Download presentation
Presentation is loading. Please wait.

1
Left Main PCI: What is Best Practice? Ayman A. Magd, MD FSCAI Board of Trustees of SCAI Board of Trustees of SCAI Professor of Cardiology, Azhar University Interventional Fellows Course, India August, 2015

2
Disclosures none Left Main Coronary PCI: Best Practice Ayman A. Magd MD, FSCAI The following relationships exist related to this presentation

5
Left Main PCI: Patient Selection and Technique Patient Selection (Risk Models) IVUS and FFR Procedure Technique (Cases) Surveillance : Follow-up
 IVUS and FFR Procedure Technique (Cases) Surveillance : Follow-up")
6
Left Main Disease Benefit of Revascularization Caracciolo et al. Circulation 1995; 91: 2325 Long-term CASS Experience Cumulative survival estimates In 1484 CASS Registry patients with 50% LM coronary artery stenosis who were initially treated with CABG surgery or non surgical therapy. Surgical Revasc for LMCA CLASS IA

7
Historical Recommendation: Unprotected Left Main PCI In patients eligible for CABG Class IIb C in ESC guideline (2005) Class III in ACC/AHA/SCAI guideline (2006)
 Class III in ACC/AHA/SCAI guideline (2006)")
8
MAIN COMPARE Outcomes Propensity Match Model for 396 Pairs Seung K et al. N Engl J Med 2008;358:1781-1792 Mortality: p=0.26MACCE: p=0.16TVR: p<0.001

12
Palmerini, et al. SICI-GISE Survey, Eur Heart J 2009 At risk At risk Ostial or midshaft 334 264 199 128 103 Ostial or midshaft 334 264 199 128 103 Bifurcat ion one stent 456 364 274 186 140 Bifurcation two stents 317 229 167 123 103 100% 75% 50% 25% 0% 0% Log-rank P = 0.00001 00.5 11.52 Years Survival free from TLR (%) No differences in overall and cardiac mortality and MI between the three groups DES for Ostial (n=334) vs distal (n=777) left main lesions One vs two stents 73% 87% 92% Independent predictors of 2-years MACE (Covariates-adjusted) HR (95% CI)P Bifurcation with 2 stents1.92 (1.30-2.84).001 Age1.02 (1.01-1.04).001 Diabetes1.53 (1.13-2.07).007 Renal dysfuntion2.25 (1.27-3.98).005 LV Ejection fraction0.98 (0.97-0.99).002 Ostial or midshaft Bifurcations, one stent Bifurcations, two stents
 No differences in overall and cardiac mortality and MI between the three groups DES for Ostial (n=334) vs distal (n=777) left main lesions One vs two stents 73% 87% 92% Independent predictors of 2-years MACE (Covariates-adjusted) HR (95% CI)P Bifurcation with 2 stents1.92 ( ).001 Age1.02 ( ).001 Diabetes1.53 ( ).007 Renal dysfuntion2.25 ( ).005 LV Ejection fraction0.98 ( ).002 Ostial or midshaft Bifurcations, one stent Bifurcations, two stents.")
13
Contemporary Trials of LM PCI vs CABG Clinical Equipoise and Reassessment of Guidelines Trial * NDeathMIStrokeRevasc Sanmartin 2007 341 ND CABG better MAIN-COMPARE 2008 1102 n/a LEMANS 2008 105 Palmerini 2006 311 Chieffo 2006 249 PCI better Lee 2006 173 ND Makikallio 2008 287 ND Brener 2008 287 n/a White 2008 343 SYNTAX 2008 705 ND PCI better CABG better * Studies with >100 patients per arm reported 2000-2008 ND=no difference; n/a=not available/not reported Suggested IIa for ostial/shaft LM and IIb for distal LM 1-2 V CAD

14
New classes of recommendations for Left Main PCI 2009 “The best case for PCI as an alternative to CABG for left main is in ostial and mid- body lesions without additional MVD” IIb Level of Evidence: B “PCI of the left main coronary artery with stents as an alternative to CABG may be considered in patients with anatomic conditions that are associated with a low risk of PCI procedural complications and clinical conditions that predict an increased risk of adverse surgical outcomes”.

15
Indications for CABG vs PCI in stable patients with lesions suitable for both procedures and low predicted surgical mortality Subset of CAD by anatomyFavours CABGFavours PCI Left main (isolated or 1VD, ostium/shaft)I AIIa B Left main (isolated or 1VD, bifurcation)I AIIb B Left main + 2VD or 3VD, SYNTAX score ≤ 32I AIIb B Left main + 2VD or 3VD, SYNTAX score ≥ 33I AIII B ESC guidelines 2010
I AIIa B Left main (isolated or 1VD, bifurcation)I AIIb B Left main + 2VD or 3VD, SYNTAX score ≤ 32I AIIb B Left main + 2VD or 3VD, SYNTAX score ≥ 33I AIII B ESC guidelines 2010")
16
Death, MI or Stroke Ischemia-Driven TVR Safety and efficacy outcomes Park et al NEJM April 4, 2011

17
CABG to improve survival is recommended for patients with significant (≥50% diameter stenosis) left main CAD. PCI to improve survival is reasonable as an alternative to CABG in selected stable patients with significant (≥50% diameter stenosis) unprotected left main CAD with: 1) anatomic conditions associated with a low risk of PCI procedural complications and a high likelihood of a good long-term outcome (e.g., a low SYNTAX score [≤22], ostial or trunk left main CAD); and 2) clinical characteristics that predict a significantly increased risk of adverse surgical outcomes (e.g., STS- predicted risk of operative mortality ≥5%). Revascularization to Improve Survival: Left Main CAD Revascularization I IIaIIbIII I IIaIIbIII 2011 Guideline Update
 unprotected left main CAD with: 1) anatomic conditions associated with a low risk of PCI procedural complications and a high likelihood of a good long-term outcome (e.g., a low SYNTAX score [≤22], ostial or trunk left main CAD); and 2) clinical characteristics that predict a significantly increased risk of adverse surgical outcomes (e.g., STS- predicted risk of operative mortality ≥5%). Revascularization to Improve Survival: Left Main CAD Revascularization I IIaIIbIII I IIaIIbIII 2011 Guideline Update.")
18
PCI to improve survival may be reasonable as an alternative to CABG in selected stable patients with significant (≥50% diameter stenosis) unprotected left main CAD with: 1) anatomic conditions associated with a low to intermediate risk of PCI procedural complications and an intermediate to high likelihood of good long-term outcome (e.g., low-intermediate SYNTAX score of 2%). Revascularization to Improve Survival: Left Main CAD Revascularization (cont.) I IIaIIbIII
 I IIaIIbIII.")
19
PCI to improve survival is reasonable in patients with UA/NSTEMI when an unprotected left main coronary artery is the culprit lesion and the patient is not a candidate for CABG. PCI to improve survival is reasonable in patients with acute STEMI when an unprotected left main coronary artery is the culprit lesion, distal coronary flow is TIMI (Thrombolysis In Myocardial Infarction) grade <3, and PCI can be performed more rapidly and safely than CABG. Revascularization to Improve Survival: Left Main CAD Revascularization (cont.) I IIaIIbIII I IIaIIbIII
 grade <3, and PCI can be performed more rapidly and safely than CABG. Revascularization to Improve Survival: Left Main CAD Revascularization (cont.) I IIaIIbIII I IIaIIbIII.")
20
PCI to improve survival should not be performed in stable patients with significant (≥50% diameter stenosis) unprotected left main CAD who have unfavorable anatomy for PCI and who are good candidates for CABG. Revascularization to Improve Survival: Left Main CAD Revascularization (cont.) I IIaIIbIII Harm
 I IIaIIbIII Harm.")
21
Why do we need risk stratification in complex coronary artery disease? Diagnostic and prognostic models: Drive informed clinical decisions because they allow the selection of the most appropriate strategy of treatment based on the patient's individual characteristics Help patients and their families to get a better understanding of issues relevant to treatment strategies and subsequent risks as part of the process to obtain informed consent Assist quality-of-care monitoring and facilitate a fair comparison of procedures performed in different clinical scenarios Are valuable aids for stratifying patients by disease severity in clinical trials Capodanno et al, Am Heart J 2011;161:462-70

22
Prognostic Models in Left Main Disease Clinical stand-alone tools EuroSCORE ACEF score Angiographic stand-alone tools SYNTAX score Combined (angiographic+clinical) tools Global Risk Classification (GRC) Clinical SYNTAX score (CSS) New Risk Classification (NERS)
 tools Global Risk Classification (GRC) Clinical SYNTAX score (CSS) New Risk Classification (NERS)")
24
The Global Risk Classification (GRC) Cardiac death free survival (%) 100 90 80 70 60 Time (months) 0 12 24 SYNTAX score 96.1% 94.6% 78.1% LOW MIDDLE HIGH P = 0.004* Cardiac death free survival (%) 100 90 80 70 60 Time (months) 0 12 24 GRC 98.4% 84.0% 68.6% LOW MIDDLE HIGH P < 0.001* * log rank test; n = 255 LM patients undergoing PCI LLI LLI IIH 0-2 3-6 > 6 < 1919-27> 27 SYNTAX score EuroSCORE Capodanno, Tamburino, et al. Am Heart J 2010:159:103-9

25
Left Main PCI: Patient Selection and Technique Patient Selection IVUS and FFR Intermediate LMCA stenosis cases Procedure Technique (Cases) Surveillance: Follow-up
 Surveillance: Follow-up")
26
Intermediate LMCA Stenosis Correlation of FFR and Angiographic Assessment Hamilos M: Circulation 2009;120 23% of patients with <50% diameter stenosis angiographically had a hemodynamically significant lesion by FFR

27
Hamilos M et al. Circulation 2009;120:1505-1512 LMCA FFR Survival Estimates and Strategy Patients with FFR > 0.8 have an excellent prognosis with medical management FFR wire placement in less diseased vessel (LAD vs Cx) Ostial lesions require guide disengagement High doses of intravenous adenosine must be used to ensure accurate FFR
 Ostial lesions require guide disengagement High doses of intravenous adenosine must be used to ensure accurate FFR.")
28
Kang SJ et al JACC Cardiovasc Interv.Kang SJ et al JACC Cardiovasc Interv. 2011 Nov;4(11):1168 Intermediate LMCA Stenosis IVUS MLA >7.5mm2 safe to defer revascularization. Fassa JACC;45;204 2005 MLA <6.0mm2 correlated with angiographically significant stenosis Sano Am Heart J. 2007 Nov;154(5):983-8. 2007 MLA <4.8 mm2 predicted FFR<0.80 MLA <4.0 mm2 predicted FFR<0.75 Kang et al JACC CV Interv 2011 Currently, in patients with angiographically intermediate disease, IVUS MLD < 2.8 mm or MLA < 6 mm2 suggests a physiologically significant lesion and may benefit from revasc. IVUS does provide procedural assistance in LMCA PCI Correlation of FFR and IVUS
:1168 Intermediate LMCA Stenosis IVUS MLA >7.5mm2 safe to defer revascularization. Fassa JACC;45; MLA <6.0mm2 correlated with angiographically significant stenosis Sano Am Heart J Nov;154(5): MLA <4.8 mm2 predicted FFR<0.80 MLA <4.0 mm2 predicted FFR<0.75 Kang et al JACC CV Interv 2011 Currently, in patients with angiographically intermediate disease, IVUS MLD < 2.8 mm or MLA < 6 mm2 suggests a physiologically significant lesion and may benefit from revasc. IVUS does provide procedural assistance in LMCA PCI Correlation of FFR and IVUS.")
32
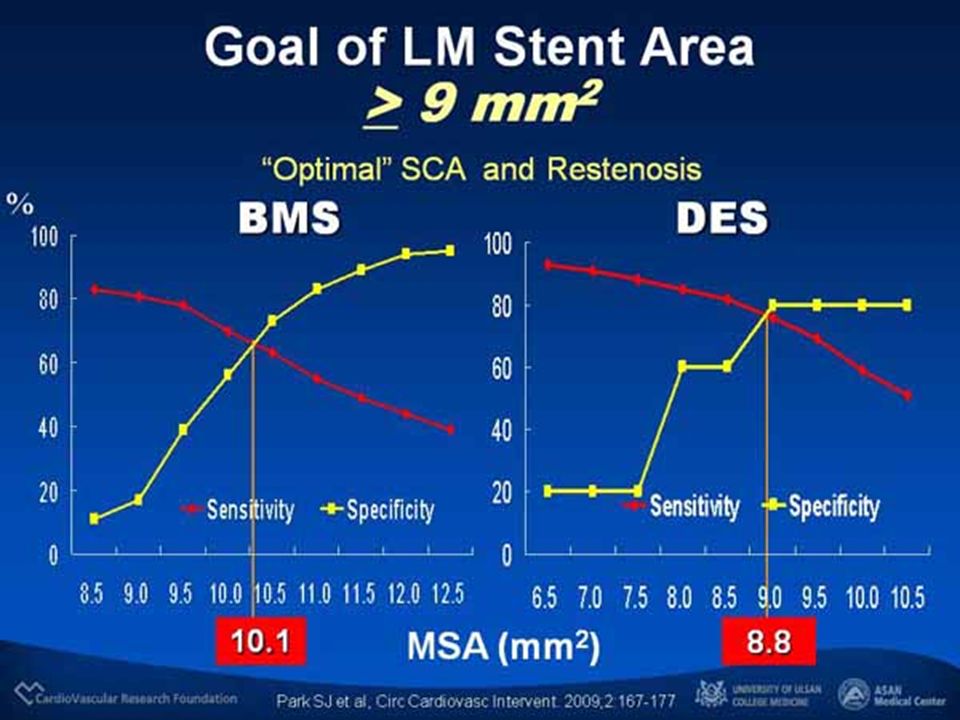
LMCA Stenting 1) Optimal Lesion preparation using a CB or Rotablation 2)IVUS Guidance : Pre. : For extent of disease and Calcification Post.: For Optimal stent deployment 3) Post Dilatation using a Non Compliant balloon 4) FFR will Likely play a bigger Role !
 Post Dilatation using a Non Compliant balloon 4) FFR will Likely play a bigger Role !.")
34
Ostial Left Main Lesion Do NOT rely on the Spider View LAO-cranio viewAP – RAO view

35
Mid-shaft Left Main Lesion AP – caudal view

36
« T » technique 90° 90°

37
4.0 mm DES 3.5mm DES Final kissing

38
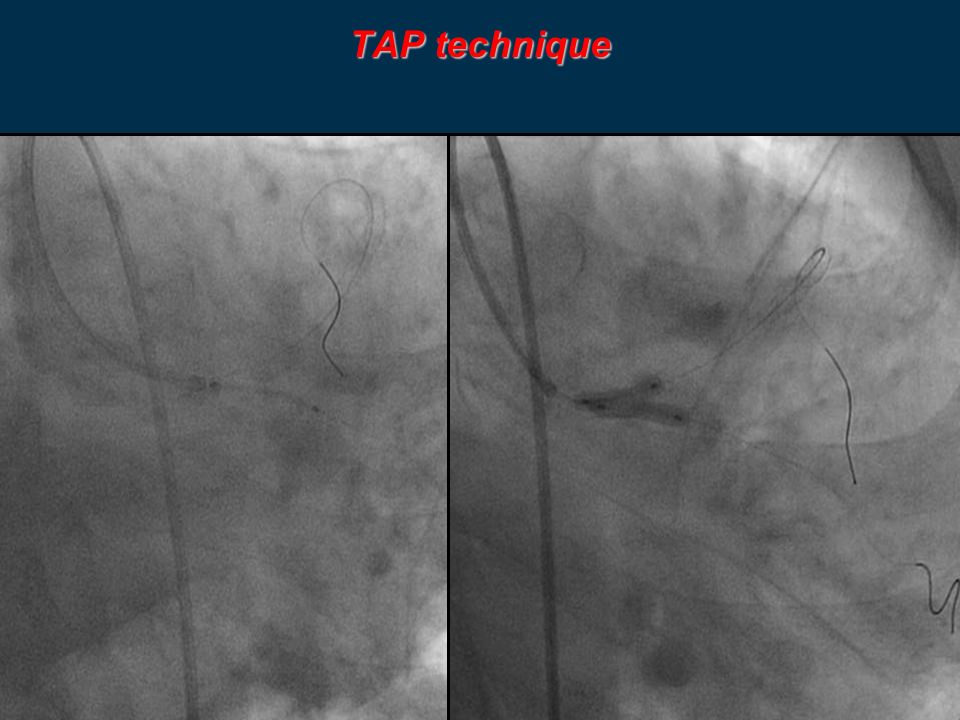
TAP technique

39
4.5x16mm DES

40
TAP technique

43
Final result

44
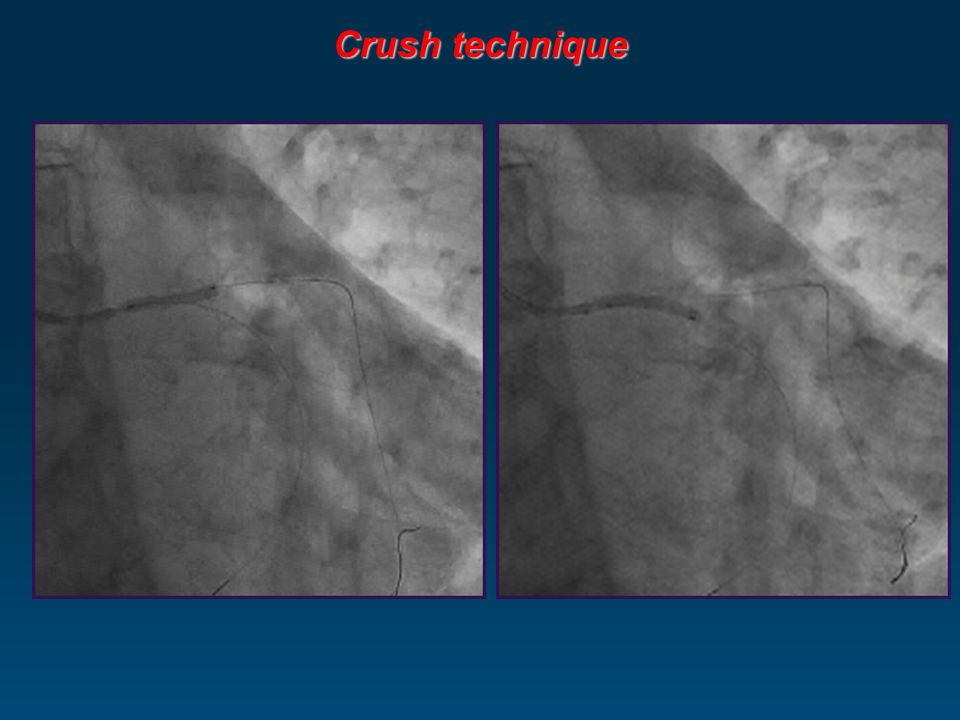
Crush technique

50
Final kissing Final result

51
Kissing stent technique

52
Kissing stent with 2 Taxus stents: 3.5x16 & 3.5x12mm Kissing stent technique ( SKS )
")
53
Kissing stent technique Final result

54
Ostial LCx

63
LMCA Trifurcation Disease

65
LMCA PCI Cases

66
Surveillance: Follow-up Non bifurcation elective LMCA PCI with DES: Risk of ST and restenosis is very low Chieffo et al Circ 2007;116:158 All DES elective PCI UPLMCA with normal LV function very low Stent Thrombosis (<1% incidence definite or probable ST over 3-5 years) Lee CCI 77:945-51,2011, Chieffo EHJ;29.2108, 2008, Meliga (DELFT Reg)JACC ;51:2212, 2008. Clinical Restenosis (TLR) for DES PCI UPLMCA is quite low 6-10%) in most Registries, no SCD signal Current guidelines support long-term aspirin treatment and at least 1 year of thienopyridine therapy in post-PCI patients (Class I, Level of Evidence: B) however this is not specific for UPLM coronary stenting. Given low risk of very late stent thrombosis in UPLM, risks and benefits of greater than 1 year of dual antiplatelet therapy may need to be tailored to patient specific co-morbidities. Stent Thrombosis Restenosis (SCD)
 for DES PCI UPLMCA is quite low 6-10%) in most Registries, no SCD signal Current guidelines support long-term aspirin treatment and at least 1 year of thienopyridine therapy in post-PCI patients (Class I, Level of Evidence: B) however this is not specific for UPLM coronary stenting. Given low risk of very late stent thrombosis in UPLM, risks and benefits of greater than 1 year of dual antiplatelet therapy may need to be tailored to patient specific co-morbidities. Stent Thrombosis Restenosis (SCD).")
Similar presentations




























>")

 vs. percutaneous coronary intervention.>")

