
Causes of vomiting & mechanism Causes of vomiting & mechanism Poison ingestion (by irritation) Poison ingestion (by irritation) Increased intracranial tension (symptom of a disease) Increased intracranial tension (symptom of a disease) Uremia ( effects on chemoreceptor trigger zone in medulla) Uremia ( effects on chemoreceptor trigger zone in medulla) Impairment of gastric motility( increase intragastric pressure). Impairment of gastric motility( increase intragastric pressure).
..")
37
Mechanism of vomiting in intestinal obstruction: Mechanism of vomiting in intestinal obstruction: Aff input to vomiting center in medulla, reflexly sends efferent impulses to abdominal muscles & diaphragm Aff input to vomiting center in medulla, reflexly sends efferent impulses to abdominal muscles & diaphragm Retrograde peristalsis in stomach Retrograde peristalsis in stomach Intragastric pressure increases Intragastric pressure increases LES relaxes & vomitus ejected via esophagus (closure of glottis prevents aspiration of vomitus) LES relaxes & vomitus ejected via esophagus (closure of glottis prevents aspiration of vomitus)
 LES relaxes & vomitus ejected via esophagus (closure of glottis prevents aspiration of vomitus)")
38
Consequences of Protracted vomiting: Consequences of Protracted vomiting: Dehydration due to loss of GI secretions Dehydration due to loss of GI secretions Loss of hydrogen ions leads metabolic alkalosis Loss of hydrogen ions leads metabolic alkalosis Prolonged vomiting leads to malnutrition Prolonged vomiting leads to malnutrition Loss of chloride ions ( hypochloremia) Loss of chloride ions ( hypochloremia)
 Loss of chloride ions ( hypochloremia)")
Similar presentations





 Salivary Secretion>")
>")




 Ass. Prof. Dr. Emre Hamurtekin EMU Faculty of Pharmacy.>")







