Download presentation
Presentation is loading. Please wait.

1
RESPIRATORY SYSTEM DRUGS
Drugs for Cough and Bronchial Asthma

2
DRUGS FOR COUGH Cough is a protective reflex (due to stimulation of mechano- or chemoreceptors in throat), its purpose being expulsion of respiratory secretions or foreign particles from air passages. is caused by a respiratory tract infection, choking, smoking, air pollution, chronic bronchitis, lung tumors, heart failure and drugs (ACE inhibitors). Cough may be: non-productive (dry) productive (when sputum is coughed up) Dry (non-productive) cough should be suppressed. Productive cough serves to drain the airway, its suppression is not desirable, may even be harmful.
, its purpose being expulsion of respiratory secretions or foreign particles from air passages. is caused by a respiratory tract infection, choking, smoking, air pollution, chronic bronchitis, lung tumors, heart failure and drugs (ACE inhibitors). Cough may be: non-productive (dry) productive (when sputum is coughed up) Dry (non-productive) cough should be suppressed. Productive cough serves to drain the airway, its suppression is not desirable, may even be harmful.")
3
Specific remedies for cough

4
Symptomatic (nonspecific) therapy
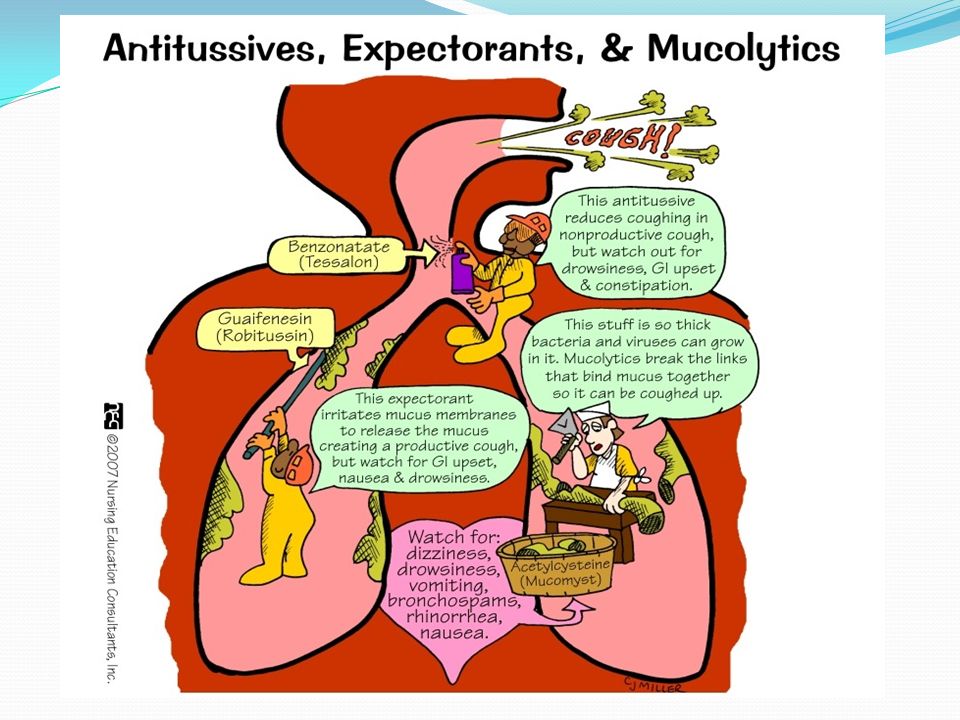
1) Antitussives (Cough centre suppressants) Central (CNS) acting: Opioids: Codeine, Ethylmorphine, Pholcodeine. Nonopioids: Noscapine, Dextromethorphan, Chlophedianol. Peripherally acting: Prenoxdiazine. 2) Expectorants (Mucokinetics) - Bronchial secretion enhancers: Sodium or Potassium citrate, Potassium iodide, Guaiphenesin (Glyceryl guaiacolate), Vasaka, Ammonium chloride. 3) Mucolytics: Bromhexine, Ambroxol, Acetyl cysteine, Carbocisteine 4) Additional therapy: Antihistamines: Chlorpheniramine, Diphenhydramine,Promethazine. Bronchodilators: Salbutamol, Terbutalin Pharyngeal demulcents: Lozenges, cough drops, drugs containing syrup, glycerine, liquorice
 Antitussives (Cough centre suppressants) Central (CNS) acting: Opioids: Codeine, Ethylmorphine, Pholcodeine. Nonopioids: Noscapine, Dextromethorphan, Chlophedianol. Peripherally acting: Prenoxdiazine. 2) Expectorants (Mucokinetics) - Bronchial secretion enhancers: Sodium or Potassium citrate, Potassium iodide, Guaiphenesin (Glyceryl guaiacolate), Vasaka, Ammonium chloride. 3) Mucolytics: Bromhexine, Ambroxol, Acetyl cysteine, Carbocisteine. 4) Additional therapy: Antihistamines: Chlorpheniramine, Diphenhydramine,Promethazine. Bronchodilators: Salbutamol, Terbutalin. Pharyngeal demulcents: Lozenges, cough drops, drugs containing syrup, glycerine, liquorice.")
8
The treatment of a cough
Half of cases go away without treatment in 10 days and 90% in 25 days. The American Academy of Pediatrics do not recommend the use of cough medicines for treating cough symptoms in children. There is tentative evidence that the use of honey is better than no treatment in decreasing coughing. Cough medicines may be tried for a chronic cough. The complications of coughing: Acute complications - cough syncope (fainting spells due to decreased blood flow to the brain when coughs are prolonged and forceful), insomnia, cough-induced vomiting, spontaneous pneumothorax (although this still remains to be proven), subconjunctival hemorrhage or "red eye", coughing defecation and in women with a prolapsed uterus, cough urination. Chronic complications - abdominal or pelvic hernias, fatigue fractures of lower ribs and costochondritis.
, insomnia, cough-induced vomiting, spontaneous pneumothorax (although this still remains to be proven), subconjunctival hemorrhage or red eye , coughing defecation and in women with a prolapsed uterus, cough urination. Chronic complications - abdominal or pelvic hernias, fatigue fractures of lower ribs and costochondritis.")
9
DEMULCENTS AND EXPECTORANTS
Pharyngeal demulcents sooth the throat and reduce afferent impulses from the inflamed/irritated pharyngeal mucosa, thus provide symptomatic relief in dry cough arising from throat. Expectorants (Mucokinetics) are drugs believed to increase bronchial secretion, facilitating its removal by coughing.
 are drugs believed to increase bronchial secretion, facilitating its removal by coughing.")
10
Expectorants (Mucokinetics)
Sodium and potassium citrate are considered to increase bronchial secretion by salt action. Potassium iodide is secreted by bronchial glands and can irritate the airway mucosa. Prolonged use can affect thyroid function and produce iodism. It is not used now. Guaiphenesin, vasaka, tolu balsum are plant products which are supposed to enhance bronchial secretion and mucociliary function while being secreted by tracheobronchial glands. Ammonium salts are nauseating—reflexly increase respiratory secretions. The USA has stopped marketing of all expectorants, except guaiphenesin. Steam inhalation and proper hydration may be more helpful in clearing airway mucus.

11
Mucolytics Bromhexine
A derivative of the alkaloid vasicine obtained from Adhatoda vasica (Vasaka), is a potent mucolytic and mucokinetic, capable of inducing thin copious bronchial secretion. It depolymerises mucopolysaccharides directly as well as by liberating lysosomal enzymes—network of fibres in tenacious sputum is broken. Side effects are rhinorrhoea and lacrimation, nausea, gastric irritation, hypersensitivity. Ambroxol A metabolite of bromhexine having similar mucolytic action, uses and side effects. Acetylcysteine It opens disulfide bonds in mucoproteins present in sputum—makes it less viscid. It has to be administered directly into the respiratory tract. Carbocisteine It liquefies viscid sputum in the same way as acetylcysteine . It is administered orally. It may break gastric mucosal barrier; is contraindicated in peptic ulcer patients. Side effects are gastric discomfort and rashes.
, is a potent mucolytic and mucokinetic, capable of inducing thin copious bronchial secretion. It depolymerises mucopolysaccharides directly as well as by liberating lysosomal enzymes—network of fibres in tenacious sputum is broken. Side effects are rhinorrhoea and lacrimation, nausea, gastric irritation, hypersensitivity. Ambroxol. A metabolite of bromhexine having similar mucolytic action, uses and side effects. Acetylcysteine. It opens disulfide bonds in mucoproteins present in sputum—makes it less viscid. It has to be administered directly into the respiratory tract. Carbocisteine. It liquefies viscid sputum in the same way as acetylcysteine . It is administered orally. It may break gastric mucosal barrier; is contraindicated in peptic ulcer patients. Side effects are gastric discomfort and rashes.")
12
ANTITUSSIVES These are drugs that:
-act in the CNS to raise the threshold of cough centre -act peripherally in the respiratory tract to reduce tussal impulses, or both these actions. Antitussives should be used only for dry nonproductive cough or if cough is unduly tiring, disturbs sleep or is hazardous (hernia, piles, cardiac disease, ocular surgery).
.")
14
Opioids Codeine = methylmorphine
An opium alkaloid, qualitatively similar to and less potent than morphine, but is more selective for cough centre. Codeine suppresses cough for about 6 hours. ADR: Abuse liability; constipation; respiratory depression; drowsiness. Driving may be impaired. Like morphine, it is contraindicated in asthmatics and should be avoided in children. Ethylmorphine It is closely related to codeine has antitussive, respiratory depressant properties like it, but is believed to be less constipating. Pholcodeine It has practically no analgesic or addicting property, but is similar in efficacy as antitussive to codeine and is longer acting—acts for 12 hours.

15
Nonopioids Noscapine (Narcotine)
It depresses cough but has no narcotic, analgesic or dependence inducing properties. Especially useful in spasmodic cough. ADR: Headache, nausea. It can release histamine and produce bronchoconstriction in asthmatics. Dextromethorphan A central NMDA (N-methyl D-aspartate) receptor antagonist; The antitussive action of dextromethorphan has been rated equivalent to codeine. It is a common ingredient of many antitussive combinations. ADR: Dizziness, nausea, drowsiness; at high doses hallucinations and ataxia may occur. Chlophedianol It is a centrally acting antitussive with slow onset and longer duration of action. ADR: Dryness of mouth, vertigo, irritability.
 receptor antagonist; The antitussive action of dextromethorphan has been rated equivalent to codeine. It is a common ingredient of many antitussive combinations. ADR: Dizziness, nausea, drowsiness; at high doses hallucinations and ataxia may occur. Chlophedianol. It is a centrally acting antitussive with slow onset and longer duration of action. ADR: Dryness of mouth, vertigo, irritability.")
16
Peripherally acting antitussives
Prenoxdiazine (marketed as Libexin) In contrast to other antitussives, it acts peripherally: Desensitizes the pulmonary stretch receptors and reduces tussle impulses originating in the lungs. It is indicated in cough of bronchial origin. Not respiration depression. Does not cause addiction. Efficacy is not impressive.
 In contrast to other antitussives, it acts peripherally: Desensitizes the pulmonary stretch receptors and reduces tussle impulses originating in the lungs. It is indicated in cough of bronchial origin. Not respiration depression. Does not cause addiction. Efficacy is not impressive.")
17
Bronchial asthma is characterised by hyperresponsiveness of tracheobronchial smooth muscle, resulting in: narrowing of air tubes increased secretion, mucosal edema mucus plugging. Symptoms include: dyspnoea, wheezing, cough and may be limitation of activity.

18
Bronchial asthma Mast cells and inflammatory cells (recruited as a result of the initial reaction) produce a multitude of mediators by the following processes: Release of mediators stored in granules (immediate): histamine, protease enzymes,TNFα. Release of phospholipids from cell membrane followed by mediator synthesis (within minutes): PGs, LTs, PAF. Activation of genes followed by protein synthesis (over hours): Interleukins, TNFα. These mediators together constrict bronchial smooth muscle, cause mucosal edema, hyperemia and produce viscid secretions Reversible airway obstruction Bronchial smooth muscle hypertrophy Damage of bronchial epithelium Airway remodeling Progressive aggravation of the disease.
 produce a multitude of mediators by the following processes: Release of mediators stored in granules (immediate): histamine, protease enzymes,TNFα. Release of phospholipids from cell membrane followed by mediator synthesis (within minutes): PGs, LTs, PAF. Activation of genes followed by protein synthesis (over hours): Interleukins, TNFα. These mediators together constrict bronchial smooth muscle, cause mucosal edema, hyperemia and produce viscid secretions. Reversible airway obstruction. Bronchial smooth muscle hypertrophy. Damage of bronchial epithelium. Airway remodeling. Progressive aggravation of the disease.")
19
Chronic obstructive pulmonary disease

20
Chronic obstructive pulmonary disease (COPD)
is also an inflammatory disease of the lungs characterized by: Progressive emphysema (alveolar destruction) Bronchiolar fibrosis / chronic bronchitis . Loss of bronchiolar elasticity leads to closure of smaller air tubes during expiration. The airway obstruction is accentuated during exercise causing shortness of breath. Bronchodilators prevent closure of peripheral air tubes during expiration and afford symptomatic relief in COPD patients, but improvement is generally <15%. An increasing part of airway obstruction is irreversible.
 Bronchiolar fibrosis / chronic bronchitis . Loss of bronchiolar elasticity leads to closure of smaller air tubes during expiration. The airway obstruction is accentuated during exercise causing shortness of breath. Bronchodilators prevent closure of peripheral air tubes during expiration and afford symptomatic relief in COPD patients, but improvement is generally <15%. An increasing part of airway obstruction is irreversible.")
23
CLASSIFICATION I. Bronchodilators
β2 Adrenomimetics: Salbutamol, Terbutaline, Salmeterol, Formoterol. Methylxanthines: Theophylline, Aminophylline (85% theophylline). Anticholinergics: Ipratropium bromide, Tiotropium bromide. II. Leukotriene antagonists Montelukast, Zafirlukast. III. Mast cell stabilizers Sodium cromoglycate, Ketotifen. IV. Corticosteroids Inhalational: Beclomethasone, Budesonide, Fluticasone. Systemic: Hydrocortisone, Prednisolone and others. V. Anti-IgE antibody Omalizumab
. Anticholinergics: Ipratropium bromide, Tiotropium bromide. II. Leukotriene antagonists. Montelukast, Zafirlukast. III. Mast cell stabilizers. Sodium cromoglycate, Ketotifen. IV. Corticosteroids. Inhalational: Beclomethasone, Budesonide, Fluticasone. Systemic: Hydrocortisone, Prednisolone and others. V. Anti-IgE antibody. Omalizumab.")
24
β2 Adrenomimetics Adrenergic drugs cause bronchodilatation through β2 receptor stimulation → relaxation. Adrenergic drugs are the mainstay of treatment of reversible airway obstruction. They are the most effective and fastest acting bronchodilators when inhaled. Though adrenaline (β1+β2+α receptor agonist) and isoprenaline (β1+β2 agonist) are effective bronchodilators, there are the selective β2 agonists that are now used in asthma to minimize cardiac side effects.
 and isoprenaline (β1+β2 agonist) are effective bronchodilators, there are the selective β2 agonists that are now used in asthma to minimize cardiac side effects.")
25
β2 STIMULANTS Short acting (4–6 hours) : Salbutamol Terbutaline
Ritodrine Long lasting (12 hours): Salmeterol Formoterol Clenbuterol the relief of bronchospasm in asthma to relax the uterine smooth muscle to delay premature labor. for prevention of asthma symptoms not for use in relieving an asthma attack (not be used to treat acute symptoms) should be used with a corticosteroid
: Salmeterol. Formoterol. Clenbuterol. the relief of bronchospasm in asthma. to relax the uterine smooth muscle to delay premature labor. for prevention of asthma symptoms. not for use in relieving an asthma attack (not be used to treat acute symptoms) should be used with a corticosteroid.")
26
β2 STIMULANTS Side effects Dizziness Headaches Tachycardia Arrhythmia
Muscle cramps Paradoxical bronchospasm! Hypotension and collapse

27
β2 STIMULANTS COPD Long-acting β2 agonists are superior to short-acting ones, and equivalent to inhaled anticholinergics in COPD. They reduce breathlessness by preventing expiratory closure of peripheral airways and abolishing the reversible component of airway obstruction.

28
METHYL XANTHINES Theophylline and its compounds have been extensively used in asthma, but are not considered first line drugs any more. They are used more often in COPD. Theophylline is one of the xanthine alkaloids: caffeine, theophylline and theobromine. All three alkaloids have qualitatively similar actions, but there are marked quantitative and pharmacokinetic differences.

29
METHYL XANTHINES Uses 1. Bronchial asthma and COPD (benefits by causing bronchodilatation) 2. Apnoea in premature infant (Reduction of the frequency and duration of episodes of apnoea) Adverse effects They have a narrow margin of safety. The irritant property of theophylline is reflected in gastric pain (with oral), rectal inflammation (with suppositories) and pain at site of i.m. injection. Rapid i.v. injection causes precordial pain, syncope and even sudden death—due to marked fall in BP, ventricular arrhythmias or asystole.
 Adverse effects. They have a narrow margin of safety. The irritant property of theophylline is reflected in gastric pain (with oral), rectal inflammation (with suppositories) and pain at site of i.m. injection. Rapid i.v. injection causes precordial pain, syncope and even sudden death—due to marked fall in BP, ventricular arrhythmias or asystole.")
30
ADR of Theophylline

31
ANTICHOLINERGICS Atropinic drugs cause bronchodilatation by blocking M3 receptors. β2 agonists mainly relaxes bronchiolar smooth muscle; Ipratropium blocks bronchoconstriction mainly in the larger airways Ipratropium bromide- short acting (4–6 hours) Tiotropium bromide- long acting (24 hours). Both are less efficacious than inhaled β2-mimetics in bronchial asthma. They are the bronchodilators of choice in COPD.
 Tiotropium bromide- long acting (24 hours). Both are less efficacious than inhaled β2-mimetics in bronchial asthma. They are the bronchodilators of choice in COPD.")
32
LEUKOTRIENE ANTAGONISTS
Leukotrienes (LT) are important mediators of bronchial asthma. Two LT1 receptor antagonists montelukast and zafirlukast are available. Efficacy is low They are indicated for prophylactic therapy of mild-to-moderate asthma as alternatives to inhaled glucocorticoids. ADR: very safe drugs; produce few side effects like headache and rashes
 are important mediators of bronchial asthma. Two LT1 receptor antagonists montelukast and zafirlukast are available. Efficacy is low. They are indicated for prophylactic therapy of mild-to-moderate asthma as alternatives to inhaled glucocorticoids. ADR: very safe drugs; produce few side effects like headache and rashes.")
33
Sodium cromoglycate (Cromolyn sod.)
MAST CELL STABILIZERS Sodium cromoglycate (Cromolyn sod.) It inhibits degranulation of mast cells (as well as other inflammatory cells). It is not a bronchodilator and does not antagonize constrictor action of histamine, LTs, etc. Release of mediators of asthma like histamine, LTs, interleukins, etc. is restricted. Bronchial hyperreactivity is reduced. Uses: A long-term prophylaxis in mild-to-moderate asthma Pharmacokinetics: is not absorbed orally. It is administered as an aerosol. ADR: throat irritation, cough, headache, dizziness, rashes
 It inhibits degranulation of mast cells (as well as other inflammatory cells). It is not a bronchodilator and does not antagonize constrictor action of histamine, LTs, etc. Release of mediators of asthma like histamine, LTs, interleukins, etc. is restricted. Bronchial hyperreactivity is reduced. Uses: A long-term prophylaxis in mild-to-moderate asthma. Pharmacokinetics: is not absorbed orally. It is administered as an aerosol. ADR: throat irritation, cough, headache, dizziness, rashes.")
34
MAST CELL STABILIZERS Ketotifen
It is an antihistaminic (H1) with some cromoglycate like action. Stimulation of mast cells and mediator release are reduced. It is not a bronchodilator Uses: bronchial asthma, atopic dermatitis, rhinitis, conjunctivitis, urticaria and food allergy. ADR: Generally well tolerated. Sedation and dry mouth are common.
 with some cromoglycate like action. Stimulation of mast cells and mediator release are reduced. It is not a bronchodilator. Uses: bronchial asthma, atopic dermatitis, rhinitis, conjunctivitis, urticaria and food allergy. ADR: Generally well tolerated. Sedation and dry mouth are common.")
35
CORTICOSTEROIDS Glucocorticoids are not bronchodilators.
They benefit by reducing bronchial hyperreactivity, mucosal edema and by suppressing inflammatory response to AG:AB reaction or other trigger stimuli. Corticosteroids improve airflow, reduce asthma exacerbations and may retarding airway remodeling and disease progression.

36
SYSTEMIC STEROID THERAPY
Systemic steroid therapy is resorted to in asthma under the following two situations: Severe chronic asthma: not controlled by bronchodilators and inhaled steroids Status asthmaticus/acute asthma exacerbation

37
INHALED STEROIDS These are glucocorticoids with high topical and low systemic activity Beclomethasone Budesonide Fluticasone

39
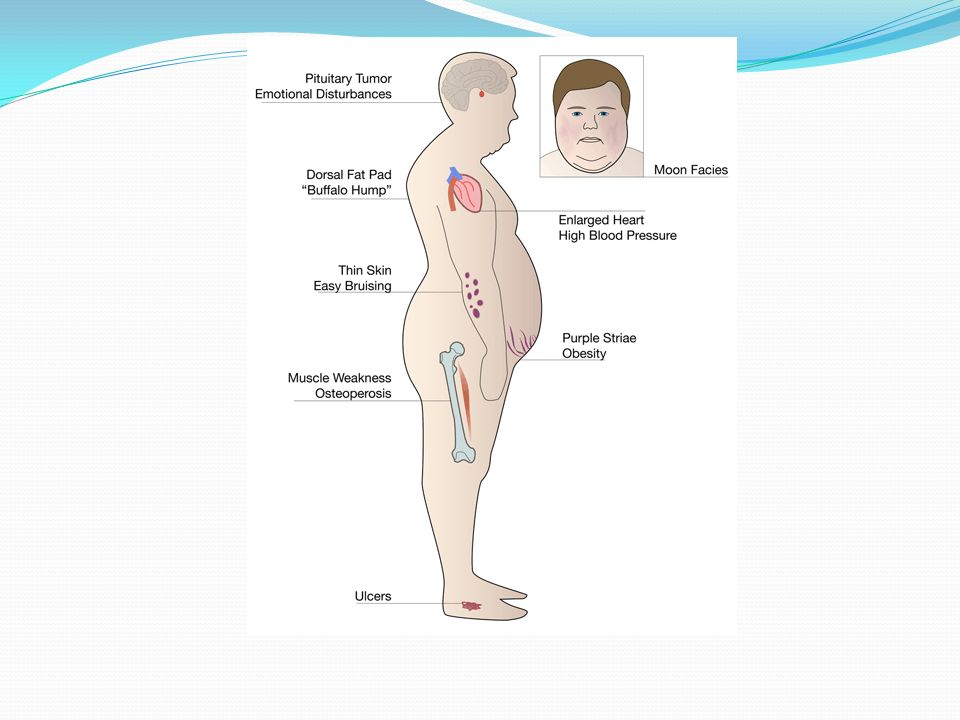
Adverse effects These can be minimized by the use of a spacer, gargling after every dose (to wash off the drug deposited on oral and pharyngeal mucosa) and prevented as well as treated by topical nystatin/clotrimazole. Systemic effects Hoarseness of voice Dysphonia Sore throat Oropharyngeal candidiasis Mood changes Osteoporosis Growth retardation in children Bruising
 and prevented as well as treated by topical nystatin/clotrimazole. Systemic effects. Hoarseness of voice. Dysphonia. Sore throat. Oropharyngeal candidiasis. Mood changes. Osteoporosis. Growth retardation in children. Bruising.")
41
ANTI-IgE ANTIBODY Omalizumab
It is a humanized monoclonal antibody against IgE. Administered s.c., it neutralizes free IgE in plasma. In severe extrinsic asthma, omalizumab has been found to reduce exacerbations and steroid requirement. It is very expensive; use is reserved for resistant asthma patients with positive skin tests or raised IgE levels who require frequent hospitalization.

42
Status asthmaticus Any patient of asthma has the potential to develop acute severe refractory asthma which may be life-threatening. Hydrocortisone (or another glucocorticoid) Salbutamol + ipratropium bromide Oxygen inhalation. Salbutamol/terbutaline 0.4 mg i.m./s.c. may be added, since inhaled drug may not reach smaller bronchi due to severe narrowing/ plugging with secretions. Intubation and mechanical ventilation, if needed.
 Salbutamol + ipratropium bromide. Oxygen inhalation. Salbutamol/terbutaline 0.4 mg i.m./s.c. may be added, since inhaled drug may not reach smaller bronchi due to severe narrowing/ plugging with secretions. Intubation and mechanical ventilation, if needed.")
Similar presentations







 SOB Cough Wheezing Tight chest.>")



 – movement of air in and out of the lungs Inhalation.>")




,>")







ANTI-HISTAMINES 2)ANTI-TUSSIVE MODIFIED BY Israa.>")
