Download presentation
Presentation is loading. Please wait.

1
Dana Ben-Ami benamidana@gmail.com September 2009 Clinical Practice Screening for Colorectal Cancer David A. Lieberman, M.D. N Engl J Med Volume 361(12):1179-1187 September 17, 2009
: September 17,")
2
Case Vignette A healthy 76-year-old woman presents as a new patient for primary care. She reports having one daily bowel movement and no rectal bleeding. She has no family history of colorectal cancer. She reports having negative stool card tests during gynecologic examinations, most recently at 65 years of age. Would you advise this patient to undergo colon- cancer screening, and if so, what test would you recommend?

3
The Clinical Problem Colorectal cancer (CRC) is the second leading cause of death from cancer in the United States. 2009: an estimation of 147,000 newly diagnosed cases and nearly 50,000 deaths associated with CRC. The incidence has been slowly decreasing since 1985. Screening of asymptomatic persons resulting in a reduction in mortality. There are several different screening tests, each with advantages and limitations.

4
Identification of High-Risk Persons A first-degree relative with colorectal cancer: -Before 50 years of age (familial adenomatous polyposis, hereditary nonpolyposis colorectal cancer syndrome, MutY homolog (MUTYH) polyposis). -At 50 years of age or older Colonoscopy is the preferred screening – either at the age of 40 or when the patient is 10 years younger than the age at which the family member received a diagnosis of CRC. Chronic ulcerative colitis or colitis d/t Crohn’s disease: Surveillance with colonoscopy, generally beginning 8 to 10 years after diagnosis.

5
Average-Risk Persons Dietary factors (diets high in fat or low in fiber, calcium, or both) Obesity Low levels of physical activity Tobacco smoking High alcohol intake The regular use of aspirin or NSAIDS and the use of HRT have reduced the risk of new adenomas or cancer.
 Obesity Low levels of physical activity Tobacco smoking High alcohol intake The regular use of aspirin or NSAIDS and the use of HRT have reduced the risk of new adenomas or cancer.")
6
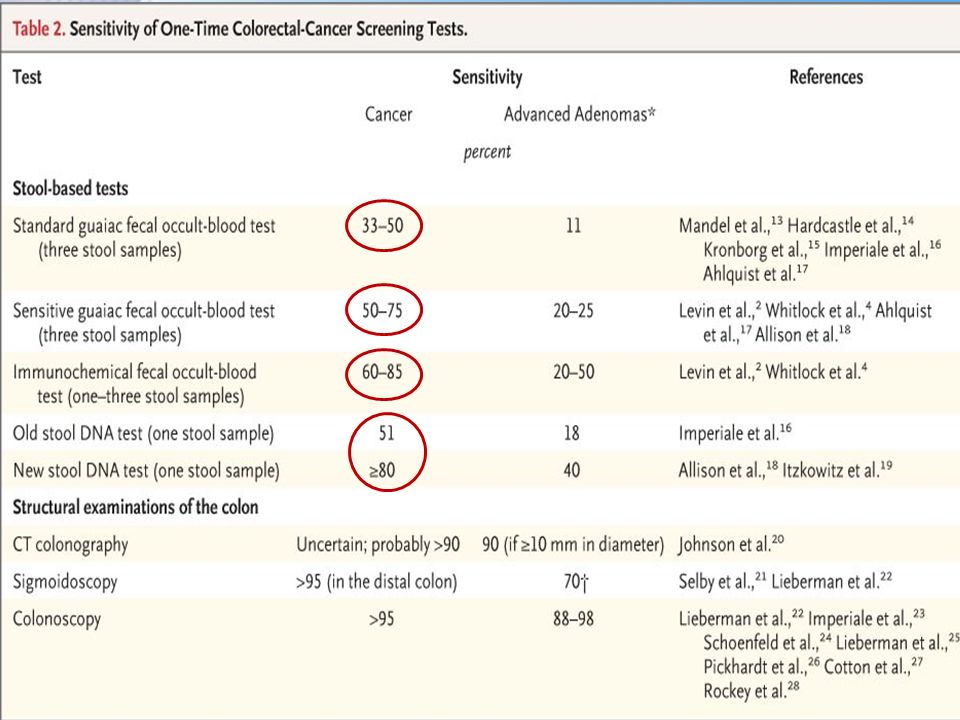
Fecal Screening Tests There are two types of fecal occult-blood tests: The standard test, which detects peroxidase activity of hem The fecal immunochemical test Stool DNA tests Persons with positive occult-blood tests have a risk of cancer that is 3-4 times as high as that among persons with negative tests. Standard guaiac tests which were administered annually or biennially over a period of 10 to 13 years resulted in a reduction in mortality from CRC of 15 to 33%.

8
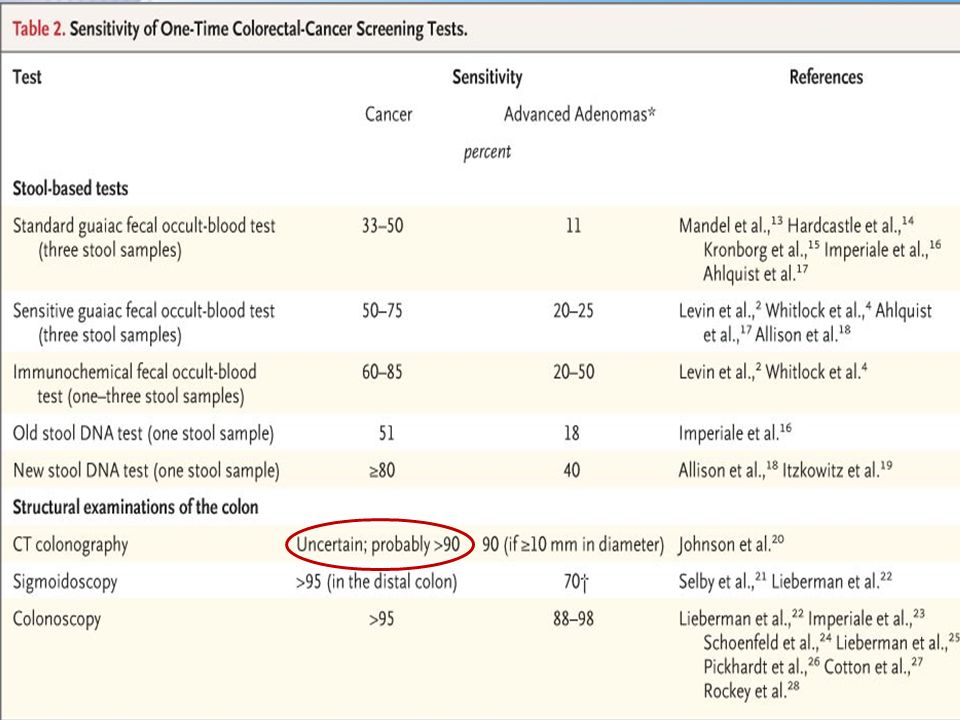
Computed tomographic (CT) colonography Requires complete bowel preparation. The detection rate for polyps that are 10 mm or larger in diameter is 90%, and for polyps that are 6 mm or larger in diameter is 78%. There is uncertainty about the detection rate for flat polyps The rate of referral for colonoscopy is an important element of program cost. Radiation exposure associated with CT colonography could increase the risk of cancer. The rate of extracolonic findings that require further evaluation is an important driver of cost

11
Sigmoidoscopy Requires bowel preparation. There is uncertainty about the usefulness of sigmoidoscopy in reducing mortality from colorectal cancer More than 30% of patients with advanced neoplasia have only proximal lesions that would not be identified with sigmoidoscopy (women > men, age > 60 years)
.")
13
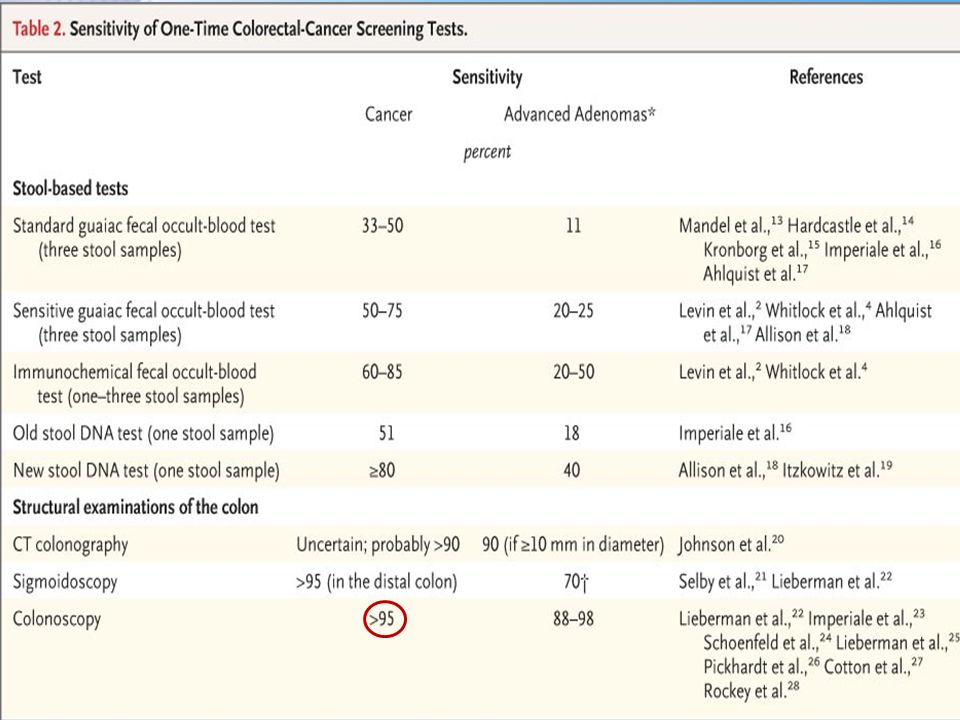
Colonoscopy Lesions that are 10 mm or larger in diameter may be missed in 2 to 12% of patients, and he detection of flat adenomas is especially difficult. The recommended 10-year interval for repeat examination after negative colonoscopic findings is based largely on case–control studies. When colonoscopy is performed by a trained endoscopist, the risk of serious adverse events is 3-5 :1000 With advancing age and coexisting conditions, the risks associated with colonoscopy increase and the benefit diminishes because of a shorter life expectancy.

15
Areas of Uncertainty Screening recommendations do not vary according to age and race or ethnic group, but screening outcomes differ according to these characteristics. Women in comparison to men Blacks in comparison to whites The American College of Gastroenterology supports the initiation of screening in blacks at 45 years of age 2

16
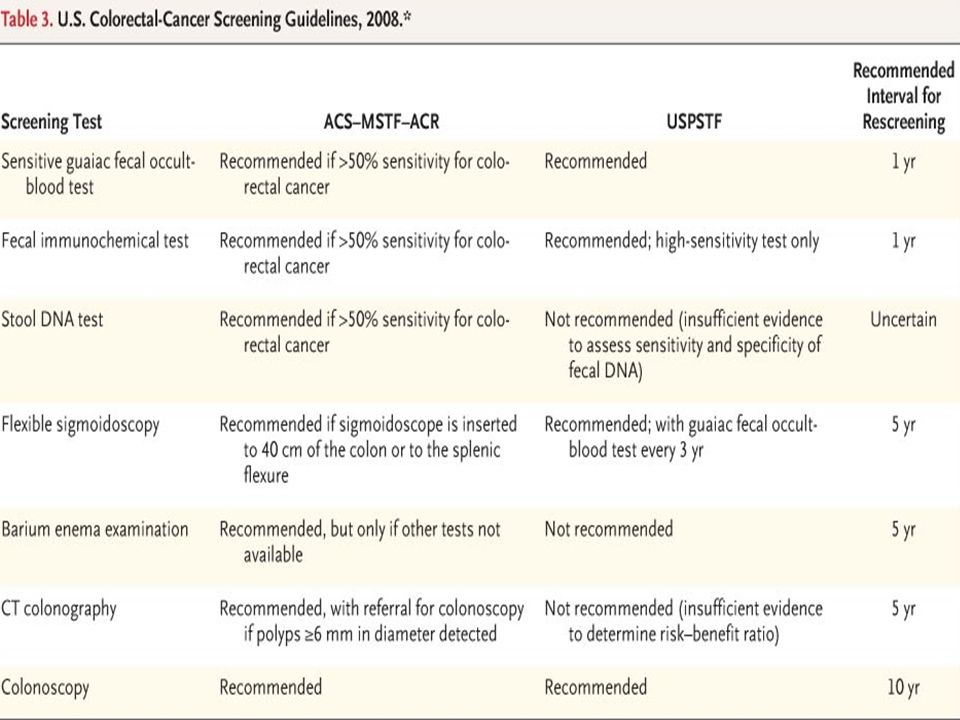
Guidelines Two new sets of guidelines for colorectal-cancer screening in the United States (from the U.S. Preventive Services Task Force [USPSTF] and joint guidelines from the American Cancer Society, the U.S. Multisociety Task Force on Colorectal Cancer, and the American College of Radiology) were published in 2008 The latter, joint guidelines recommend structural examinations of the colon that may lead to cancer prevention as the preferred test, if resources are available. 2 Both sets of guidelines recommend a sensitive guaiac test or fecal immunochemical test if fecal testing is required. Patients should be informed that colonoscopy is necessary if the test results are positive and that the test should be repeated annually if the results are negative. The USPSTF does not recommend CT colonography and stool DNA testing, which are new techniques that are associated with many uncertainties (Table 1). 3 Guidelines from the American College of Gastroenterology recommend colonoscopy as the preferred screening test. 55Table 1 3 55 The USPSTF concludes that screening should not be routinely recommended in persons older than 75 years of age, and it should not be recommended at all in persons older than 85 years of age, even though the risk of colorectal cancer and advanced polyps continues to increase with age. 1,25 If persons between the ages of 75 and 85 years have never undergone screening, decisions about screening should be individualized according to health status. 125 Internationally, there is considerable variation among screening recommendations. Fecal occult-blood testing is recommended in Europe and Canada. Alternatives to fecal occult-blood testing are sigmoidoscopy in the United Kingdom, Italy, and Norway and colonoscopy in Germany, Austria, Poland, and Italy.
 were published in 2008 The latter, joint guidelines recommend structural examinations of the colon that may lead to cancer prevention as the preferred test, if resources are available. 2 Both sets of guidelines recommend a sensitive guaiac test or fecal immunochemical test if fecal testing is required. Patients should be informed that colonoscopy is necessary if the test results are positive and that the test should be repeated annually if the results are negative. The USPSTF does not recommend CT colonography and stool DNA testing, which are new techniques that are associated with many uncertainties (Table 1). 3 Guidelines from the American College of Gastroenterology recommend colonoscopy as the preferred screening test. 55Table The USPSTF concludes that screening should not be routinely recommended in persons older than 75 years of age, and it should not be recommended at all in persons older than 85 years of age, even though the risk of colorectal cancer and advanced polyps continues to increase with age. 1,25 If persons between the ages of 75 and 85 years have never undergone screening, decisions about screening should be individualized according to health status. 125 Internationally, there is considerable variation among screening recommendations. Fecal occult-blood testing is recommended in Europe and Canada. Alternatives to fecal occult-blood testing are sigmoidoscopy in the United Kingdom, Italy, and Norway and colonoscopy in Germany, Austria, Poland, and Italy..")
17
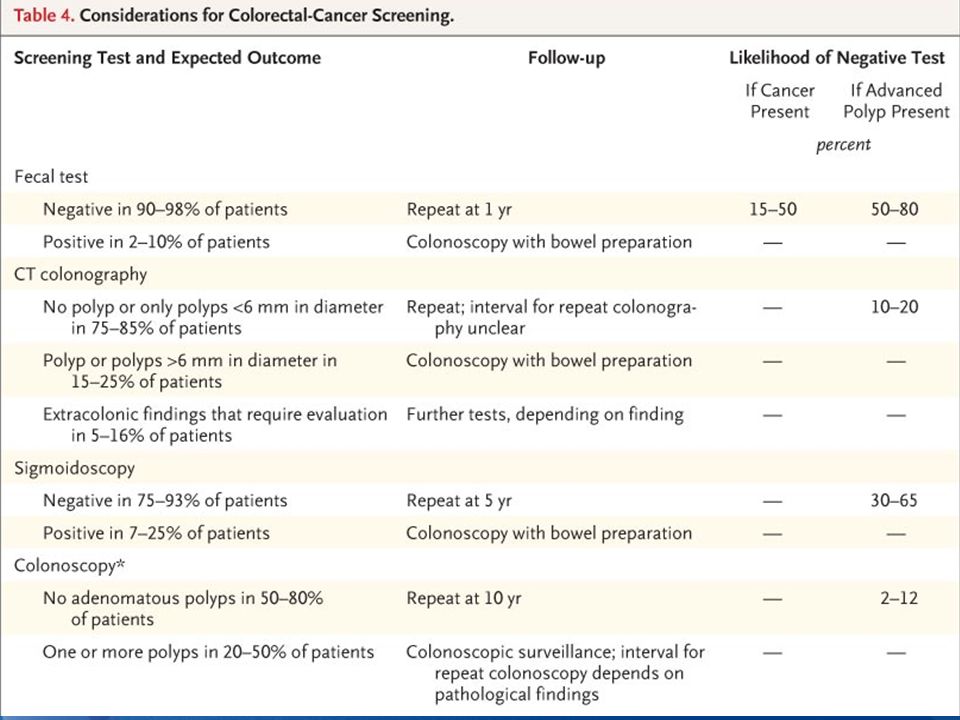
Conclusions and Recommendations Colorectal-cancer screening should begin with a process of informed decision making (Table 4). Patients should be informed that there is strong evidence that screening persons who are at average risk is effective in reducing the risk of death from colorectal cancer, but that there is no perfect screening test and each program has advantages, limitations, and uncertainties (Table 1). Patients also should be informed about the "downstream" benefits and risks associated with the various screening tests, including the need for follow-up tests and the likelihood that the test will detect important pathologic findings, if present.Table 4Table 1 Although the USPSTF does not recommend routine screening in persons older than 75 years of age, the healthy 76-year-old woman in the vignette has never undergone proper screening and she should be offered it. Given that her sex and age are associated with an increased risk of neoplasia in the proximal colon, I would recommend colonoscopy. She should be referred to an endoscopist who monitors quality and meets benchmarks for colonoscopic examination. If this test is negative, she will not need any further screening in her lifetime. If she prefers fecal testing, she should understand the limitations of one-time testing for the detection of advanced polyps and cancer and the need for repeat testing over the next few years.
. Patients also should be informed about the downstream benefits and risks associated with the various screening tests, including the need for follow-up tests and the likelihood that the test will detect important pathologic findings, if present.Table 4Table 1 Although the USPSTF does not recommend routine screening in persons older than 75 years of age, the healthy 76-year-old woman in the vignette has never undergone proper screening and she should be offered it. Given that her sex and age are associated with an increased risk of neoplasia in the proximal colon, I would recommend colonoscopy. She should be referred to an endoscopist who monitors quality and meets benchmarks for colonoscopic examination. If this test is negative, she will not need any further screening in her lifetime. If she prefers fecal testing, she should understand the limitations of one-time testing for the detection of advanced polyps and cancer and the need for repeat testing over the next few years..")
20
Case Vignette A healthy 76-year-old woman presents as a new patient for primary care. She reports having one daily bowel movement and no rectal bleeding. She has no family history of colorectal cancer. She reports having negative stool card tests during gynecologic examinations, most recently at 65 years of age. Would you advise this patient to undergo colon- cancer screening, and if so, what test would you recommend?

21
Original Article Capsule Endoscopy versus Colonoscopy for the Detection of Polyps and Cancer André Van Gossum, M.D., Miguel Munoz Navas, M.D., Iñaqui Fernandez-Urien, M.D., Cristina Carretero, M.D., Gérard Gay, M.D., Michel Delvaux, M.D., Marie Georges Lapalus, M.D., Thierry Ponchon, M.D., Horst Neuhaus, M.D., Michael Philipper, M.D., Guido Costamagna, M.D., Maria Elena Riccioni, M.D., Cristiano Spada, M.D., Lucio Petruzziello, M.D., Chris Fraser, M.D., Aymer Postgate, M.D., Aine Fitzpatrick, M.D., Friedrich Hagenmuller, M.D., Martin Keuchel, M.D., Nathalie Schoofs, M.D., and Jacques Devière, M.D. N Engl J Med Volume 361(3):264-270 July 16, 2009
: July 16,")
22
Background On the basis of the small-bowel capsule endoscope (PillCam SB), the PillCam COLON capsule endoscope, an ingestible capsule consisting of an endoscope equipped with a video camera at both ends, was designed especially for visualizing the colon A less invasive screening tool might serve as an additional screening method for the early detection of colorectal cancer and adenomatous polyps The study sponsor donated the PillCams
, the PillCam COLON capsule endoscope, an ingestible capsule consisting of an endoscope equipped with a video camera at both ends, was designed especially for visualizing the colon A less invasive screening tool might serve as an additional screening method for the early detection of colorectal cancer and adenomatous polyps The study sponsor donated the PillCams")
23
Aims of study To compare the performance of capsule endoscopy with colonoscopy for the detection of colorectal polyps and cancers To evaluate the accuracy of detecting: -Colonic polyps -Advanced adenomas -Carcinomas

24
Study Group Patients with known colonic disease: -Patients with a history of CRC or adenomatous polyps for whom at least 3 years had passed since their last colonoscopy -Patients with any positive findings on radiographic examinations -Patients with known ulcerative colitis Patients with suspected colonic disease: At least one of the following symptoms: rectal bleeding, hematochezia, melena, a recent change in bowel habits, or a positive fecal occult-blood test. Methods

25
Exclusion criteria: Age younger than 18 years The presence of dysphagia, congestive heart failure, renal insufficiency, intestinal obstruction, a life-threatening condition, or a pacemaker or other implanted electromedical device Current pregnancy Abdominal surgery in the past 6 months Inability to provide informed consent Current participation in another clinical study Methods

26
Study Design The PillCam COLON capsule is an ingestible capsule equipped with an endoscope that has two imagers, enabling it to acquire video images from both ends The device acquires images at a rate of 4 frames per second The preprogrammed "sleep" mode allows recording of images from the esophagus and the stomach for 3 minutes before the capsule switches to sleep mode for 1 hour 45 minutes in order to conserve battery life Colonoscopy was performed after capsule endoscopy, on either the same day as ingestion or the next morning Adverse events were recorded. Events were graded as mild, moderate, or severe Methods

27
The eight participating centers enrolled 332 patients Four patients (1.2%) withdrew before completing the study documents and were not included in the analysis Eight patients were not included in the analysis of the accuracy of polyp detection: in five patients (1.5%), the capsule did not reach the colon before the end of the capsule's battery life in two patients (0.6%), the colonoscopy was incomplete because the colonoscope could not be passed beyond the sigmoid colon one patient (0.3%) was unable to swallow the capsule Therefore, 320 patients were included in the accuracy analysis Results
 withdrew before completing the study documents and were not included in the analysis Eight patients were not included in the analysis of the accuracy of polyp detection: in five patients (1.5%), the capsule did not reach the colon before the end of the capsule s battery life in two patients (0.6%), the colonoscopy was incomplete because the colonoscope could not be passed beyond the sigmoid colon one patient (0.3%) was unable to swallow the capsule Therefore, 320 patients were included in the accuracy analysis Results")
28
Known or Suspected Positive Colonic Findings in the 320 Patients Included in the Accuracy Analysis, According to Age Van Gossum A et al. N Engl J Med 2009;361:264-270

29
At "wake up” time, the capsule remained proximal to the cecum in 312 of the 320 patients (97.5%). Of the 320 patients, 221 (69.1%) excreted the capsule within 6 hours after ingestion, and 297 (92.8%) within 10 hours. All patients excreted the capsule naturally, 319 (99.7%) within 16 hours after ingestion, and 1 (0.3%) during the 4th week after ingestion A total of 27 adverse events were reported in 26 (7.9%) of the 328 patients who completed the study In 22 of these 26 patients, adverse events were related to the bowel preparation and included abdominal discomfort, nausea, vomiting, and headache Results
 excreted the capsule within 6 hours after ingestion, and 297 (92.8%) within 10 hours. All patients excreted the capsule naturally, 319 (99.7%) within 16 hours after ingestion, and 1 (0.3%) during the 4th week after ingestion A total of 27 adverse events were reported in 26 (7.9%) of the 328 patients who completed the study In 22 of these 26 patients, adverse events were related to the bowel preparation and included abdominal discomfort, nausea, vomiting, and headache Results.")
30
Sensitivity and Specificity of Capsule Endoscopy for the Detection of the Lesions Detected by Colonoscopy

31
Lesions Observed on Colonoscopy and Capsule Endoscopy

32
The PillCam COLON capsule functioned appropriately in 97.5% of the patients. Bowel-preparation regimen used for capsule endoscopy was more extensive than that used for colonoscopy Capsule endoscopy is a safe method of visualizing the colonic mucosa without the need for sedation or insufflation. The sensitivity of capsule endoscopy for detecting colonic polyps, advanced adenomas, and colorectal cancer was relatively low in comparison with colonoscopy. The patients in this study were not representative of a typical screening population Discussion

33
DANA BEN-AMI benamidana@gmail.com September 2009 Thank you..

Similar presentations