Download presentation
Presentation is loading. Please wait.

1
Prescribing in cardiovascular disease By Jole Hannan Medicines Optimisation Pharmacist

2
Tips StatinsBeta-blockers ACE inhibitors

3
What patients are confronted with…

4
Simple messages for statins

5
Don’t measure cholesterol levels for primary prevention patients Use simvastatin 40mg primary prevention and consider it at 12 months post MI Higher intensity statin of choice is Atorvastatin 80mg At 12 months post MI review statin requirement Amlodipine, diltiazem, verapamil and amiodarone increase effect of Simvastatin – so reduce the dose. If Patient has a reaction to a statin record what it is recent study shows break treatment and retry Ask a patient if they have had a bad reaction if cholesterol control is poor – often adherence is main reason for poor results

6
Don’t measure cholesterol levels for primary prevention patients (no targets or levels recommended) Link to primary prevention – simple step at initiation which will save any reviewer time and effort. Simvastatin 40mg and Atorvastatin 10mg are now low cost statins at present £1.16/£1.17 for 28 Amlodipine, Diltiazem, Verapamil and Amiodarone increase effect of Simvastatin – so reduce the dose to Simvastatin 20mg or use Atorvastatin 10mg. Remember statin are not a magic bullet …

7
Primary prevention patients (20% risk) If 100 patients take a statin over 10 years what is the outcome??
 If 100 patients take a statin over 10 years what is the outcome")
8
5 patients “saved” by taking a statin Red patients will have CV event regardless of statin use Estimated 18, 000 patients on simvastatin last year = 900 saved

9
Remember - not a ‘magic bullet’ Remind patients : If you are being treated with statins, to keep your cholesterol levels at a healthy level it is likely you will also need to make lifestyle changes such as: eating a healthy diet low in saturated fathealthy diet taking regular exerciseregular exercise quitting smoking if you smoke quitting smoking moderating your consumption of alcoholconsumption of alcohol Optimal treatment of other conditions

10
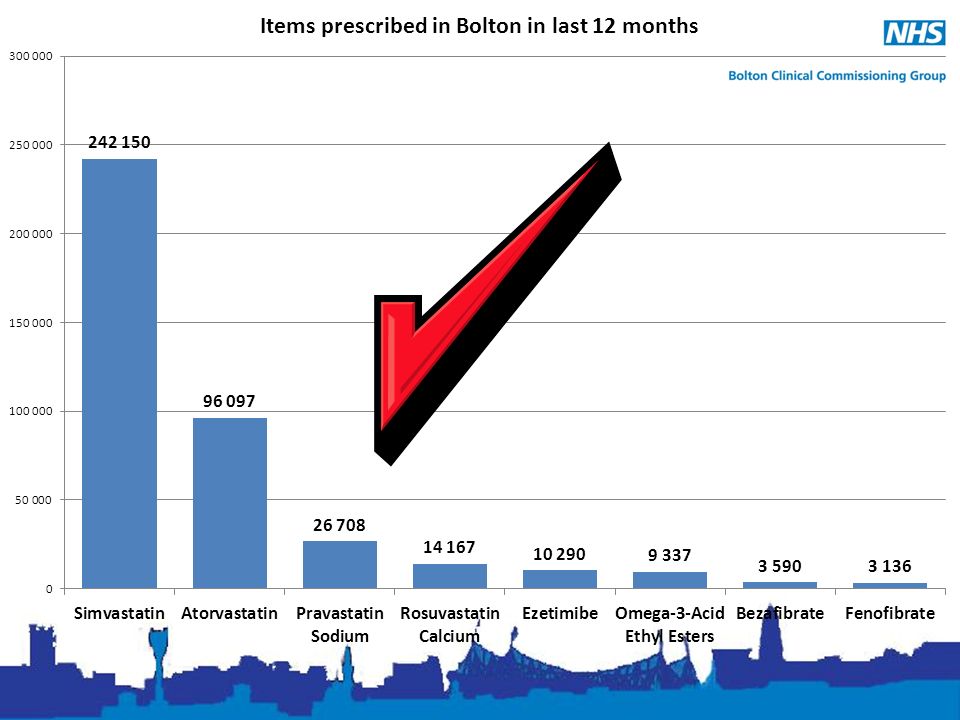
Higher intensity statin of choice is Atorvastatin (80mg) At 12 months post MI review statin requirement – “TC: HDL ratio <3.5” = reduce statin Rosuvastatin use = 4 th line option – 1 st Simvastatin 2 nd Atorvastatin 3 rd Pravastatin 4 th Rosuvastatin Rosuvastatin 40mg £390 per patient per year Atorvastatin 80mg £39 per patient per year Ezetimibe/Omacor use = lipid clinic only
 At 12 months post MI review statin requirement – TC: HDL ratio <3.5 = reduce statin Rosuvastatin use = 4 th line option – 1 st Simvastatin 2 nd Atorvastatin 3 rd Pravastatin 4 th Rosuvastatin Rosuvastatin 40mg £390 per patient per year Atorvastatin 80mg £39 per patient per year Ezetimibe/Omacor use = lipid clinic only")
12
£800,000

13
Statin intolerance Is it intolerance to the statin? Record the intolerance and severity in notes – if entered as an allergy this can have significant future effects Recent studies show reduced dose or alternative statins can be tolerated in majority of cases Some studies do show atorvastatin/rosuva can be used on alternate days – but very small studies If non severe intolerance consider reducing dose or use next line statin

14
NICE CVD information Start treatment with a statin as soon as possible No target cholesterol levels are recommended for primary prevention in people without Type 2 diabetes. Target cholesterol levels are recommended for secondary prevention and for people with Type 2 diabetes: – If total cholesterol does not fall below 4 mmol/L or low- density lipoprotein cholesterol does not fall below 2 mmol/L, consider higher-intensity statin therapy.

15
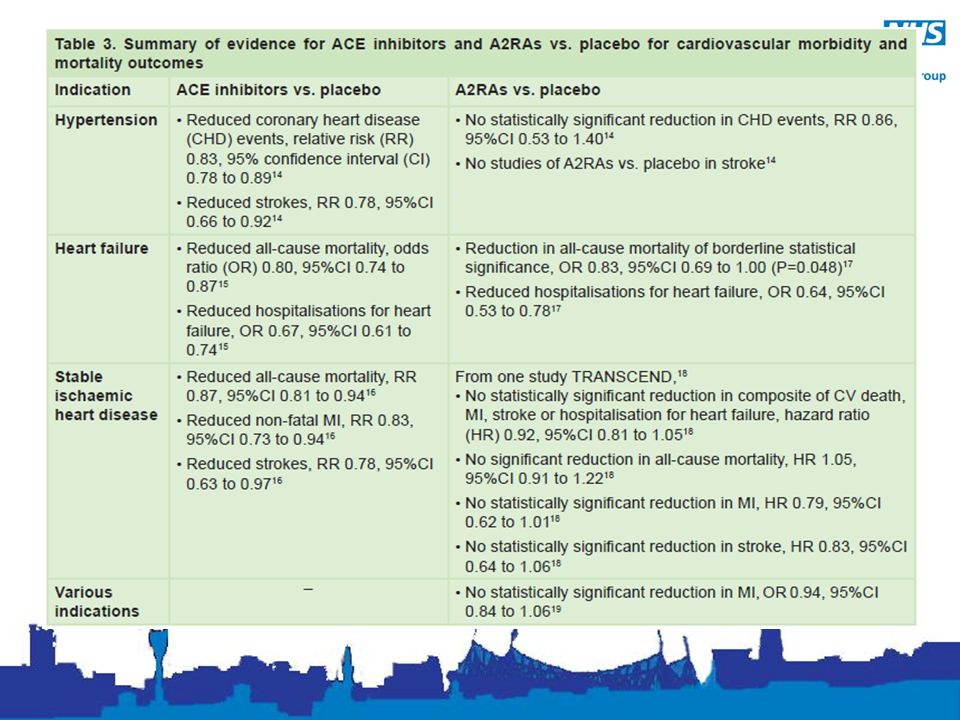
Renin-angiotensin system BNF - great source of information – Heart failure – covered in workshops Heart failure – Angiotensin-converting enzyme inhibitors - ACEs Angiotensin-converting enzyme inhibitors – Angiotensin-II receptor antagonists – ARBS/A2RAs Angiotensin-II receptor antagonists – Renin inhibitors - Aliskiren Renin inhibitors

16
ACE or ARBs NICE recommended ACE is 1 st line in – Diabetes mellitus – Chronic kidney disease (CKD) – Chronic heart failure – Post-myocardial infarction (post-MI) Hypertension – either low cost ARB or ACE 1 st line
 – Chronic heart failure – Post-myocardial infarction (post-MI) Hypertension – either low cost ARB or ACE 1 st line")
18
Which ACE/ARB to chose? Low cost ARBs are – Candesartan – Losartan, – Valsartan Capsules – Irbesartan High cost ARB are – Telmisartan – Olmesartan – Branded items – Valsartan TABLETS – Combination products ACE – GM Formulary Ramipril capsules Lisinopril tablets ACEs higher cost Branded Perindopril arginine Trandolapril 1 & 4mg Imidapril Combination products

19
ACE ARB testing Measure serum potassium concentrations, estimate the GFR before starting – Reminder - eGFR is an estimate – care in patients that are not “average” Repeat these measurements between 1 and 2 weeks after starting ACE inhibitor/ARB therapy and after each dose increase

20
When to stop an ACE/ARB Serum potassium concentration rises to 6.0 mmol/litre or more Do not modify the ACE/ARB dose if the change in eGFR is less than 25% or the change in plasma creatinine is less than 30% – investigate other causes such as volume depletion or concurrent medication (for example, NSAIDs) – if no other cause found consider Reduce the dose to a previously tolerated lower dose, and Or stop the ACE inhibitor/ARB therapy And add an alternative antihypertensive medication if required
 – if no other cause found consider Reduce the dose to a previously tolerated lower dose, and Or stop the ACE inhibitor/ARB therapy And add an alternative antihypertensive medication if required")
21
RAS Drugs like the statins – costs have reduced but still ARBs are more expensive than ACEI are Main concerns for optimal treatment – Titrate up the dose – Annual monitoring

22
Aliskiren Contraindicated in – Diabetics using ACE/ARB – eGFR below 60 and using ACE/ARB in all other patients, combination treatment with an ACE inhibitor or an angiotensin-II receptor antagonist is not recommended Small numbers of patients – review anyone taking longer than 12 months – Meds Opt have reviewed most patients and given recommendations to practices

23
Beta Blockers Link to indication – HF, CHD, migraine, anxiety, glaucoma, thyroid When to change Beta blockers – Review compelling indication and BP control – If removing reduce dose slowly Review adherence – irregular use can be as problematic as no use

24
Think Asthma COPD When to change a Beta blocker Specials (liquids) – alternatives from Meds Opt Team Link to indication (HF, CHD, migraine, anxiety, glaucoma, thyroid) so at med review which one are you looking at Risk of overdose*
 – alternatives from Meds Opt Team Link to indication (HF, CHD, migraine, anxiety, glaucoma, thyroid) so at med review which one are you looking at Risk of overdose*")
25
Which Beta Blocker Very simple choice in most cases Although review all low dose patients to ensure dose titration has been attempted Nebivolol – dose review – 2.5mg cost £70 per month – 5mg cost £2 per month

26
Medication review Key message – Medication review Why is patient on the medication? Are they taking it? – If you prescribe monthly have they order 12 Rxs in last year? Do their results look like they are taking it? Do they know why they are taking the medication? Are they having and side effects, problems, or is there anything that could be improved? – Statin – forget to take, Beta blocker – cold feet, ACE/ARB = cough Are they on a register (NHSE is watching!)
.")
27
Thank you Information on any aspect of prescribing please contact Medicines Optimisation on 01204 46 21 25 Available to practice staff and patients

Similar presentations




 www.ahrq.gov.>")














