Download presentation
Presentation is loading. Please wait.

1
Overview on Neuroendocrine tumors of pancreas
Sarah S. Al-Ghamdi 2013

2
Outlines: Basic Anatomy, Embryology and Histology Epidemiology
Classification Overview on functional types of neuroendocrine tumors of pancreas

3
Basic Anatomy: - Gland of both Exocrine and Endocrine function
- Location: Retro-peritoneum, 2nd lumbar vertebral level - Extends in an oblique, transverse position - Parts of pancreas: head, neck, body and tail

4
Basic Anatomy:

5
Cell Origins: The embryologic development of normal pancreatic tissue can be separated into three phases: 1- First: dorsal and ventral buds arise from foregut endoderm. 2- Second: cells differentiate into exocrine and endocrine cells. 3- Finally: morphogenesis occurs through growth and branching.

6
Cell Origins: These events result in three distinct cell types derived from a common precursor: 1- Exocrine acinar cells: synthesize and secrete digestive proenzymes into pancreatic ducts 2- Ductal cells: line the pancreatic ducts and secrete alkaline fluid 3- Endocrine cells: primarily involved in glucose homeostasis, are clustered into structures called islets of Langerhans

7
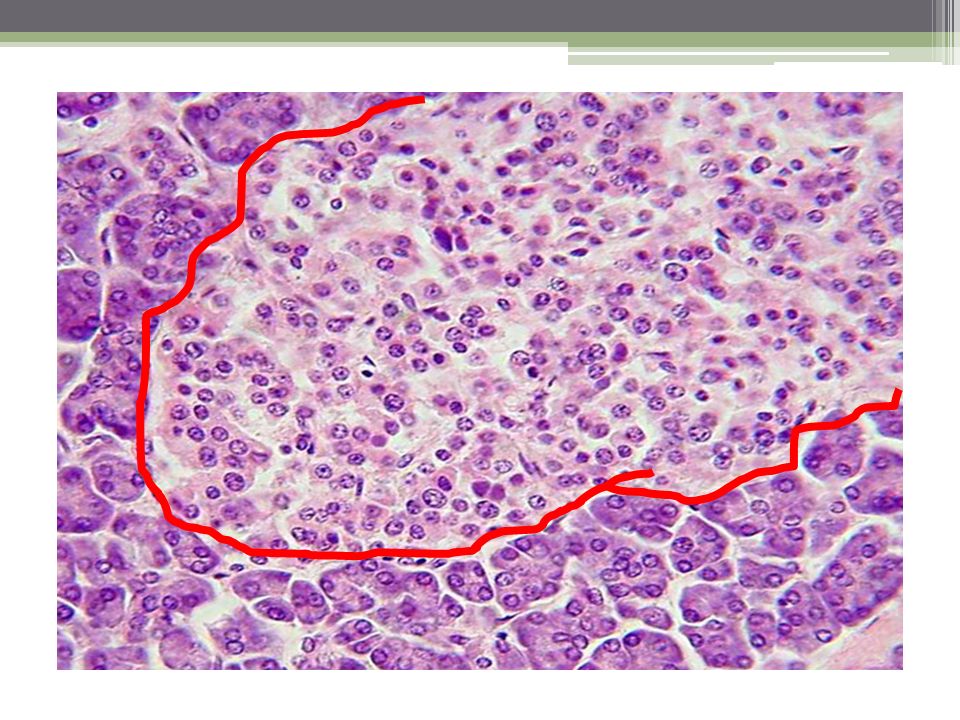
Histology: Endocrine Pancreas Exocrine Pancreas
Nests of cells - islets of Langerhans 2 major components – Acinar cells and Ducts Accounts for only 2% of the pancreatic mass They constitute 80% to 90% of the pancreatic mass Four major cell types - Alpha (A) cells secrete glucagon - Beta (B) cells secrete insulin - Delta (D) cells secrete somatostatin 20 to 40 acinar cells coalesce into a unit called the acinus Centroacinar cell (2nd cell type in the acinus) is responsible for fluid and electrolyte secretion by the pancreas
 cells secrete glucagon. - Beta (B) cells secrete insulin. - Delta (D) cells secrete somatostatin. 20 to 40 acinar cells coalesce into a unit called the acinus. Centroacinar cell (2nd cell type in the acinus) is responsible for fluid and electrolyte secretion by the pancreas.")
9
Pancreatic Cancer: Pancreatic cancer is the fourth leading cause of cancer death in the United States. Approximately individuals in the USA and over individuals worldwide die from the disease each year . The incidence approximates the mortality rate, which reflects the poor prognosis of pancreatic cancer. the 5-year survival rate for affected patients remains under 5%

10
WHO Classification: Lymphoma Epithelial Tumors benign
Premalignant lesion Malignant Neuroendocrine neoplasm Mesenchymal tumours Lymphangioma NOS Lymphoma NOS Solitary fibrous tumor Lymphoma Diffuse large B-cell lymphoma Secondary Tumors

11
Neuroendocrine Tumors:
Pancreatic neuroendocrine tumors, also called islet cell tumors, are rare tumors that form from the hormone-producing cells in the pancreas called islet cells It accounts for less than 5% of all pancreatic tumors. They tend to grow slower than the adenocarcinoma

12
Types: Pancreatic neuroendocrine microadenoma
Neuroendocrine tumor: G1 , G2 , NOS - Large cell and Small cell neuroendocrine carcinoma Gastrinoma Glucagonoma Insulin producing carcinoma (insulinoma) Somatostatinoma Vipoma
 Somatostatinoma. Vipoma.")
13
Neuroendocrine Tumors:
Functional or non-Functional Benign Vs malignant Considered malignant except microadenomas (less than 5 mm, usually incidental at autopsy), because no histologic criteria differentiates benign and malignant (except metastases) Cell of origin ?? Can occur as part of 4 inherited disorders: MENI, VHL, NF-1 and TSC 80% occur in MEN1 patients, usually age 50-60
, because no histologic criteria differentiates benign and malignant (except metastases) Cell of origin Can occur as part of 4 inherited disorders: MENI, VHL, NF-1 and TSC. 80% occur in MEN1 patients, usually age")
14
Neuroendocrine Tumors : (prognosis)
Tumor size > 3 cm Invasion of stroma, capsule, vessels or adjacent organs Glandular/solid pattern Older age, high proliferation index (Ki-67 of 5% or more Necrosis, vascular invasion, perineural invasion or CK19+

15
NET G1- G2 Rare, arise from serotonin secreting cells normally present in pancreas Well-differentiated: cells with features similar to normal gut endocrine cell, expressing general markers of neuroendocrine differentiation and hormones according to site, with mild- to-moderate nuclear atypia and a low number of mitoses G1 (NET G1): mitotic count <2/10 HPF or ≤2% Ki67 index G2 (NET G2): mitotic count 2-20/10 HPF or 3-20% Ki67 index
: mitotic count <2/10 HPF or ≤2% Ki67 index. G2 (NET G2): mitotic count 2-20/10 HPF or 3-20% Ki67 index.")
17
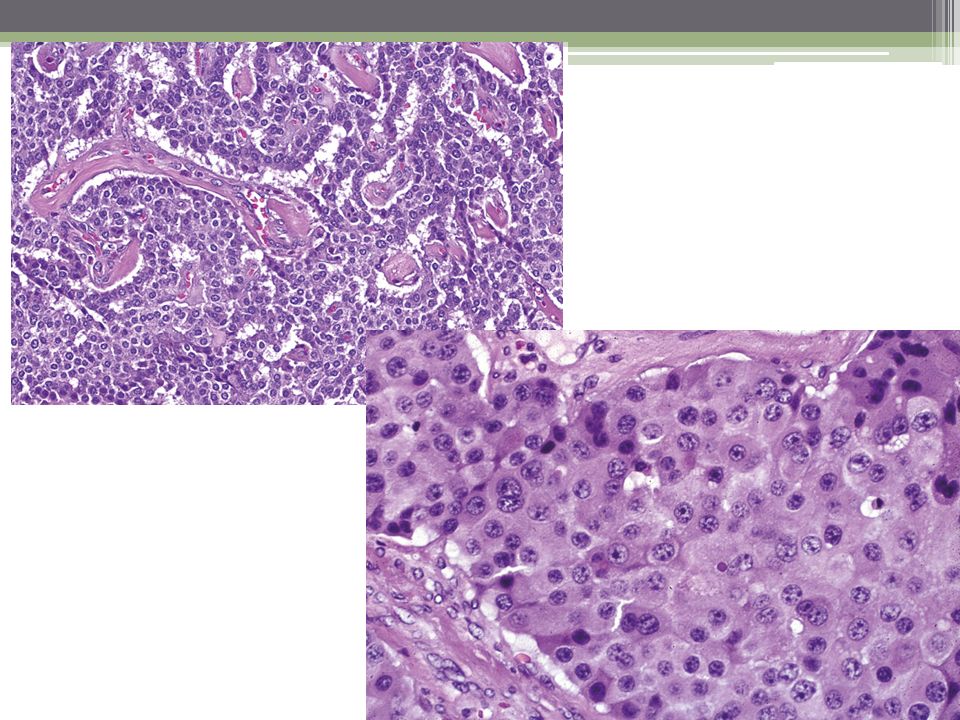
Neuroendocrine carcinoma, NOS
- Poorly differentiated, high grade malignant neoplasm - Composed of small, intermediate or large cells, - diffusely expressing neuroendocrine markers (diffuse staining for synaptophysin; faint or focal staining for chromogranin A) - marked nuclear atypia, multifocal necrosis and a high number of mitoses (> 20 per 10 HPF)
 - marked nuclear atypia, multifocal necrosis and a high number of mitoses (> 20 per 10 HPF)")
18
Neuroendocrine carcinoma, NOS
- Represents less than 3% of pancreatic neuroendocrine tumors - May produce ACTH - Associated with hypercalcemia

19
Large number of poorly differentiated fusiform cells and focal necrosis

20
Pancreatic neuroendocrine carcinoma (NEC)
Pancreatic neuroendocrine carcinoma (NEC). Note the very high mitotic rate
. Note the very high mitotic rate.")
21
Insulinoma (beta cell tumor)
Functionally active and commonly benign endocrine tumour of the pancreas with evidence of beta cell differentiation and clinical hypoglycemia due to inappropriate secretion of insulin Only 7-10% have malignant behavior Whipple’s triad

22
Insulinoma (beta cell tumor)
")
23
Insulinoma (beta cell tumor)
")
24
-Gastrinoma (G cell tumor)
Functionally active and usually malignant endocrine tumour with clinical symptoms due to inappropriate secretion of gastrin ZES

25
Gastrinoma: C/P Associated with hypersecretion of gastric acid and severe peptic ulceration 90% have ulcers; 85% in duodenum/jejunum, 15% in stomach 50% have diarrhea Tumors usually in pancreas or duodenum peripancreatic soft tissue, gastric antrum Also ovary, mesentery, liver, intra-abdominal lymph nodes (unclear if due to ectopic pancreatic tissue or metastases) 50% are locally invasive or metastatic at diagnosis
 50% are locally invasive or metastatic at diagnosis.")
26
Gastrinoma: Malignant tumor has trabecular pattern, hyaline and fibrous tissue between epithelial cell cords

27
Glucagonoma: Rare Arising from alpha cells of pancreas; often displays vascular invasion and may metastasize Adult females, age 40+

28
Multiple small tumors with gyriform growth pattern
Types Glucagonoma syndrome Multiple small tumors with gyriform growth pattern High incidence of malignancy Nearly always benign Necrolytic migratory erythema Sore red tongue, angular stomatitis Severe weight loss, depression Deep venous thromboses May develop overwhelming infection Normochromic, normocytic anemia Strongly immunoreactive for glucagon Typical granules on EM

29
EM-Glucagon granules:

30
Necrolytic migratory erythema

31
VIPoma called Verner-Morrison tumors - tumors secrete vasoactive intestinal peptide (VIP) 90% of VIPomas arise from pancreas Diarrhea (cholera-like), hypokalemia, achlorhydria It contains pancreatic polypeptide, calcitonin, alpha chain of hCG
, hypokalemia, achlorhydria. It contains pancreatic polypeptide, calcitonin, alpha chain of hCG.")
32
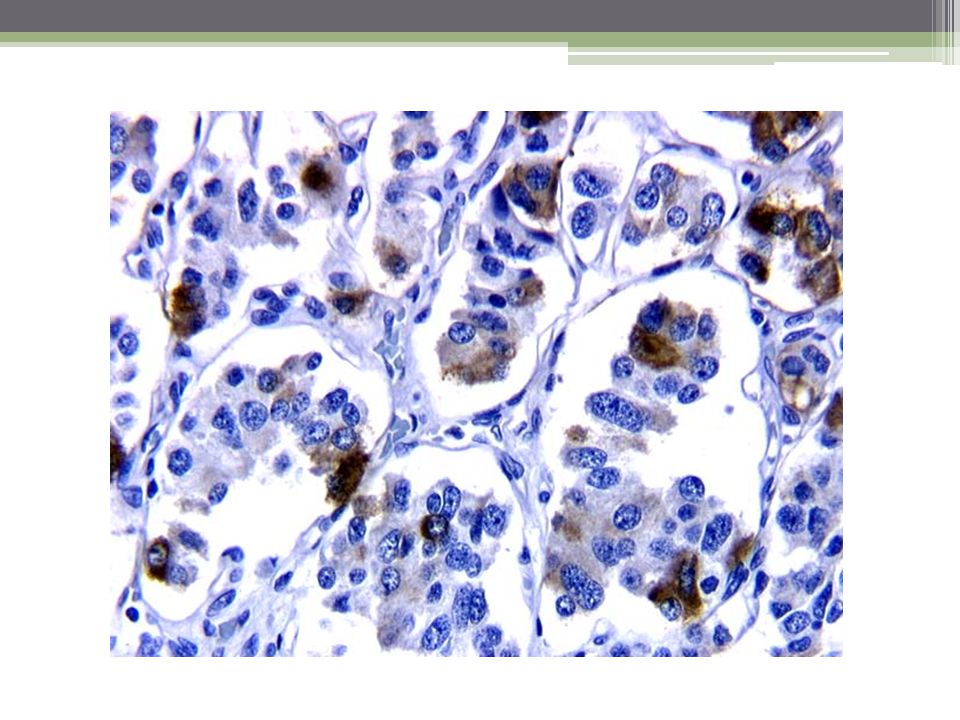
Interconnecting nests and trabeculae of uniform cuboidal cells with granular cytoplasm and central round nuclei

33
Somatostatinoma Functionally active and usually malignant endocrine tumour with evidence of D-cell differentiation Only rarely associated with somatostainoma syndrome (diabetes, cholecystolithiasis, steatorrhea, hypochlorhydria) May be in duodenal wall May have psammoma bodies
 May be in duodenal wall. May have psammoma bodies.")
35
The endoscopic finding of the duodenal submucosal tumor

36
Thank You …

Similar presentations


 EXOCRINE PANCREASE Lecture Dr. Gamal Hamra Wednesday 01/12/1430 (18/11/2009)>")

 are derived from the diffuse neuroendocrine system, which is made up of.>")

>")










>")

