Download presentation
Presentation is loading. Please wait.

1
Metal Allergies in Arthroplasty Michael Zlowodzki MD University of Minnesota Department of Orthopaedic Surgery

2
OUTLINE Incidence of metal hypersensitivity: Are all metals the same? Types of hypersensitivity Does metal sensitivity contribute to implant failure or affect patient function? Methods to test for metal sensitivity

3
20 y/o female Extensive eczematous dermatitis on chest and back 5 months after fixation of a patella fracture with a stainless steel screw Treated with topical steroids for 1 year “Out of sheer desperation” the screw was removed 72h after screw removal the eczema completely disappeared CASE EXAMPLE

4
“The orthopaedist still doubted that the steel screws could be the cause of her dermatitis and applied a stainless steel screw to the skin of her back. In a period of 4 hours generalized pruritus and erythema developed.”

5
INCIDENCE: Dermal hypersensitivity to metal: 10-15%

6
Why are metals causing hypersensitivity? All metals in contact with biological systems corrode Released ions form complexes with proteins, which act as antigens (allergens) Hypersensitivity Response
 Hypersensitivity Response.")
8
Types of Hypersensitivity Humeral response –Type 1, 2, 3 –Within minutes Cell-mediated response –Type 4 –Within hours to days –Main response in implant-related hypersensitivity

9
Cell-mediated response (Type 4) Antigens activate T-lymphocytes T-Lymphocytes release cytokines –Interferon –Tumor necrosis factor –Interleukin 1&2 Cytokines recruit and activate macrophages, monocytes and neutrophils
 Antigens activate T-lymphocytes T-Lymphocytes release cytokines –Interferon –Tumor necrosis factor –Interleukin 1&2 Cytokines recruit and activate macrophages, monocytes and neutrophils")
10
Local Reaction Metallosis Excessive periprosthetic fibrosis Muscular necrosis Implant loosening???

11
What cause the actual tissue damage?

12
Vicious Cycle Macrophages trigger activation of T-cells T-cells activate macrophages Macrophages trigger activation of T-cells T-cells activate macrophages

13
What can happen? Hives Eczema Erythema Pruritus Dermatitis Urticaria Vasculitis

14
Size of particles is important Large particles may not bond to proteins and may not act as antigens

15
Metal-on-Metal Arthroplasty Cobalt ions Chromium ions Charged Bind with proteins Act as antigens Particle size in nanometer range (< 50 nm)
")
16
N=8 with >20y McKee-Farrar THA 9-fold elevation of serum chromium 35-fold elevation of urine chromium 3-fold elevation of serum cobalt N=6 with <2y McKee-Farrar THA 3-fold elevation of serum chromium 4-fold elevation of serum cobalt

17
Metals known as sensitizers Nickel Cobalt Chrome Beryllium Titanium Tantellum Vanadium

18
Cross-reactivity between nickel and cobalt Titanium implants instead of stainless steel in patients allergic to Nickel Zirconium alloy least allergenic

19
“OXINIUM implants also increase the opportunity for patients with an acute allergy to nickel to have knee replacement surgery. Although many metals have traces of nickel in them, this advanced material does not have any detectable amount of nickel.”

20
Stainless steel: –Chromium –Nickel –Molybdenium Titanium –Titanium –Aluminum –Vanadium

21
TESTING FOR HYPERSENSITIVITY

22
In-Vivo vs. In-Vitro In-Vivo: –Skin testing In-Vitro: –Lymphocyte transformation testing (LTT) –Leukocyte migration inhibition testing (LIF / MIF)
 –Leukocyte migration inhibition testing (LIF / MIF).")
23
In-Vivo: Skin testing Skin testing may be not applicable for implant related testing –Exposure too short –Hypersensitivity response not to implant itself, but the dissolution or corrosion products –it is unclear which are the optimal challenge agents (eg, metal chlorides, specific metal-protein complexes). –the skin possesses unique antigen-presenting cells (Langerhans cells) that are not present in the periprosthetic tissues –Could induce hypersensitivity Not useful
 that are not present in the periprosthetic tissues –Could induce hypersensitivity Not useful.")
24
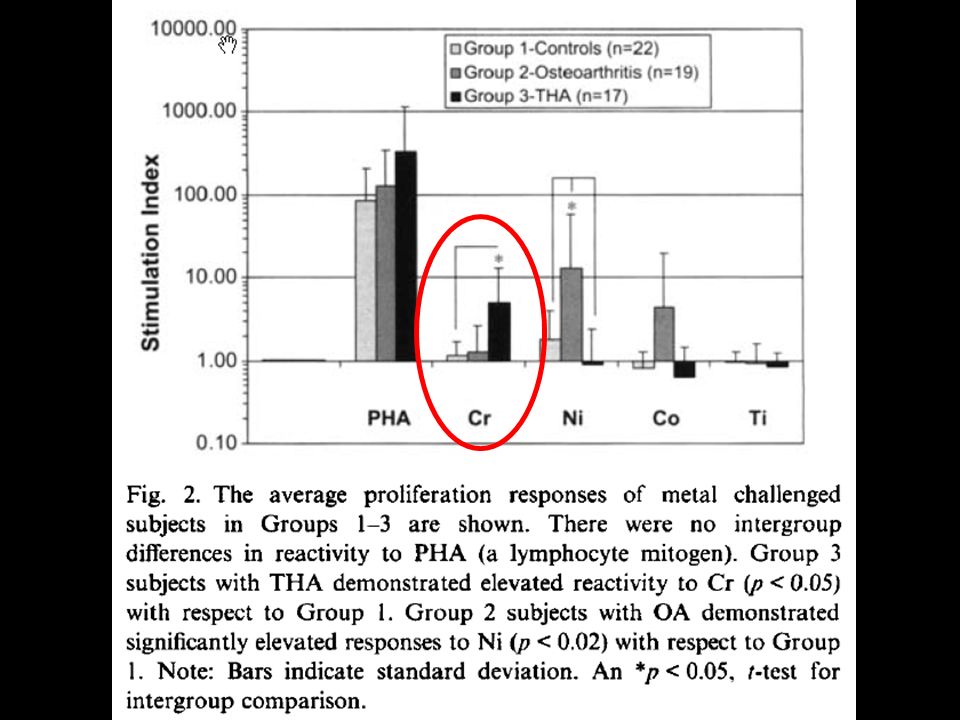
In-Vitro testing: Lymphocyte transformation testing (LTT) Developed in 1960 Measures proliferative response of lymphocytes to antigens Lymphocytes which are sensitized by allergens transform into blasts and proliferate when they are again exposed to the antigen DNA replication is used as a measure of proliferation Ratio of lymphocyte proliferation after antigen challenge to lymphocyte proliferation in the absence of antigen. This ratio is called the stimulation index (SI)
.")
25
Lymphocyte transformation testing (LTT): How does it work? Patients blood (Lymphocytes) A mitogen that transforms lymphycytes into lymphoblasts (PHA) Antigen (Metal of choice) Radioactive DNA marker (Radiolabeled Thymidine)
 A mitogen that transforms lymphycytes into lymphoblasts (PHA) Antigen (Metal of choice) Radioactive DNA marker (Radiolabeled Thymidine).")
26
Lymphocyte transformation testing (LTT): How does it work? Radioactive marker gets incorporated into lymphocytes and is measured after 6 days Not available at VA

27
Advantages of LTT Quantifiable number Greater sensitivity Blood instead of skin contact Does not induce hypersensitivity Can test for many metals in several concentrations

28
Disadvantages of LTT the optimal challenge agent has yet to be established Threshold values unknown False-positives Clinical significance unclear

31
Positive LTT and osteolysis

32
In-Vitro testing: Leukocyte migration inhibition testing (LIF / MIF) Leukocytes in culture migrate randomly Can be attracted by chemoattractants such as those related by bacteria In the presence of sensitizing antigents leukocytes move more slowly -> they are “migration-inhibited” Labor intensive and inaccurate
 Leukocytes in culture migrate randomly Can be attracted by chemoattractants such as those related by bacteria In the presence of sensitizing antigents leukocytes move more slowly -> they are migration-inhibited Labor intensive and inaccurate")
33
Does metal sensitivity affect patient function and failure rates?

34
25% vs. 60%

35
Does metal sensitivity cause aseptic loosening?

36
Positive patch testing results Metal-on-Metal: 28% (Total N=32) Metal-on-Poly: 3% (Total N=29) Controls: 3% (Total N=33) 2/9 aseptic loosenings in metal-on-metal group with positive patch test
 Metal-on-Poly: 3% (Total N=29) Controls: 3% (Total N=33) 2/9 aseptic loosenings in metal-on-metal group with positive patch test")
37
Metal-on-metal: Histologic response Prominent perivascular and/or diffuse lymphocytic infiltration that is reminiscent of a delayed-type hypersensitivity response Willert HG et al: Metal-on-metal bearings and hypersensitivity in patients with artificial hip joints: A clinical and histomorphological study. J Bone Joint Surg Am 2005;87:28-36.

38
Aseptic lymphocytedominated vasculitis- associated lesion (ALVAL)
")
39
CONCLUSION Risk of using metal implants is minimal Contribution to implant failure unknown Clinical value of in-vitro testing (LTT) unknown Use Titanium or Zirconium implants instead of stainless steel in patients allergic to Nickel
 unknown Use Titanium or Zirconium implants instead of stainless steel in patients allergic to Nickel")
Similar presentations






 Immune team. Cell-Mediated Immunity (CMI) Antigen T-lymphocytes Immune responses Immune responses.>")

 Immune system.>")


 Or to precipitate.>")


 Prof. Dr. Zahid Shakoor MBBS, Ph D (London) College of Medicine King Saud University.>")





