Download presentation
Presentation is loading. Please wait.

1
Liver Enzymes, Viral Hepaitits, Autoimmune Hepatitis Kimiko Suzue MD, Ph.D. Department of Pathology

3
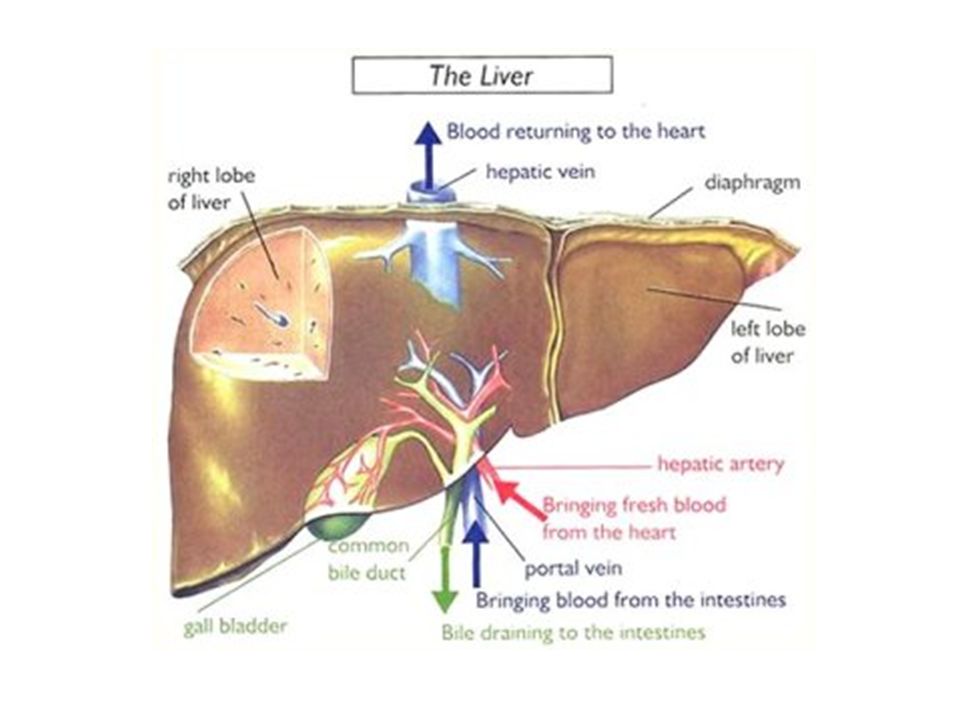
Liver Functions Protein synthesis Bile secretion Bilirubin conjugation and excretion Metabolite storage –Triglycerides and glycogen –Vitamins (especially vitamin A) Metabolic functions –Gluconeogenesis –Urea production Detoxification and inactivation –Many drugs and other substances metabolized here
 Metabolic functions –Gluconeogenesis –Urea production Detoxification and inactivation –Many drugs and other substances metabolized here")
4
Liver Functions Enormous functional reserve Typically 80% to 90% of hepatic functional capacity must be lost before liver failure occurs Chronic liver disease resulting in liver failure is much more common than fulminant hepatic failure (sudden, massive liver destruction) Liver disease is typically inisidious and hepatic injury may first become apparent from abnormal laboratory tests
 Liver disease is typically inisidious and hepatic injury may first become apparent from abnormal laboratory tests")
5
Laboratory evaluation of liver disease Hepatocyte function: - Serum albumin - Prothrombin time: measuring coagulation factors (II, V, VII, X); prolonged in liver cirrhosis - Serum ammonia Hepatocyte injury (enzymes normally present inside the hepatocytes and released with injury): - Serum aspartate aminotransferase (AST) - Serum alanine aminotransferase (ALT) - Serum lactate dehydrogenase (LDH)
; prolonged in liver cirrhosis - Serum ammonia Hepatocyte injury (enzymes normally present inside the hepatocytes and released with injury): - Serum aspartate aminotransferase (AST) - Serum alanine aminotransferase (ALT) - Serum lactate dehydrogenase (LDH)")
6
Laboratory evaluation of liver disease Biliary excretory function: Bile canalicular membrane enzymes -Serum alkaline phosphatase -Serum gamma-glutamyl transpeptidase (GGT) Normally secreted in bile -Serum bilirubin Searching for etiology: - Hepatitis viral antigens and antibodies - Autoimmune antibodies: for autoimmune hepatitis - Tissue iron and copper: for hemochromatosis and Wilson disease
 Normally secreted in bile -Serum bilirubin Searching for etiology: - Hepatitis viral antigens and antibodies - Autoimmune antibodies: for autoimmune hepatitis - Tissue iron and copper: for hemochromatosis and Wilson disease")
7
Aminotransferases Together, Aspartate Aminotransferase (AST) and Alanine Aminotransferase (ALT are referred to as the -‘liver transaminases’, (nl 8-35 U/L each) Widely distributed! AST present in cardiac muscle, liver, skeletal muscle, kidney, brain, lung and pancreas - Elevated AST with normal ALT, consider non-hepatic causes (MI, pericarditis, muscle disease) ALT is present in liver and kidney, thus - ALT is more specific for liver
 ALT is present in liver and kidney, thus - ALT is more specific for liver.")
8
Aminotransferases AST:ALT ratio is over 2 in 80% of patients with toxic, ischemic, and alcoholic hepatitis AST:ALT is usually <1 in viral hepatitis When AST >3000U/L, etiology usually a toxin AST is over ten times the upper limit of normal in >50% of patients with acute viral hepatitis

9
Alkaline phosphatase Produced by bone, bile ducts, intestine and placenta Elevation seen in biliary disease, bone disease, bone growth (children), pregnancy, congestive heart failure, hyperthyroidism and drugs such as ibuprofen and acetominophen Adult reference range 20-130 U/ml (separate range for children and pregnant women) Sensitive indicator of hepatic metastases
, pregnancy, congestive heart failure, hyperthyroidism and drugs such as ibuprofen and acetominophen Adult reference range U/ml (separate range for children and pregnant women) Sensitive indicator of hepatic metastases")
10
Gamma-glutamyl transferase Present in biliary epithelial cells, liver, small bowel, kidney, testes, pancreas, spleen, heart, brain. Sensitive but not specific for biliary injury Present in smooth ER of hepatocytes and exposure to toxins (warfarin, barbiturates, dilantin, valproate, methotrxate, alcohol) will cause GGT increase Best test to confirm elevated AlkPhos from biliary tree
 will cause GGT increase Best test to confirm elevated AlkPhos from biliary tree.")
11
Approach to patient with elevated alkaline phosphatase AlkPhos elevated GGT elevated AlkPhos, GGT >2X Liver Ultrasound Yes No Yes Pursue non-hepatic causes (bone, etc) If no symptoms, recheck in 3-6 months
 If no symptoms, recheck in 3-6 months")
12
Bilirubin 0.2 to 0.3 grams produced daily from degradation of heme After hepatocellular uptake, the bilirubin gets conjugated with glucuronides, then excreted into bile Unconjugated hyperbilirubinemia -Hemolysis, Blood shunting (cirrhosis), Gilbert’s syndrome, Crigler-Najjar syndrome Conjugated hyperbilirubinemia -Dubin-Johnson syndrome, Hepatitis -Mechanical obstruction (PBC, PSC, tumor, stricture, stone)
, Gilbert’s syndrome, Crigler-Najjar syndrome Conjugated hyperbilirubinemia -Dubin-Johnson syndrome, Hepatitis -Mechanical obstruction (PBC, PSC, tumor, stricture, stone)")
13
Albumin Most abundant protein synthesized by liver Most abundant protein in human plasma Half-life = 20 days May be affected by nutrition, GI and renal losses Levels may be reduced in presence of edema and ascites Only in end-stage liver disease is serum albumin noticeably decreased

14
Prothrombin Time (PT) Sensitive marker for impaired hepatic function Many coagulation factors synthesized in liver and have short half-lives (Factors II and VII has half-lives) In cirrhosis, prolonged PT does not correct with intramuscular vitamin K
 Sensitive marker for impaired hepatic function Many coagulation factors synthesized in liver and have short half-lives (Factors II and VII has half-lives) In cirrhosis, prolonged PT does not correct with intramuscular vitamin K")
15
Clinical consequences of liver disease Hepatic dysfunction: -Decreased synthetic capacity leading to : Hypoalbuminemia: edema, ascites, muscle wasting, weight loss Hypoglycemia: weakness and syncope Coagulation factor deficiency: bleeding -Decreased detoxificationcapacity leading to: Hyperammonemia and increased toxic metabolites: Encephalopathy (altered behavior and disturbances in consciousness that may lead to deep coma and death) Injury to other organs by active toxins
 Injury to other organs by active toxins")
16
Clinical consequences of liver disease -Hepatorenal syndrome: Patients with severe chronic liver disease whogo into renal failure without intrinsic or functional causes of renal failure. Approximately 8% of pts with cirrhosis and ascites Decreased blood flow to the kidney - Systemic vasodilation - Renal afferent arterioles constriction Poor prognosis with median survival of 2 weeks in rapid-onset form and 6 months in insidious-onset form Liver transplantation -Hepatopulmonary syndrome Chronic liver disease, hypoxemia, pulmonary vascular dilatations

17
Clinical consequences of liver disease Jaundice: yellow discoloration of skin and sclera due to accumulation of bilirubin Cholestasis: systemic accumulation of bilirubin in addition to bile salts and cholesterol (usually secondary to obstruction) Portal hypertension in cirrhosis: increased resistance to portal blood flow -Esophageal varices -Ascites -Splenomegaly -Hemorrhoids Malignancy on top of cirrhosis
 Portal hypertension in cirrhosis: increased resistance to portal blood flow -Esophageal varices -Ascites -Splenomegaly -Hemorrhoids Malignancy on top of cirrhosis")
18
Clinical consequences of portal hypertension Robbins 18-3

19
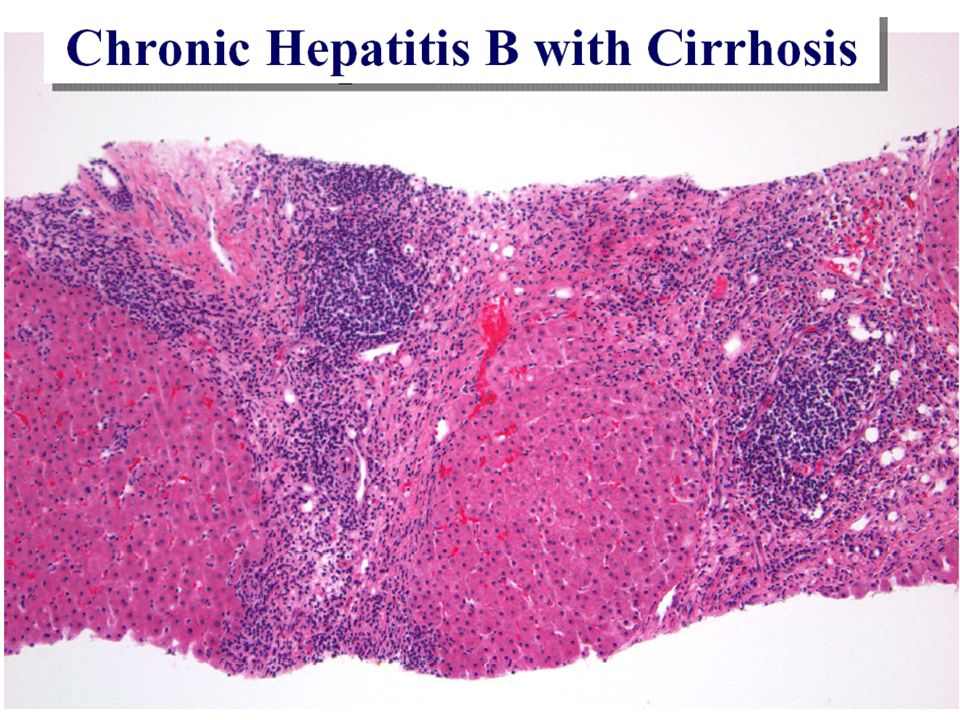
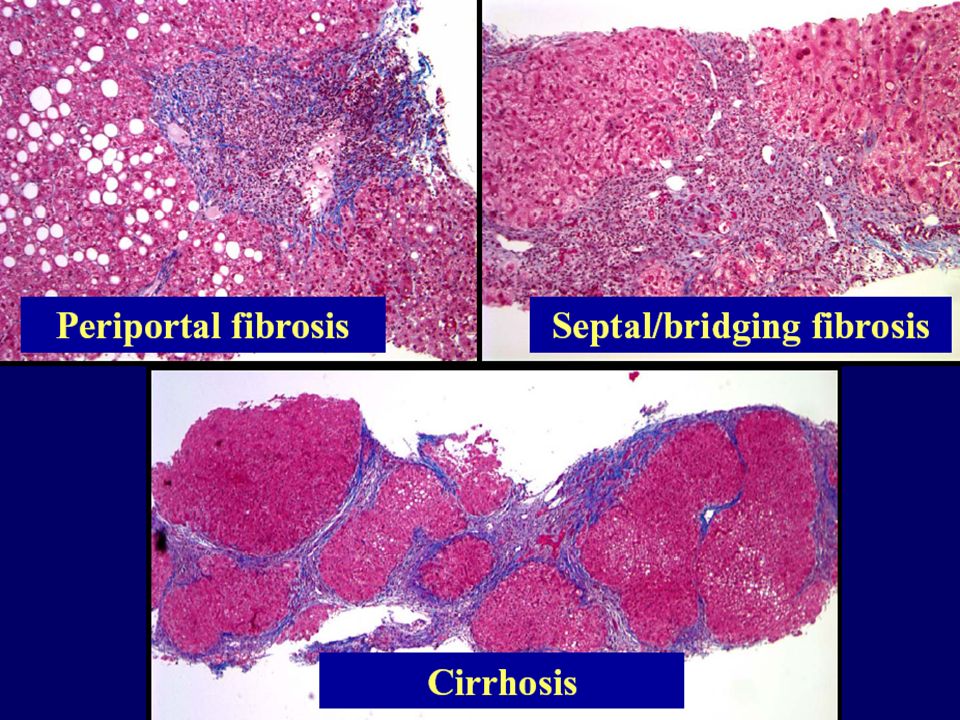
Liver cirrhosis Definition: bridging fibrous septa and parenchymal nodules with disruption of architecture. End stage for many diseases affecting the liver Mechanism: cell death, regeneration and fibrosis

20
Chronic Passive Congestion

21
Hepatic Diseases Viral hepatitis Autoimmune hepatitis Drug-induced hepatitis Fatty liver disease -Alcoholic -Non-alcoholic (NAFL) -Steatohepatitis (ASH, NASH) Hemochromatosis Wilson disease Alpha 1 antitrypsin disease Neoplasms of the liver
 -Steatohepatitis (ASH, NASH) Hemochromatosis Wilson disease Alpha 1 antitrypsin disease Neoplasms of the liver")
22
Hepatitis Acute hepatitis Viral Drug-induced Other Chronic hepatitis Autoimmune Viral Drug-induced Other

23
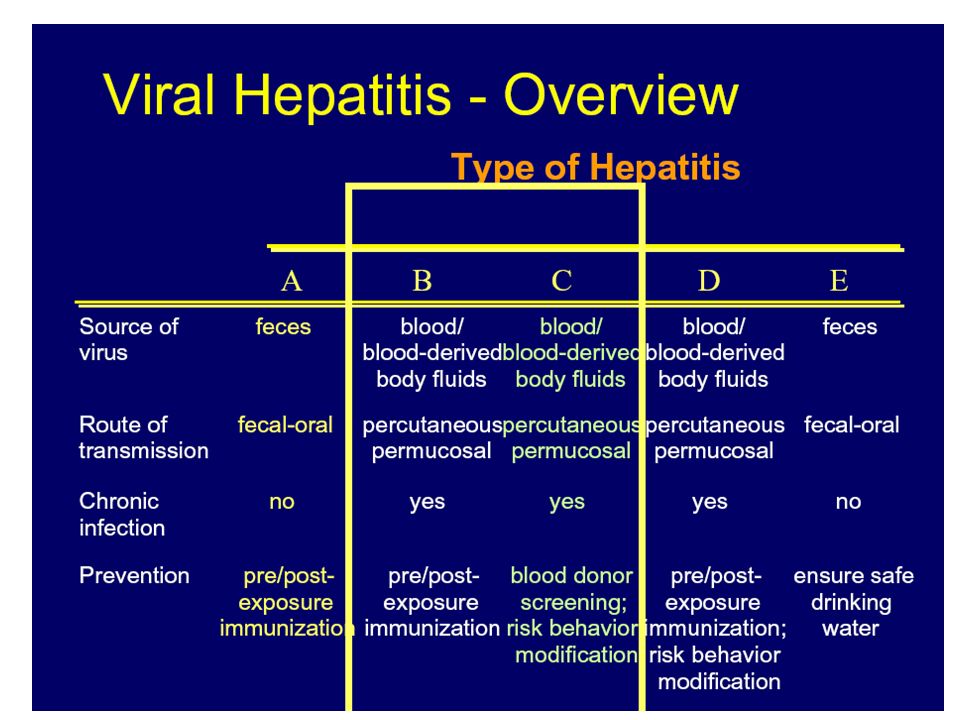
Hepatitis A virus RNA virus Mode of transmission: fecal-oral (contaminated water and food) Incubation period: 2-6 weeks Virus shedding: 2-3 weeks before and 1 week after appearance of jaundice 50% of population above age 50 are seropositive in USA, no carrier state No increased risk for chronic hepatitis, or carcinoma
 Incubation period: 2-6 weeks Virus shedding: 2-3 weeks before and 1 week after appearance of jaundice 50% of population above age 50 are seropositive in USA, no carrier state No increased risk for chronic hepatitis, or carcinoma")
24
Hepatitis B virus dsDNA virus Mode of transmission: parenteral (blood products, contaminated needles and IV drug abuse), and body fluids (including saliva) Incubation period: 4-26 weeks Carrier state: yes, 350 million carriers around the world
, and body fluids (including saliva) Incubation period: 4-26 weeks Carrier state: yes, 350 million carriers around the world")
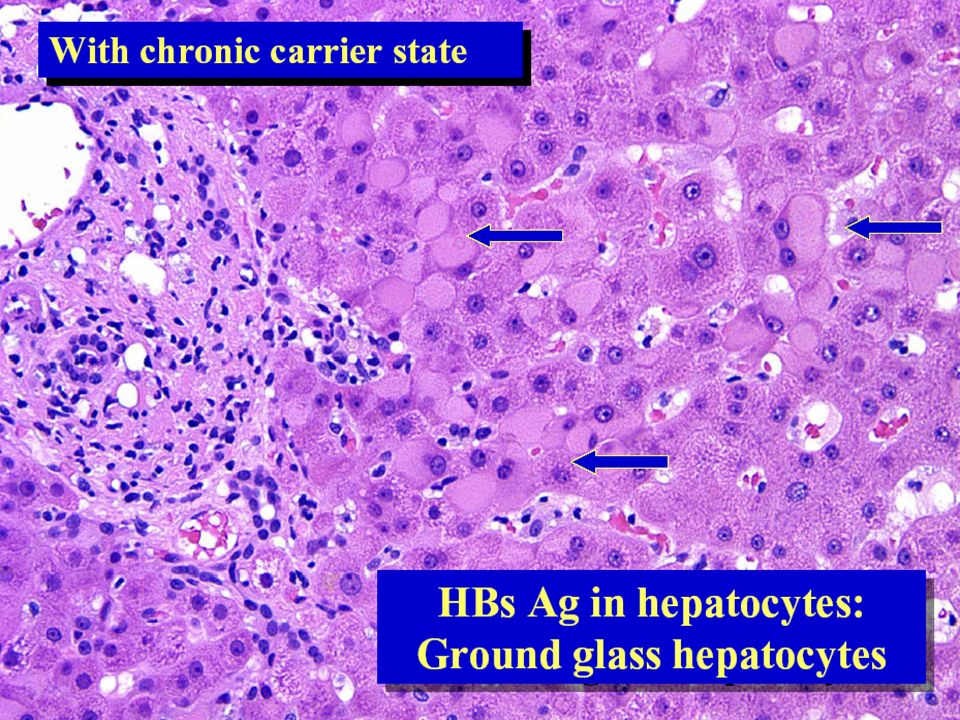
25
Hepatitis B virus Following acute infection, patients may clear infection and develop immunity or may develop chronic carrier state (10%) Production of antibodies against surface antigen (HBsAg) confers immunity. Prevention of infection by vaccination with HBsAg and by screening of donor blood/ organs

27
Hepatitis B infection: Possible outcomes Possible outcomes of infection: –Subclinical or acute hepatitis with recovery and clearance (85%); 1% of those may develop fulminant hepatitis and death –Healthy carriers (10%) –Persistent infection (5%): 80% recover and 20% develop chronic hepatitis –20% of chronic hepatitis patients develop cirrhosis and 10% of those develop hepatocellular carcinoma
; 1% of those may develop fulminant hepatitis and death –Healthy carriers (10%) –Persistent infection (5%): 80% recover and 20% develop chronic hepatitis –20% of chronic hepatitis patients develop cirrhosis and 10% of those develop hepatocellular carcinoma")
33
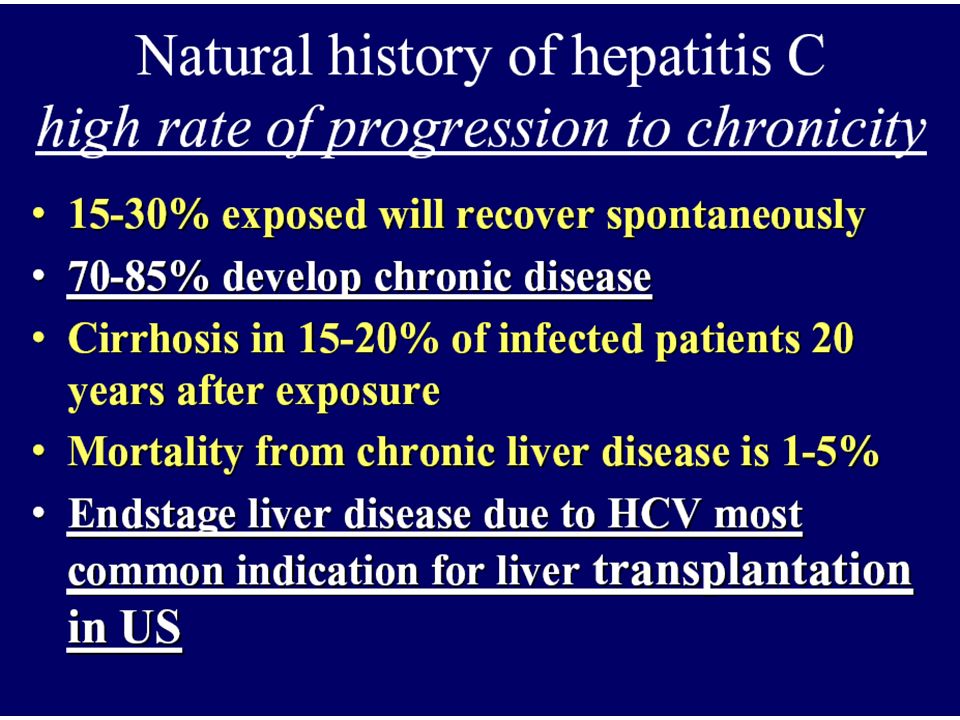
Hepatitis C ssRNA virus Mode of transmission: parenteral, sexual and vertical, 40% unknown source. It is present in the saliva. Incubation period: 2-26 weeks Outcomes of infection: HCV is the leading cause for chronic liver disease

35
Hepatitis C virus risk factors Intravenous drug abuse (54%) Multiple sex partners (36%) Surgery in last 6 months (16%) Needle stick injury (10%) Multiple contacts with an HCV-infected person (10%) Employment in medical or dental fields (1.5%) Unknown (32%)
 Multiple sex partners (36%) Surgery in last 6 months (16%) Needle stick injury (10%) Multiple contacts with an HCV-infected person (10%) Employment in medical or dental fields (1.5%) Unknown (32%)")
37
Hepatitis C virus Genomic instability: HCV RNA polymerase has poor fidelity Elevated titers of anti-HCV IgG after infection does not consistently confer protection Circulating HCV RNA persists in many patients despite the presence of neutralizing antibodies

42
Hepatitis D Defective RNA virus that needs Hep B capsule to replicate Mode of transmission: Parenteral Coinfection of B and D: mild disease with recovery in most cases, <5% chronic hepatitis Superinfection by D after B: accelerated more severe hepatitis; 80% chronic hepatitis

43
Hepatitis E ssRNA virus Mode of transmission: waterborne Incubation period: 2-8 weeks Endemic in certain populations; 40% in Indian population Self-limited infection but with higher mortality in pregnant females

44
Hepatitis Viruses Yes NoCarcinoma Rare0.1-1.0%0.1%Fulminant hepatitis >70%5-10%NoneChronic hepatitis Present NoneCarrier state Parenteral Oral-fecalTransmission Hepatitis CHepatitis BHepatitis A

46
Autoimmune hepatitis More in females (70%) The absence of serologic markers for viral hepatitis T cell-mediated autoimmune hepatocyte injury –IFN- produced by CD4+ and CD8+ T cells –CD8+ T cell mediated cytotoxicity Increased frequency of HLA-B8 and DRw3 Elevated serum IgG levels (Hypergammaglobulinemia) High titers of autoantibodies (antinuclear, anti- smooth muscle, anti-liver kidney microsome-1 antibodies)
 The absence of serologic markers for viral hepatitis T cell-mediated autoimmune hepatocyte injury –IFN- produced by CD4+ and CD8+ T cells –CD8+ T cell mediated cytotoxicity Increased frequency of HLA-B8 and DRw3 Elevated serum IgG levels (Hypergammaglobulinemia) High titers of autoantibodies (antinuclear, anti- smooth muscle, anti-liver kidney microsome-1 antibodies)")
47
Autoimmune hepatitis Associated with other forms of autoimmune disorders –Celiac disease, systemic lupus erythematosus, rheumatoid arthritis, thyroiditis, Sjogren’s syndrome and ulcerative colitis Clusters of plasma cells in the interface of portal tracts and hepatic lobules May be indolent or become fulminant hepatitis Risk for cirrhosis is 5% Respond to immunosuppressive drugs

48
Autoimmune Hepatitis

49
Autoimmune hepatitis Document a chronic hepatitis (predominant serum aminotransferase abnormality) Exclude hereditary diseases Exclude viral diseases Exclude alcohol or drug-related diseases Autoimmune serologic markers –Serum IgG > 1.5 X normla –ANA, SMA, anti-LKM Compatible histologic features –Interface hepatitis, moderate to severe –No granulomas, no biliary lesions or suggestion of other disease
 Exclude hereditary diseases Exclude viral diseases Exclude alcohol or drug-related diseases Autoimmune serologic markers –Serum IgG > 1.5 X normla –ANA, SMA, anti-LKM Compatible histologic features –Interface hepatitis, moderate to severe –No granulomas, no biliary lesions or suggestion of other disease")
Similar presentations














>")
 LIVER FUNCTION AND THE BILIARY TRACT LECTURE FOUR Dr. Essam H. Aljiffri.>")
 that progresses to cirrhosis Replacement of liver tissue.>")
 LIVER FUNCTION AND THE BILIARY TRACT LECTURE FIVE Dr. Essam H. Aljiffri.>")







