Download presentation
Presentation is loading. Please wait.

1
TMF Quality Innovation Network Quality Improvement Organization Coordination of Care and Medication Safety Project August 18, 2015

2
About TMF QIN TMF Health Quality Institute focuses on improving lives by improving the quality of health care through contracts with federal, state and local governments, as well as private organizations. For nearly 40 years, TMF has helped health care providers and practitioners in a variety of settings improve care for their patients. We provide quality improvement services in these states: Arkansas, Missouri, Oklahoma, Puerto Rico and Texas.

3
About the QIN-QIO Program Leading rapid, large-scale change in health quality: Goals are bolder. The patient is at the center. All improvers are welcome. Everyone teaches and learns. Greater value is fostered. 3

4
Major Changes to the CMS Quality Improvement Organization Program The Centers for Medicare & Medicaid Services (CMS) separated medical case review from quality improvement work creating two separate structures: › Medical case review to be performed by Beneficiary Family Centered Care Quality Improvement Organizations (BFCC-QIOs) › Quality improvement and technical assistance QIOs to be performed by Quality Innovation Network Quality Improvement Organizations (QIN- QIOs) › Note: Both types of contracts cannot be held by the same organization BFCC-QIOs are organized among five geographic areas across the Nation. QIN-QIOs are regional and cover up to six states and/or territories. The QIO contract cycle will be extended from 3 to 5 years.

5
TMF QIN-QIO Regional Partners TMF has built a strong quality improvement team throughout the multi- state region, partnering with longtime, successful quality improvement entities, Arkansas Foundation for Medical Care (AFMC), Primaris in Missouri and the Quality Improvement Professional Research Organization, Puerto Rico (QIPRO) to form the TMF QIN-QIO.
, Primaris in Missouri and the Quality Improvement Professional Research Organization, Puerto Rico (QIPRO) to form the TMF QIN-QIO.")
6
11SOW QIN-QIO Map

7
TMF QIN-QIO’s Provide technical assistance with: Community coalition formation Root cause analyses Intervention selection and implementation plan Measurement Provide readmission and medication safety metrics Provide educational webinars

8
The QIO Program’s Approach to Clinical Quality Foundational Principles: Enable innovation Foster learning organizations Eliminate disparities Strengthen infrastructure and data systems Goals Make care safer Strengthen person and family engagement Promote effective communication and coordination of care Promote effective prevention and treatment Promote best practices for healthy living Make care affordable

9
TMF QIN-QIO Learning and Action Network: http://www.TMFQIN.orghttp://www.TMFQIN.org 9

10
TMF QIN-QIO Learning and Action Network: http://www.TMFQIN.orghttp://www.TMFQIN.org 10

11
Readmissions Network Reduce hospital readmission rates in the Medicare program by 20 percent Reduce hospital admission rates in the Medicare program by 20 percent Increase community tenure by increasing the number of days spent at home by Medicare Fee-for-Service (FFS) beneficiaries by 10 percent Reduce the prevalence of adverse drug events, emergency department visits and observation stays or readmissions occurring as a result of the care transitions process 11
 beneficiaries by 10 percent Reduce the prevalence of adverse drug events, emergency department visits and observation stays or readmissions occurring as a result of the care transitions process 11")
12
Medication Safety Network Reduce ADEs by 35 percent per 1,000 screened Medicare Fee-for-Service (FFS) beneficiaries by the year 2019 Monitor ADE rates by Medicare FFS beneficiaries on anticoagulants, diabetic agents or opioids by care setting, state, region and readmission rate 12
 beneficiaries by the year 2019 Monitor ADE rates by Medicare FFS beneficiaries on anticoagulants, diabetic agents or opioids by care setting, state, region and readmission rate 12")
13
Behavioral Health Network Increase screening for depression and alcohol use disorder in primary care Improve post-discharge follow-up care for patients hospitalized in Inpatient Psychiatric Facilities Reduce readmissions following hospitalization in Inpatient Psychiatric Facilities

14
Source: Lynn J, Straube BM, Bell KM, Jencks SF, Kambic RT. Using population segmentation to provide better health care for all: The “Bridges to Health” model. Milbank Q. 2007;85:185-208. Statement of Problem: Readmissions Hospitalizations consume 31 percent of the $2 trillion in total health care expenditures in the United States › 1 in 4 (25 percent) of hospitalizations are avoidable › 1 in 5 (20 percent) of all hospitalizations result in 30-day readmissions 14
 of hospitalizations are avoidable › 1 in 5 (20 percent) of all hospitalizations result in 30-day readmissions 14.")
15
Why are people readmitted? No Community infrastructure for achieving common goals Unreliable system support Lack of standard and known processes Unreliable information transfer Unsupported patient activation during transfers Provider-Patient interface U nmanaged condition worsening Use of suboptimal medication regimens Return to an emergency department 15

18
Top Five MS DRGs and their 30-day Inpatient Readmission Rates: Texas 11/1/2014 – 1/31/2015 DRG CodeDRG Description Number of Discharges 30-day Readmits Rate of 30- day Readmits 871 Septicemia or severe sepsis w/o mv 96+ hours w/ mcc 7,6161,24316.3% 291 Heart failure and shock w/ mcc 3,67283922.8% 292 Heart failure & shock w/ cc 3,38072921.6% 193 Simple pneumonia & pleurisy w/ mcc 3,21555817.4% 190 Chronic obstructive pulmonary disease w/ mcc 2,84954019.0% Source: Medicare Part A Claims Data 18

19
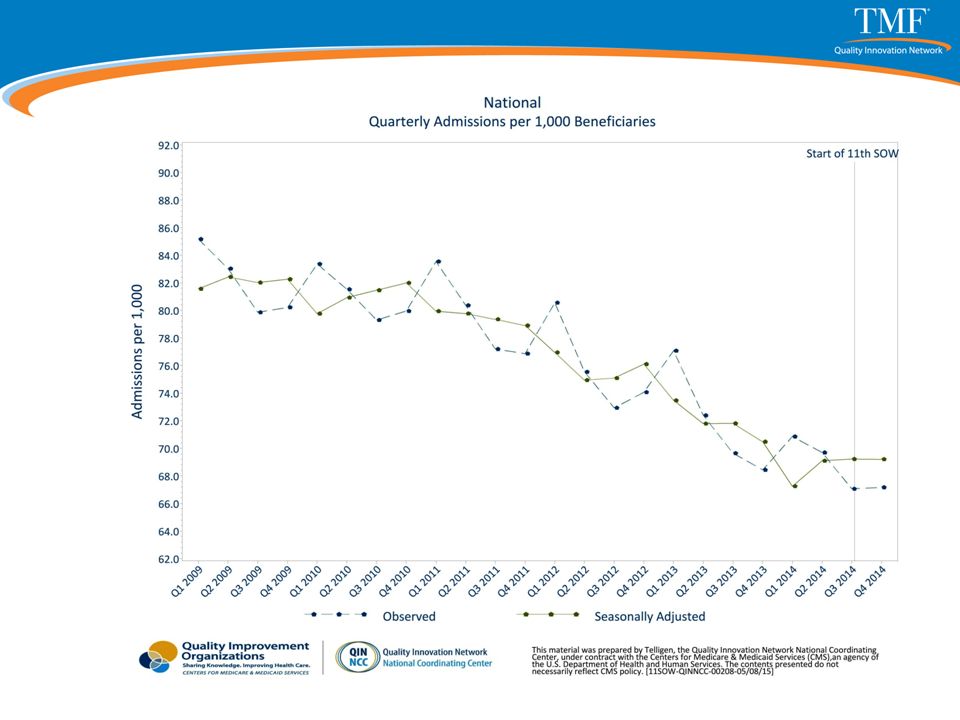
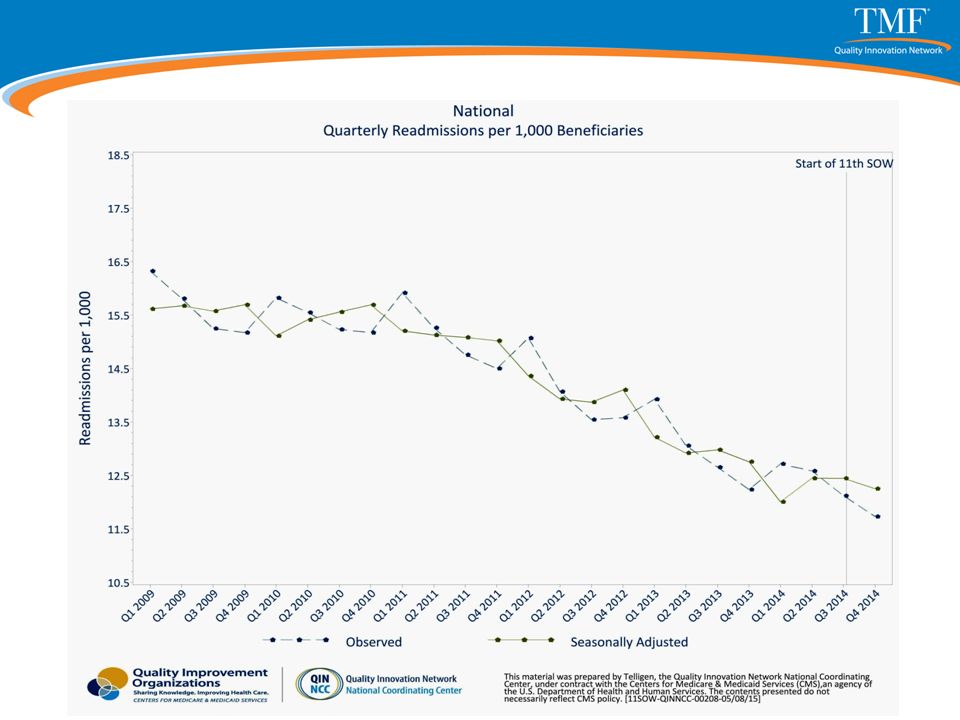
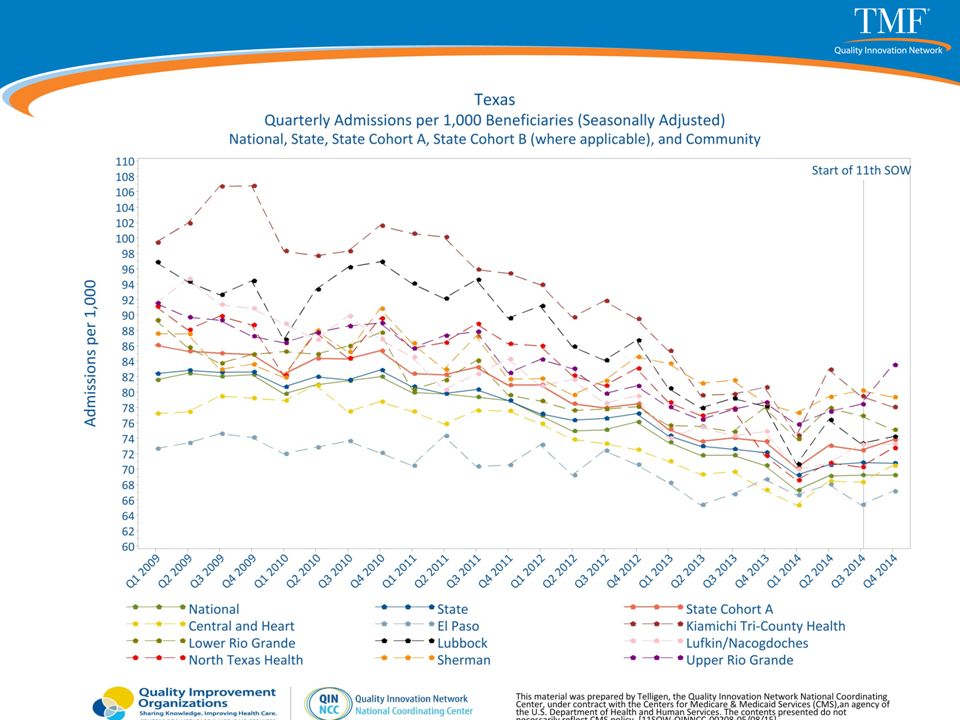
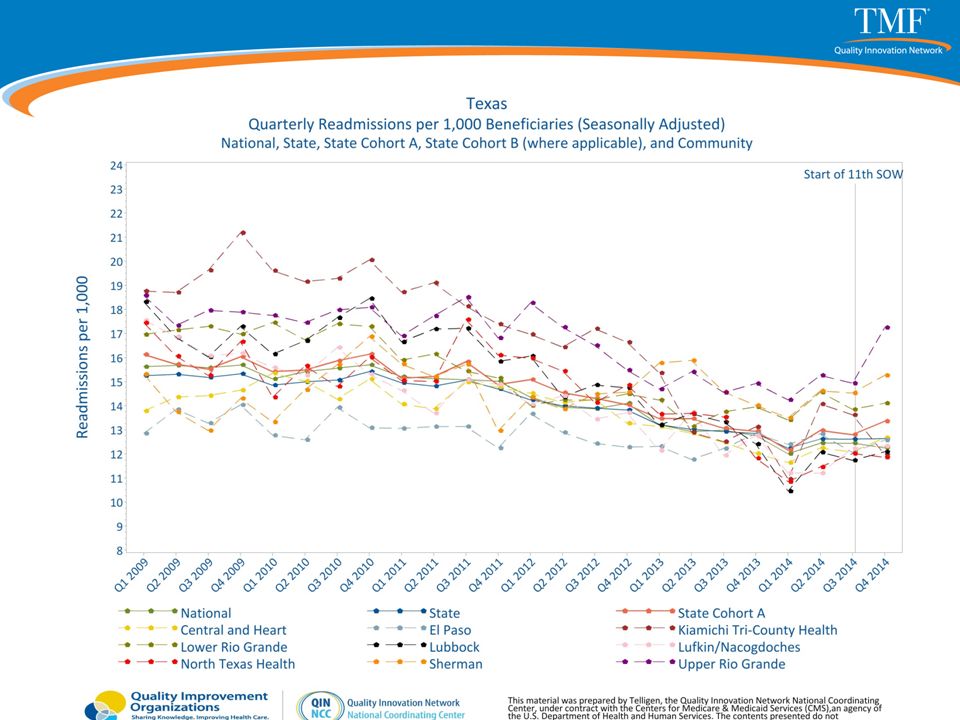
QIN Region and Texas Rate of 30-Day Hospital Readmissions 19 Source: Medicare Part A Claims Data

22
Communities and Readmissions Communities are all unique Community needs and barriers are most often best solved within that community Patients go from one provider to the next within a given community so there is more focus on coordinating within the community providers instead of working in silos.

23
Community-wide Effort Across All Care Settings Interventions promote seamless transitions across care settings, focusing on patients’ discharge from hospitals to other levels of care: IRFs, HHAs, SNFs, LTACs, Dialysis, Hospice, Physicians, Assisted Living Facilities Interventions that target the highest readmission risks › By diagnosis and type of medications taken › By frequency of readmission 23

24
Best Practice Interventions: Project Re-Engineered Discharge (RED) – hospitals MATCH or IHI Global Trigger Tool- Medication Reconciliation Care Transitions Intervention (CTI) – hospitals Interventions to Reduce Acute Care Transfers (INTERACT) – nursing homes Best Practices Intervention Package (BPIP) – home health agencies Multi-Center Medication Reconciliation Quality Study (MARQUIS) Tool Kit End-of-Life options TMF QIN-QIO Learning and Action website (www.TMFQIN.org)www.TMFQIN.org 24
 – hospitals MATCH or IHI Global Trigger Tool- Medication Reconciliation Care Transitions Intervention (CTI) – hospitals Interventions to Reduce Acute Care Transfers (INTERACT) – nursing homes Best Practices Intervention Package (BPIP) – home health agencies Multi-Center Medication Reconciliation Quality Study (MARQUIS) Tool Kit End-of-Life options TMF QIN-QIO Learning and Action website ( 24")
25
Resources TMF QIN-QIO http://www.TMFQIN.org Partnership for Patients http://partnershipforpatients.cms.gov/ Interact http://interact2.net/index.aspx 25

26
For more information Mary B. Healy RN, Mary.Healy@area-b.hcqis.orgMary.Healy@area-b.hcqis.org Cindy Bigbee RN, MSN Cindy.Bigbee@area-b.hcqis.orgCindy.Bigbee@area-b.hcqis.org Donna Zimmerman RN,BSN Donna.Zimmerman@area-b.hcqis.orgDonna.Zimmerman@area-b.hcqis.org Julie Baran RN Julie.Baran@area-b.hcqis.orgJulie.Baran@area-b.hcqis.org Jim Turpin- ADE Jim.Turpin@area-b.hcqis.orgJim.Turpin@area-b.hcqis.org Marie Richards Marie.Richards@area-b.hcqis.orgMarie.Richards@area-b.hcqis.org Vanessa Andow CHPQ – Project Director, Readmissions, Medication Safety, Behavioral Health Vanessa.Andow@area-b.hcqis.org 26 This material was prepared by TMF Health Quality Institute, the Medicare Quality Innovation Network Quality Improvement Organization, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents do not necessarily reflect CMS policy. 11SOW-QINQIO-C3-14-06
, an agency of the U.S. Department of Health and Human Services. The contents do not necessarily reflect CMS policy. 11SOW-QINQIO-C")
27
Next Steps

Similar presentations






 A Community Collaboration.>")



>")








