Download presentation
Presentation is loading. Please wait.

1
Advances in Genetic Testing for Inheritable Bleeding Disorders
Keith Gomez Haemophilia and Thrombosis Centre Royal Free Hospital

2
Overview Status of genetic testing Use in clinical practice
New technologies Future challenges

3
Clinical Uses of Genetic Diagnosis
Prediction of phenotype Inhibitor formation Assay discrepancy Confirmation of severity Identification of carriers / relatives Pre-natal and pre-implantation genetic diagnosis Funded by the NHS for prevention of severe cases

4
Testing Strategy for Mutation Detection
Haemophilia B All Severities Sequencing Single nucleotide variations Multiplex ligation-dependent probe amplification Large mutations

5
Testing Strategy for Mutation Detection
Haemophilia A Severe Non-severe Inversions Large insertions or deletions Single nucleotide variations PCR Southern MLPA Southern Sequencing PCR: Polymerase chain reaction; MLPA: Multiplex ligation-dependent probe amplification

6
National Haemophilia Database 2014
Coagulation Defect Patients in Register Treated Total Male Female Haemophilia A 5,686 - 54% Haemophilia B 1,205 55% Haemophilia A Carrier 1,377 5% Haemophilia B Carrier 425 12% Von Willebrand Disease 10,178 3,178 6,460 11% Factor XI deficiency 2,459 1,051 1,408 3% Factor VII deficency 964 461 503 6% Other factor deficiencies 1,247 515 732 Platelet Dysfunction 1,768 570 1,198 Glanzmann Thrombasthenia 119 50 69 29% Total Registered Patients 26,581 13,696 12,885 21%

7
Current Genetic Tests for Bleeding Disorders
Genetic Testing Haemophilia A and B Readily available von Willebrand Disease Limited availability of partial sequence Other factor deficiencies Limited availability Platelet Disorders with gene identified (e.g. Glanzmann’s) Very limited availability Platelet Disorders of no gene identified No test
 Very limited availability. Platelet Disorders of no gene identified. No test.")
8
Human Genome Project Sequence the entire human DNA sequence
Map and characterise all genes Started in 1990, completed in 2003 3,234 Mbp <2% contains 25,000 protein coding genes

9
Comparison of Genetic Testing Strategies
Method Description Advantages Disadvantages Single Gene All tests for a single gene Identifies nearly all mutations at a specific locus May need multiple tests Variable costs Exome panel (ThromboGenomics) Coding regions from selected genes Rapid Low cost Fewer VUS Only tests genes on the panel May miss gross abnormalities Whole Exome Sequencing (BRIDGE) Screens all exomes (2%) in the genome Covers entire human coding sequencing Discovers new genes Laborious More VUS Whole Genome Sequencing (BRIDGE) >99% of human sequence (coding and non-coding) Non-coding sequence covered Includes regulatory elements Very laborious Many VUS Exomes = coding sequence and flanking regions VUS = Variant of uncertain significance
 Coding regions from selected genes. Rapid. Low cost. Fewer VUS. Only tests genes on the panel. May miss gross abnormalities. Whole Exome Sequencing (BRIDGE) Screens all exomes (2%) in the genome. Covers entire human coding sequencing. Discovers new genes. Laborious. More VUS. Whole Genome Sequencing (BRIDGE) >99% of human sequence (coding and non-coding) Non-coding sequence covered. Includes regulatory elements. Very laborious. Many VUS. Exomes = coding sequence and flanking regions. VUS = Variant of uncertain significance.")
10
BRIDGE or ThromboGenomics?
Patient with Inheritable Bleeding Disorder Specialised Laboratory Assays Specific gene suspected No specific genetic defect ThromboGenomics ~80 genes BRIDGE BPD Gene Discovery Platform

11
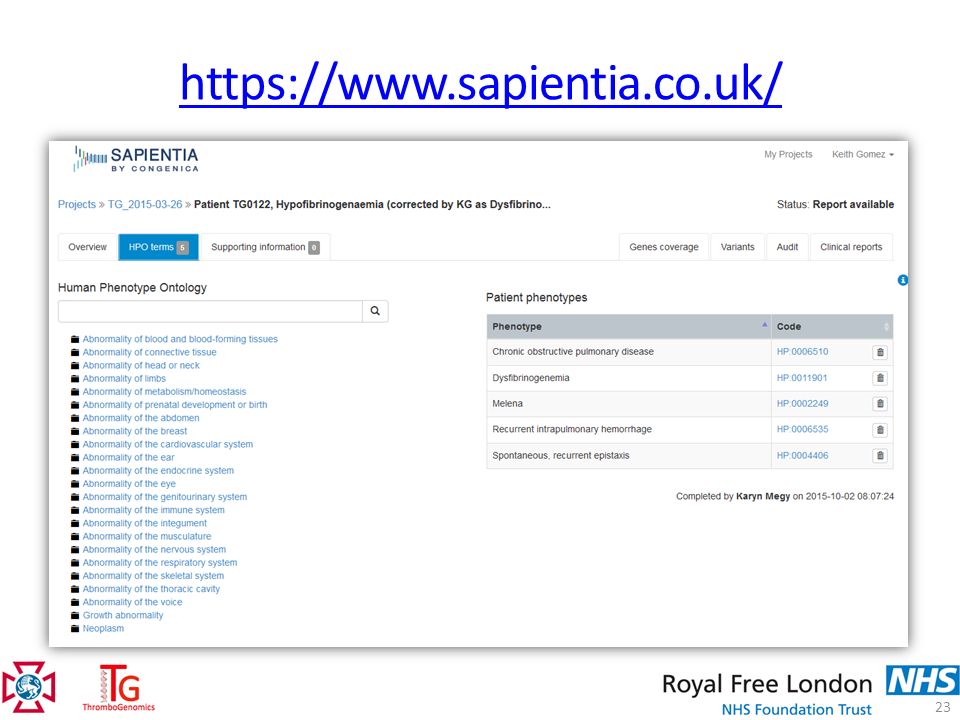
ThromboGenomics Standardisation of symptoms Exomes sequenced
Human Phenotype Ontology (HPO) Allows better genotype-phenotype correlation Exomes sequenced BRIDGE: whole genome ThromboGenomics: ~80 genes linked in OMIM to known bleeding disorders Results reviewed in MDT Report sent to referring clinician
 Allows better genotype-phenotype correlation. Exomes sequenced. BRIDGE: whole genome. ThromboGenomics: ~80 genes linked in OMIM to known bleeding disorders. Results reviewed in MDT. Report sent to referring clinician.")
12
Human Phenotype Ontology
Westbury et al. Genome Medicine 2015;7:36

13
Human Phenotype Ontology
Cluster 18 Cluster 29 Westbury et al. Genome Medicine 2015;7:36

14
ThromboGenomics vs Current Testing
One, single DNA based test Multiple tests Screening of 100+ genes simultaneously Screen one gene at a time Single laboratory Multiple laboratories each doing a few genes Affordable Expensive for large genes ThromboGenomics screens 10 times as many genes as are currently available on the NHS The ThromboGenomics platform will be regularly re-versioned to include new genes discovered by BRIDGE-BPD and others

15
ThromboGenomics – Genes
Rare Coagulation Factor Defects Haemophilias + VWD Thrombotic SERPINC1 SERPIND1 THBD PLAT PROC PROS1 HRG Undefined CYCS COL3A1 Transcription factors Coagulation factors FGA FGB FGG F2 F5 F7 F8 F9 F10 F11 F13A1 F13B SERPINE1 VKORC1 vWF SERPINF2 LMAN1 MCFD2 GGCX Membrane phospholipids ANO6 PLA2G4A Granule defects 9 HPS LYST NBEA d granules a granules NBEAL2 GFI1B STXBP2 VIPAS39 VPS33B Cytoskeletal signalling ACTN1 MYH9 FERMT3 Intracellular PLAU ANKRD26 TBXAS1 (enzyme) RASGRP2 GNE (enzyme) WAS THPO Thrombopoietin GPV ITGA2B Ca2+ Ca2+ sensor GP1Ba Receptors ITGB3 P2RY12 GP6 TBXA2R MPL GPIX GP1Bb STIM1 ORAI1 ER FLI1 GATA1 RUNX1 HOXA11 RBM8A ETV6 GNAS MASTL
 RASGRP2. GNE (enzyme) WAS. THPO. Thrombopoietin. GPV. ITGA2B. Ca2+ Ca2+ sensor. GP1Ba. Receptors. ITGB3. P2RY12. GP6. TBXA2R. MPL. GPIX. GP1Bb. STIM1. ORAI1. ER. FLI1. GATA1. RUNX1. HOXA11. RBM8A. ETV6. GNAS. MASTL.")
16
ThromboGenomics – Genes
Glanzmann Thrombasthenia Bernard Soulier Thrombotic SERPINC1 SERPIND1 THBD PLAT PROC PROS1 HRG Undefined CYCS COL3A1 Transcription factors Coagulation factors FGA FGB FGG F2 F5 F7 F8 F9 F10 F11 F13A1 F13B SERPINE1 VKORC1 vWF SERPINF2 LMAN1 MCFD2 GGCX Membrane phospholipids ANO6 PLA2G4A Granule defects 9 HPS LYST NBEA d granules a granules NBEAL2 GFI1B STXBP2 VIPAS39 VPS33B Cytoskeletal signalling ACTN1 MYH9 FERMT3 Intracellular PLAU ANKRD26 TBXAS1 (enzyme) RASGRP2 GNE (enzyme) WAS THPO Thrombopoietin GPV ITGA2B Ca2+ Ca2+ sensor GP1Ba Receptors ITGB3 P2RY12 GP6 TBXA2R MPL GPIX GP1Bb STIM1 ORAI1 ER FLI1 GATA1 RUNX1 HOXA11 RBM8A ETV6 GNAS MASTL Hermansky-Pudlak, Chediak-Higashi syndromes Genetic test for HPS only for subtype 1 and 3 subtypes of HPS leaving the other 7 subtypes with no test available. Knowing the subtype can change the patient management
 RASGRP2. GNE (enzyme) WAS. THPO. Thrombopoietin. GPV. ITGA2B. Ca2+ Ca2+ sensor. GP1Ba. Receptors. ITGB3. P2RY12. GP6. TBXA2R. MPL. GPIX. GP1Bb. STIM1. ORAI1. ER. FLI1. GATA1. RUNX1. HOXA11. RBM8A. ETV6. GNAS. MASTL. Hermansky-Pudlak, Chediak-Higashi syndromes. Genetic test for HPS only for subtype 1 and 3 subtypes of HPS leaving the other 7 subtypes with no test available. Knowing the subtype can change the patient management.")
17
ThromboGenomics – Genes
Macrothrombocytopenia Thrombotic SERPINC1 SERPIND1 THBD PLAT PROC PROS1 HRG Undefined CYCS COL3A1 FLI1 GATA1 RUNX1 HOXA11 RBM8A ETV6 GNAS MASTL Coagulation factors FGA FGB FGG F2 F5 F7 F8 F9 F10 F11 F13A1 F13B SERPINE1 VKORC1 vWF SERPINF2 LMAN1 MCFD2 GGCX Membrane phospholipids ANO6 PLA2G4A Granule defects 9 HPS LYST NBEA d granules a granules NBEAL2 GFI1B STXBP2 VIPAS39 VPS33B Cytoskeletal signalling ACTN1 MYH9 FERMT3 Intracellular PLAU ANKRD26 TBXAS1 (enzyme) RASGRP2 GNE (enzyme) WAS THPO Thrombopoietin GPV ITGA2B Ca2+ Ca2+ sensor GP1Ba Receptors ITGB3 P2RY12 GP6 TBXA2R MPL GPIX GP1Bb STIM1 ORAI1 ER 5 min Transcription factors
 RASGRP2. GNE (enzyme) WAS. THPO. Thrombopoietin. GPV. ITGA2B. Ca2+ Ca2+ sensor. GP1Ba. Receptors. ITGB3. P2RY12. GP6. TBXA2R. MPL. GPIX. GP1Bb. STIM1. ORAI1. ER. 5 min. Transcription factors.")
18
Sequencing Platform Illumina HiSeq2000 Multiplexed 24 samples per lane
The platform has been validated using 300 samples on Hiseq 2000 as 75 or 125 bp PE run with average of 150 M reads per lane. Multiplexed 24 samples per Hiseq lane. The coverage at 30x 99.5 % which is well above the 15x minimum requirement for clinical standard. This means that 99.5% of the target region has at least 30 reads. For the validation we have been using 173 samples with known mutations out of the 300. the mutations presents are 195 in total We looked at single nucleotide variants present in 173 samples Another important type of mutation in mendelian disorders are small insertions and/or deletions called INDELS and large deletions. There were 170 SNVs, 13 INDELs and 12 CNVs that we have been able to detect so far all of them with an excellent sensitivity 7.30min (For some genes there are pseudogenes the bioinformatician have algorithm to cope with this data) (For inversion we will screen the sample using established test and if positive no TG) (10 CNV all Haemophilia A patients CNV present in raw data but not picked up by the algorithm.)
 (For inversion we will screen the sample using established test and if positive no TG) (10 CNV all Haemophilia A patients CNV present in raw data but not picked up by the algorithm.)")
19
ThromboGenomics – Capture design
~80 genes (about 1.2 million bases) All exons All 5’ and 3’ UTRs Gene upstream regions 1500 base pairs Example: ITGA2B gene (Integrin alpha 2b) Gene structure 3’UTR 5’UTR Target regions Coverage The platform can screen 76 genes an we make sure to capture all the variants in all the exons, all 5’ and 3’ UTRs, all variants reported in HGMD, gene upstream regions 1500bp. Here I am showing an example. This is the gene structure with exons which represent the coding region of the gene and introns which are the non coding regions and click below the regions that are sequenced. These rows indicate the coverage which is how many time a nucleotide has been sequenced and the coverage is then summarized as a peak 6.20min
 All exons. All 5’ and 3’ UTRs. Gene upstream regions 1500 base pairs. Example: ITGA2B gene (Integrin alpha 2b) Gene structure. 3’UTR. 5’UTR. Target regions. Coverage. The platform can screen 76 genes an we make sure to capture all the variants in all the exons, all 5’ and 3’ UTRs, all variants reported in HGMD, gene upstream regions 1500bp. Here I am showing an example. This is the gene structure with exons which represent the coding region of the gene and introns which are the non coding regions and click below the regions that are sequenced. These rows indicate the coverage which is how many time a nucleotide has been sequenced and the coverage is then summarized as a peak. 6.20min.")
20
https://haemgen.haem.cam.ac.uk/thrombogenomics
21
Results Reporting Weekly web-conference Multi Disciplinary Team (MDT)
Clinician responsible for the case Clinical Geneticists Bioinformaticians Software developers Project Scientific Coordinator The results are discussed by a MDT that brings together several professionists. The chair of the project is Dr Keith Gomez form Royal Free in London (Study coordinator come back for phenotype and laboratory data)
")
22
Prediction of Mutation Effect
10 million variants in each person’s genome Can have per gene Genotype – Phenotype correlation Previously described mutation Check database Novel mutation Found in normal controls or relatives (co-segregation) Sequence alignments Structure-Function analysis
 Sequence alignments. Structure-Function analysis.")
24
Interpretation of Variants
Sequence track shows reverse complement Protein track translates from R to L, so CGG = Arg and CAG = Gln

25
ExAC control dataset Exome Aggregation Consortium (ExAC)
60,706 individuals

26
Interpretation of Variants
Sequence track shows reverse complement Protein track translates from R to L, so CGG = Arg and CAG = Gln

27
Pathogenicity Assignment
Description Criteria Clearly pathogenic High Impact Variants ≥4 previous reports in unrelated pedigrees Molecular mechanism proven Likely to be pathogenic <4 previous reports Co-segregation in pedigree with phenotype Variant of Unknown significance (VUS) Unlikely to be pathogenic Present in normal population at low frequency Clearly not pathogenic Common in normals No obvious phenotype “Polymorphism” For each mutation there are further details. The MDT takes decision about pathogenicity. The “ Clear pathogenic” option is chosen only if there are more than 4 independent cases that show the same mutation There is also a “contribution to phenotype” drop down menu to specify how the mutation observed explains the patient phenotype 10.40min
 Unlikely to be pathogenic. Present in normal population at low frequency. Clearly not pathogenic. Common in normals. No obvious phenotype. Polymorphism For each mutation there are further details. The MDT takes decision about pathogenicity. The Clear pathogenic option is chosen only if there are more than 4 independent cases that show the same mutation. There is also a contribution to phenotype drop down menu to specify how the mutation observed explains the patient phenotype min.")
28
Pathogenicity Assignment
Description Criteria Clearly pathogenic High Impact Variants ≥4 previous reports in unrelated pedigrees Molecular mechanism proven Likely to be pathogenic <4 previous reports Co-segregation in pedigree with phenotype Variant of Unknown significance (VUS) For each mutation there are further details. The MDT takes decision about pathogenicity. The “ Clear pathogenic” option is chosen only if there are more than 4 independent cases that show the same mutation There is also a “contribution to phenotype” drop down menu to specify how the mutation observed explains the patient phenotype 10.40min
 For each mutation there are further details. The MDT takes decision about pathogenicity. The Clear pathogenic option is chosen only if there are more than 4 independent cases that show the same mutation. There is also a contribution to phenotype drop down menu to specify how the mutation observed explains the patient phenotype min.")
29
Genotype-Phenotype Correlation
Relevance to Phenotype Examples Full contribution to phenotype Heterozygous variant in condition known to have dominant inheritance Homozygous variant in recessive condition Partial contribution to phenotype Heterozygous variant in recessive condition Variant in related gene in same pathway Uncertain contribution to phenotype Variant in gene with possible relationship to main locus None For each mutation there are further details. The MDT takes decision about pathogenicity. The “ Clear pathogenic” option is chosen only if there are more than 4 independent cases that show the same mutation There is also a “contribution to phenotype” drop down menu to specify how the mutation observed explains the patient phenotype 10.40min

30
MDT Outcome Multi Disciplinary Team (MDT) Causative Variant BRIDGE BPD
Consultant Haematologists, Clinical Geneticists, Bioinformaticians, Clinical Scientists, Project Scientific Coordinator, Causative Variant Yes Confirmation by Sanger sequencing Report to referring Consultant Sample considered for NGS Whole Genome Sequencing No BRIDGE BPD If the causative variant is found then it is confirmed by sanger sequencing and report goes to the referring consultant. If the causative variant is not found , sample is considered for WGS 11.20min (Study coordinator come back for phenotype and laboratory data)
")
31
ThromboGenomics Results
203 samples 134 Variant known (35 different genes) 109 SNV 13 Indels 5 Exon(s) deletions 7 Gross 79 No prior genetic analysis 74 Causal variants to BRIDGE
 109. SNV. 13. Indels. 5. Exon(s) deletions. 7. Gross. 79. No prior genetic analysis. 74. Causal. variants. to BRIDGE.")
32
ThromboGenomics – Timeline
2015 All UK Haemophilia Centres Gene list version 2.0 Available to all NHS Hospitals Accredited Service Genomics in Thrombosis and Haemostasis SSC 2016 First sample processed (Gene list version 1.0) 300 samples processed Idea submitted to ISTH by Willem Ouwehand and Thomas Kunicki 2009.….. 2012 2013 2014 TG Working Group This slide represents the evolution of the TG project from an idea to a clinical platform. In 2012 the first sample was sequenced we now have 300 samples sequenced. We have a new Open to all HC. We are now open to all UK HC but the most important thing is that the platform will be run as an accredited service providing a report at no charge if clinical data are provided. at that point the and we will let you know the day sample can be submitted without the consent under the NIHR Bio-Resource. The final goal is to make this platform available to the all NHS hospital in This project is everseen by by the ISTH (From July the platform will be available as a clinical platform where DNA is extracted in a clinical accredited lab, pull down and if positive results mutation verified in clinical lab and report will come from a clinical accredited lab) SSC = Scientific and Standardization Committee
 300 samples. processed. Idea submitted to ISTH. by Willem Ouwehand. and Thomas Kunicki … TG Working Group. This slide represents the evolution of the TG project from an idea to a clinical platform. In 2012 the first sample was sequenced we now have 300 samples sequenced. We have a new Open to all HC. We are now open to all UK HC but the most important thing is that the platform will be run as an accredited service providing a report at no charge if clinical data are provided. at that point the and we will let you know the day sample can be submitted without the consent under the NIHR Bio-Resource. The final goal is to make this platform available to the all NHS hospital in This project is everseen by by the ISTH. (From July the platform will be available as a clinical platform where DNA is extracted in a clinical accredited lab, pull down and if positive results mutation verified in clinical lab and report will come from a clinical accredited lab) SSC = Scientific and Standardization Committee.")
33
ThromboGenomics – Global Network

34
Genomics in T&H SSC Committee
Acknowledgements – TG Funding Genomics in T&H SSC Committee Chair - Willem H Ouwehand, Cambridge UK Dan Bellissimo, Pittsburgh, USA Paul Bray, Philadelphia, USA Kathleen Freson, Leuven, Belgium Anne Goodeve, Sheffield, UK Michele Lambert, Philadelphia, USA Pieter Reitsma, Leiden, The Netherland Co-chairs Anthony Attwood Louise Daugherty Cedric Ghevaert Jennifer Jolley Myrto Kostadima Karyn Megy Sofia Papadia Chris Penkett Ilenia Simeoni Jonathan Stephens Ernest Turro Matthias Ballmaier Marco Cattaneo Jose Guerrero Dan Hampshire Marian Hill Marguerite Neerman- Arbez Nancy Hogg Paquita Nurden Peter Smethurst William Stevenson Sarah Westbury Tadbir Bariana Peter Collins Ron Kerr Mike Laffan Claire Lentaigne Ri Liesner Christopher Ludlam Carolyn Millar Andrew Mumford Amit Nathwani David Perry Suthesh Sivapalaratnam As mentioned before this TG is the results of national and international collaborations and here there are some of the people involved. Thank you for your attention. I am very happy to take questions 12.00min CAMBRIDGE MEMBERS CURATORS CONTRIBUTORS

Similar presentations