Download presentation
Presentation is loading. Please wait.

1
IMAGING OF THE CHEST Bengi Gürses MD.
Yeditepe University School of Medicine Department of Radiology

2
Imaging Modalities Direct radiography (Chest x-ray)
Computed Tomography MRI and US in selected patients...

3
Chest X Ray

4
INTRODUCTION Positioning: Posteroanterior (PA) Lateral (left)
Anteroposterior (AP) Lateral decubitus
 Lateral decubitus.")
5
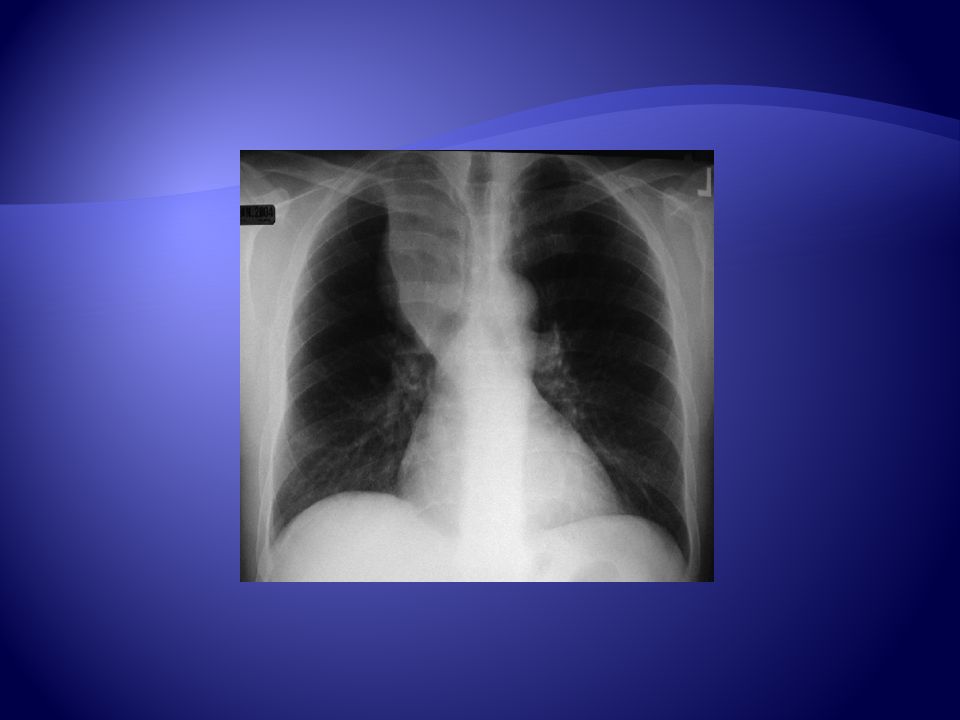
Positioning The x ray enters the patient posteriorly and exit anteriorly with the patient’s chest on the film cassette. There is 180 cm distance between the x-ray tube and cassette. Obtained in deep inspiration !!!

6
Positioning The patient’s left side is against the film. The right side is magnified. Obtained in deep inspiration !!!

7
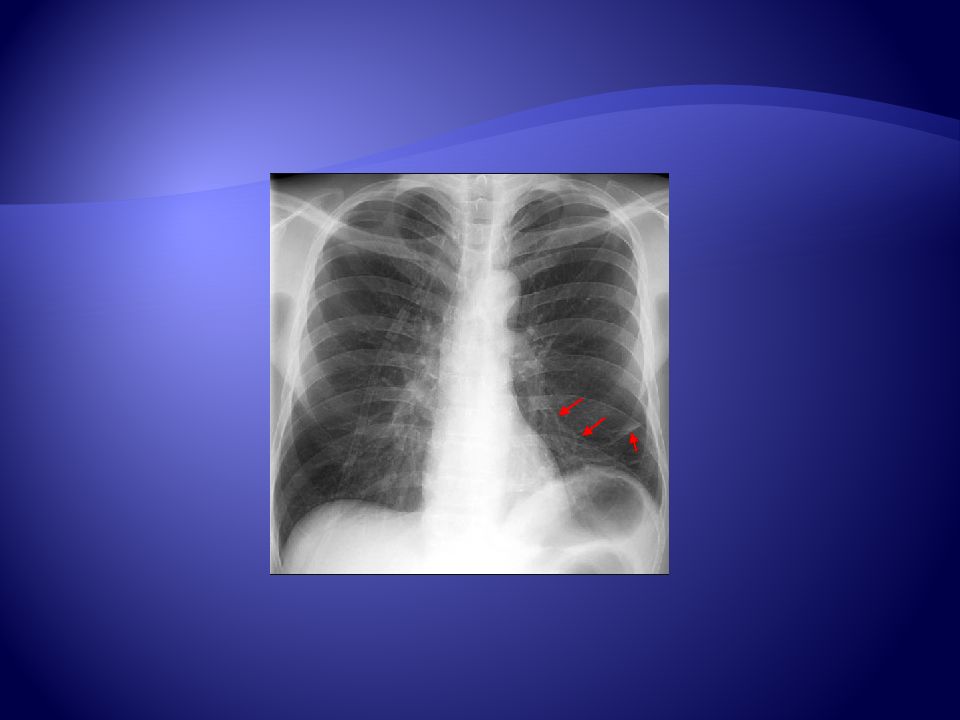
The right ribs (red arrows below) are larger due to magnification and usually projected posterior to the left ribs if the patient was examined in a true lateral position. This can be very helpful if there is a unilateral pleural effusion seen only on the lateral view.

8
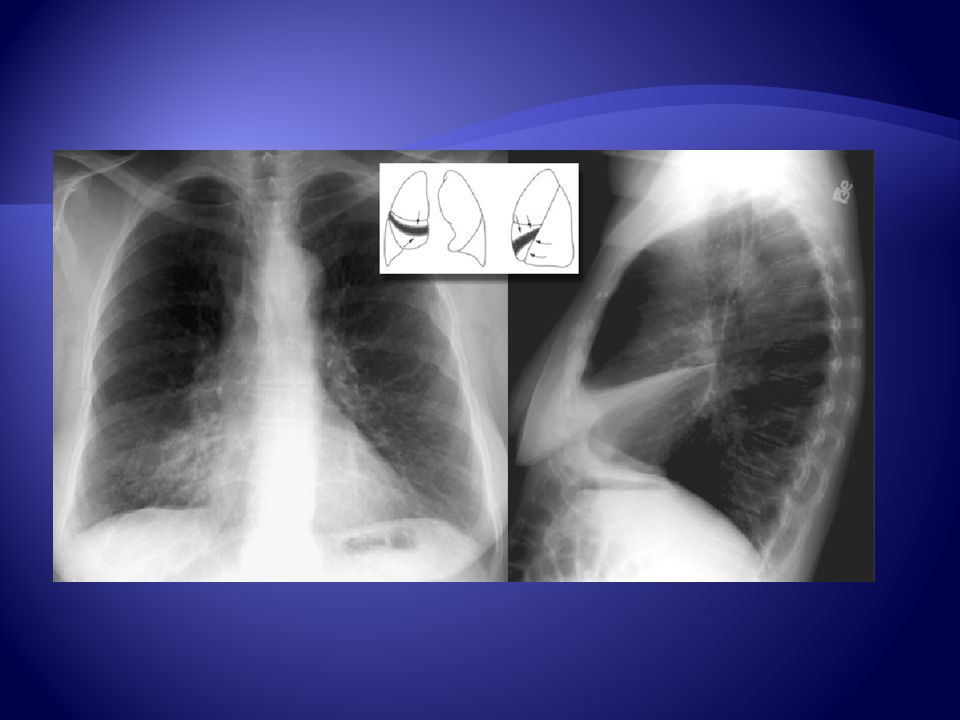
The left hemidiaphragm is usually lower than the right
The left hemidiaphragm is usually lower than the right. Also, since the heart lies predominantly on the left hemidiaphragm the result on a lateral film is silouhetting out of the anterior portion of the hemidiaphragm, whereas the anterior right hemidiaphragm remains visible. Notice how the right diaphragm (red arrows) continues anteriorly, while the left diaphragm disappears (black arrow) because of the silouhetting caused by the heart. Also notice how the right diaphragm at the blue arrows continues past the smaller left ribs and ends at the larger and more posterior right ribs.
 continues anteriorly, while the left diaphragm disappears (black arrow) because of the silouhetting caused by the heart. Also notice how the right diaphragm at the blue arrows continues past the smaller left ribs and ends at the larger and more posterior right ribs.")
10
The PA (posterioranterior) film is obtained with the patient facing the cassette and the x-ray tube 180 cm away. This distance diminishes the effect of beam divergence and magnification of structures closer to the x-ray tube. AP (anteriorposterior) position the x-ray tube is 100 cm from the patient. The heart shadow is magnified because it is an anterior structure.
 position the x-ray tube is 100 cm from the patient. The heart shadow is magnified because it is an anterior structure.")
11
PA AP

12
The patient can also be examined in a lateral decubitus position.
This could be helpful to assess the volume of pleural effusion and demonstrate whether a pleural effusion is mobile or loculated.

13
Is the film technically adequate?????

14
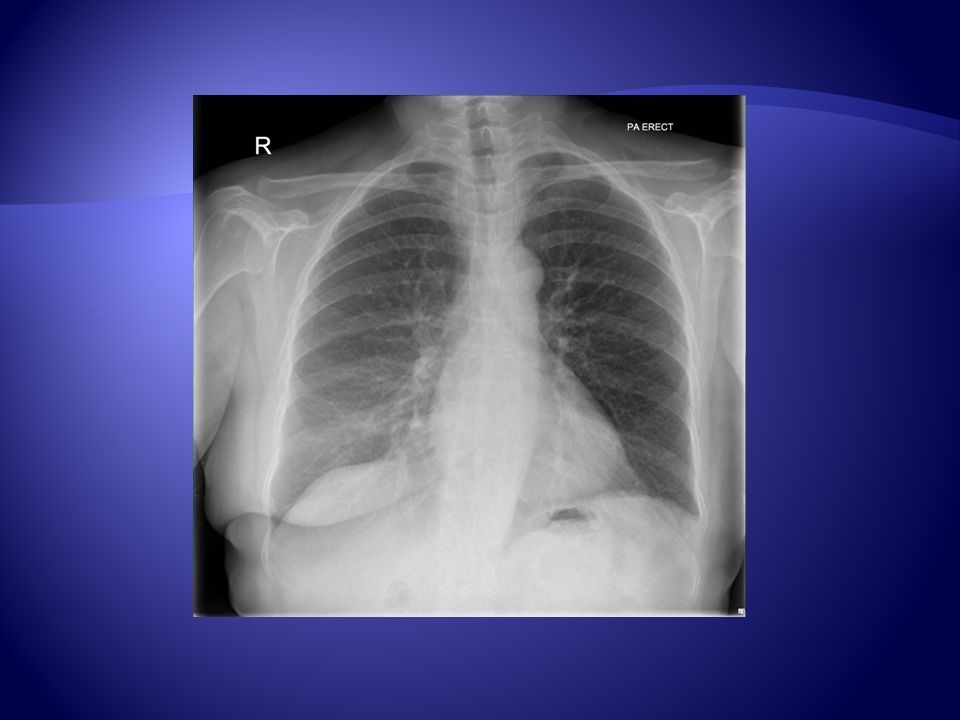
The patient should be examined in full inspiration
The patient should be examined in full inspiration. This greatly helps the radiologist to determine if there are intrapulmonary abnormalities. The diaphragm should be found at about the level of the 8th - 10th posterior rib or 5th - 6th anterior rib on good inspiration.

15
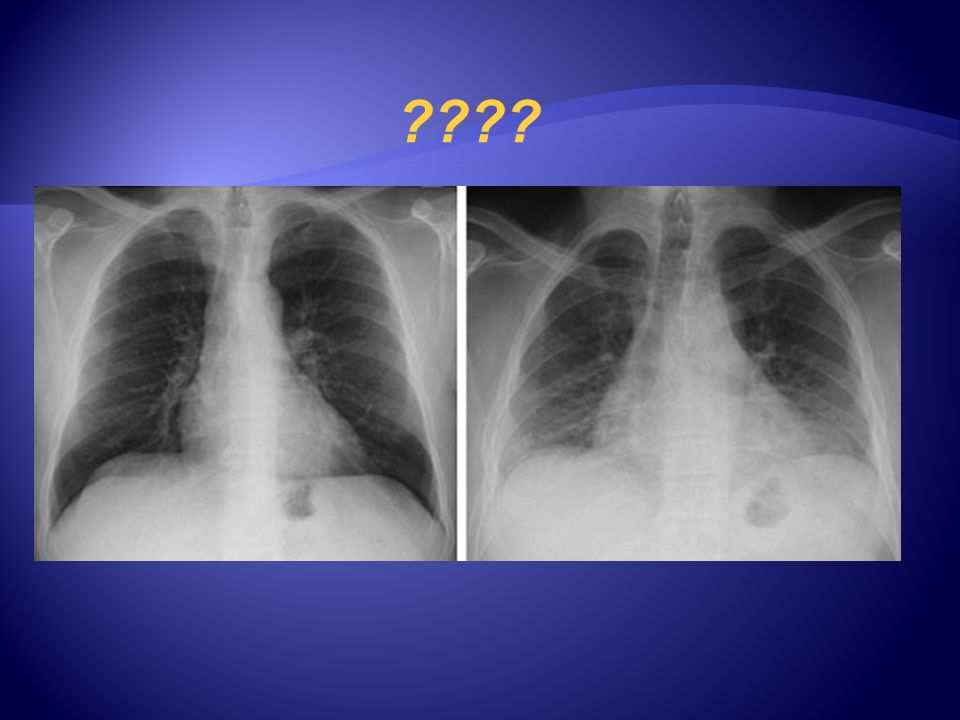
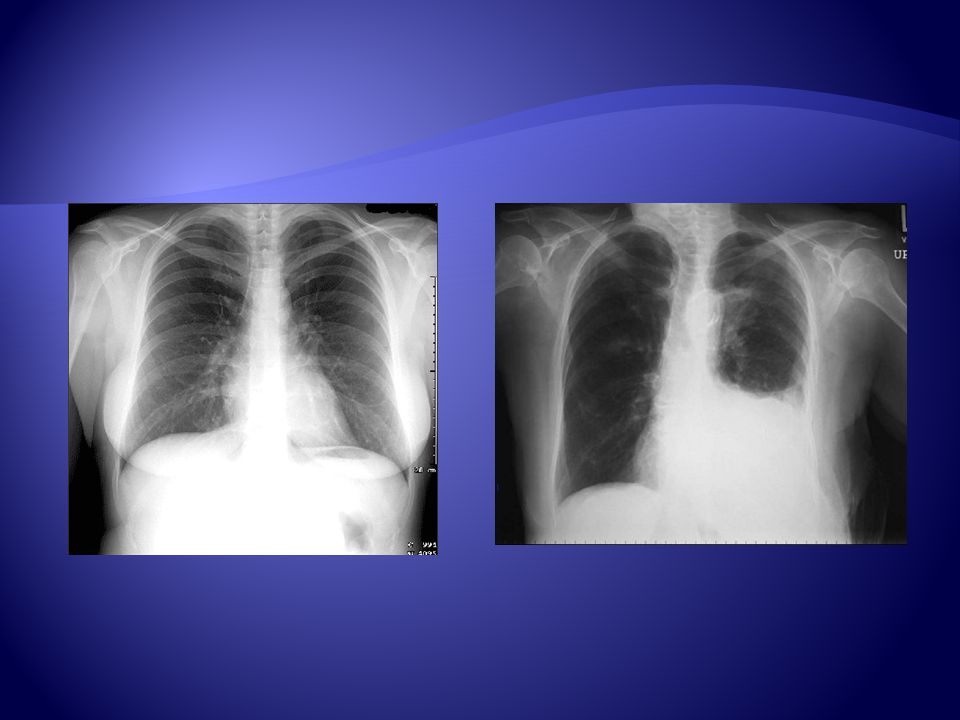
A patient can appear to have a very abnormal chest if the film is taken during expiration.
On the first film, the loss of the right heart border silhouette would lead you to the diagnosis of a possible pneumonia. On repeat exam with improved inspiration, the right heart border is normal.

16
Adequate penetration of the patient by radiation is also required for a good film. On a good PA film, the thoracic spine disc spaces should be barely visible through the heart but bony details of the spine are not usually seen. On the other hand penetration is sufficient that bronchovascular structures can usually be seen through the heart.

17
On the lateral view, look for proper penetration and inspiration by observing that the spine appears to be darken as you move caudally. This is due to more air in lung in the lower lobes and less chest wall. The sternum should be seen edge on and posteriorly you should see two sets of ribs.

18
Underpenetrated Overpenetrated

19
Rotation ???

20
If there is rotation of the patient, the mediastinum may look very unusual. One can access patient rotation by observing the clavicular heads and determining whether they are equal distance from the spinous process of the thoracic vertebral bodies.

21
Rotation ???

22
In this rotated film skin folds can be mistaken for a tension pneumothorax !!!!! Wrong positioning of the heads of the clavicles and the spinous processes

23
????
24
INTERPRETATION

25
BONE AIR WATER TISSUE

26
LUNG ANATOMY Trachea Carina Right and left pulmonary bronchi
Lobar bronchi

27
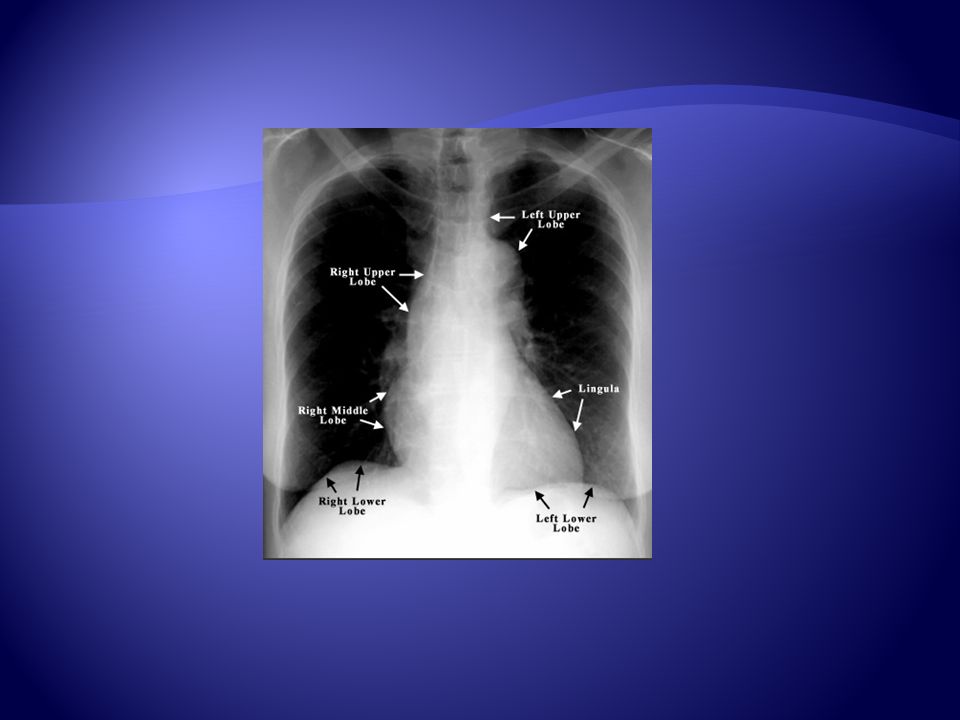
LUNG ANATOMY Right Lung Left Lung *Superior lobe *Middle lobe
*Inferior lobe Left Lung

28
Right Lung Superior lobe Middle lobe Inferior lobe

29
PA View Lateral View Extensive overlap Lower lobes extend high
Extent of lower lobes

30
*The right upper lobe (RUL) occupies the upper 1/3 of the right lung
*Posteriorly, the RUL is adjacent to the first 3-5 ribs *Anteriorly, the RUL extends inferiorly as far as the 4th right inferior rib

31
*The right middle lobe is typically the smallest of the three lobes, appears triangular in shape, narrowest to the hilum

32
*The right lower lobe is the largest
*Posteriorly, the RLL extends as far superiorly as the 6th thoracic vertebra, and inferiorly till the diaphragm

33
*The three lobes are seperated from eachother by two fissures
*The minor fissure seperates the upper and middle lobes and is oriented horizontally *The major fissure, which is oriented obliquely, extends above till the 4th vertebra

34
*There is no minor fissure on the left
*There are two lobes: LUL, LLL Major fissure is similar to the one on the left side, slightly inferior in location *The portion of the left lobe that corresponds anatomically to the right middle lobe is incorporated to the upper lobe

35
PA View Aortic arch Pulmonary trunk Left atrial appendage
Left ventricle Right ventricle SVC Right hemidiaphragm Left hemidiaphragm Horizontal fissure

37
Patient Data (name history #, age, sex, old films)
Routine Technique: AP/PA, exposure, rotation, supine or erect Trachea: midline or deviated, caliber, mass Lungs: abnormal shadowing or lucency Pulmonary vessels: artery or vein enlargement Hila: masses, lymphadenopathy Heart: thorax: heart width > 2:1 ? Cardiac configuration? Mediastinal contour: width? mass? Pleura: effusion, thickening, calcification Bones: lesions or fractures Soft tissues: don’t miss a mastectomy ICU Films: identify tubes first and look for pneumothorax

41
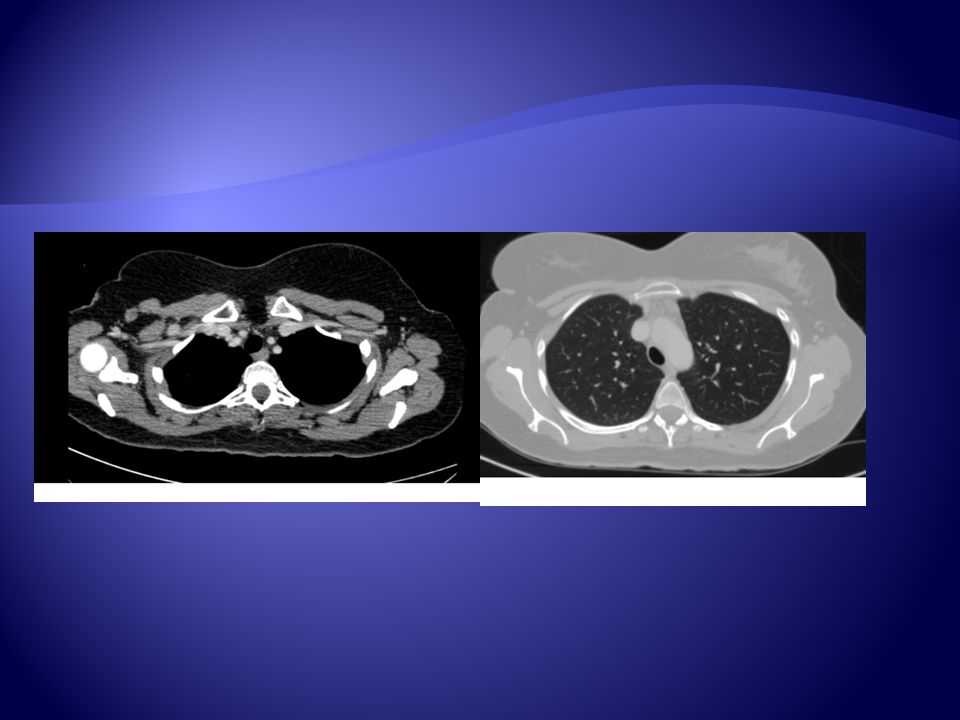
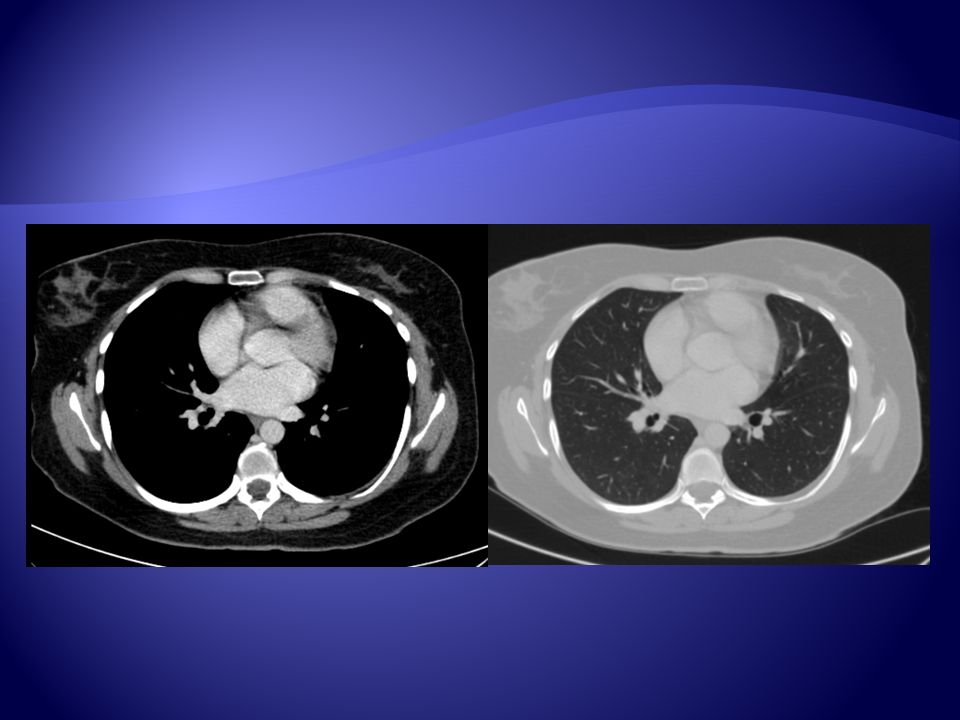
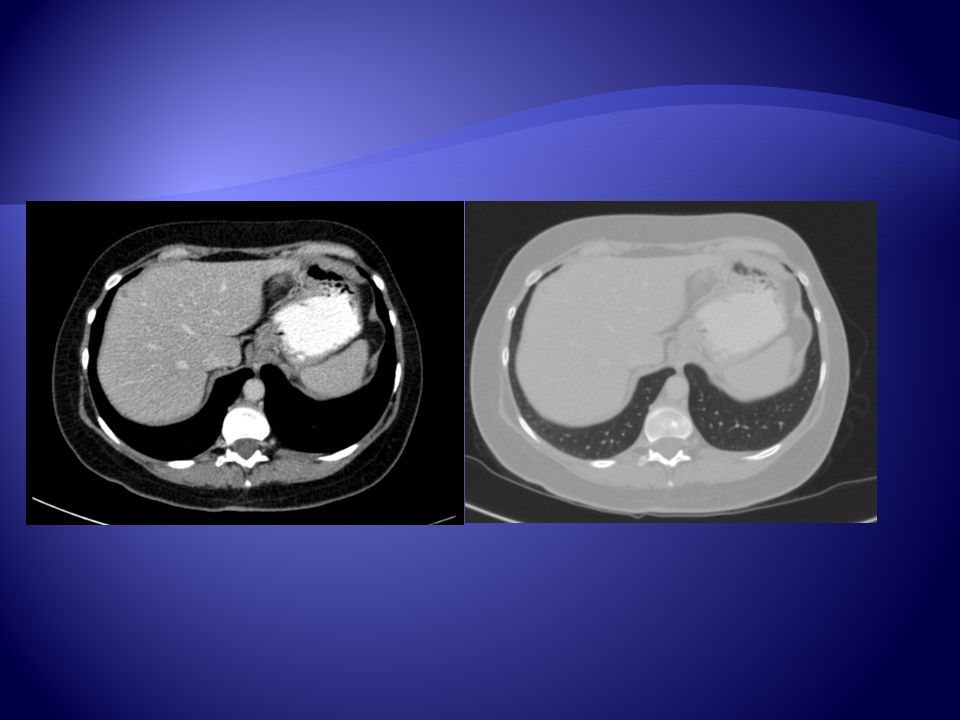
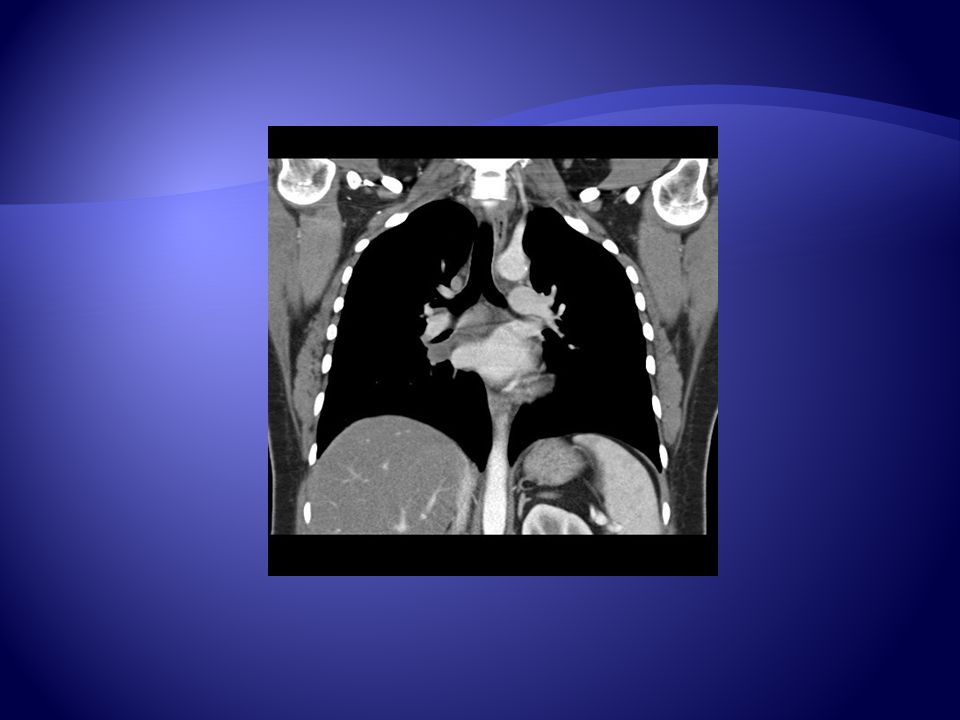
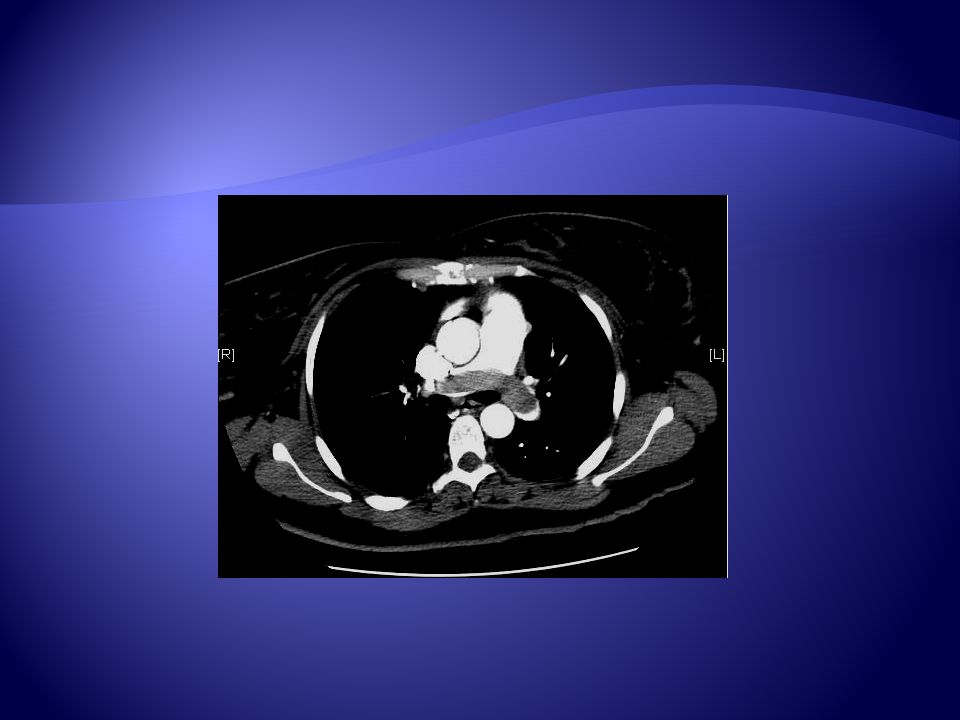
Computed Tomography

47
The Silhouette Sign An intrathoracic radio-opacity if in anatomic contact with the border of a mediastinal structure, will obscure that border.

50
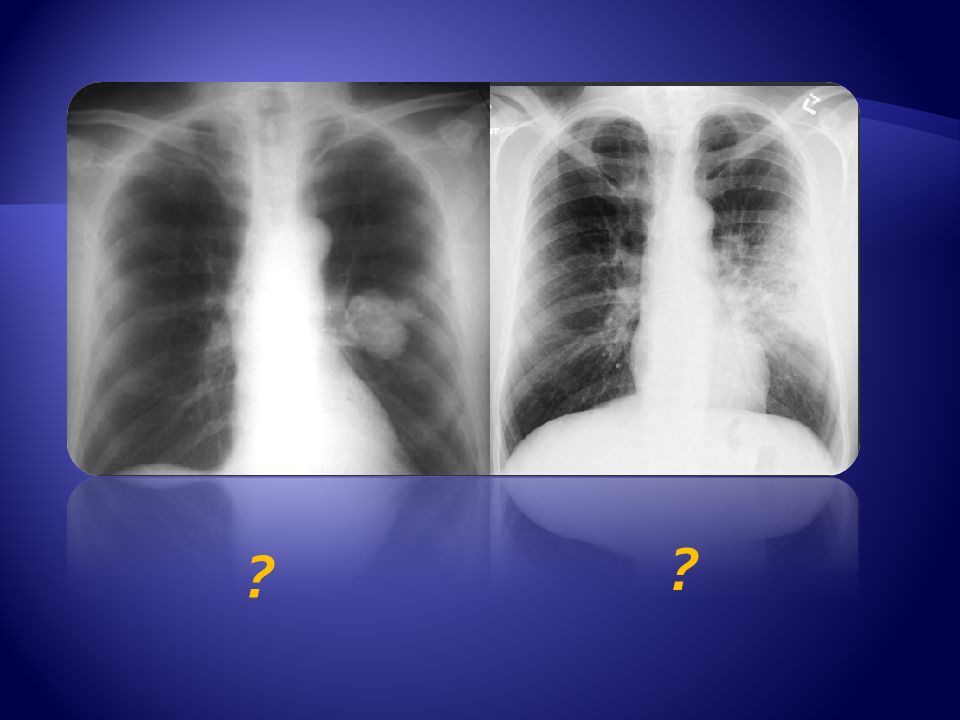
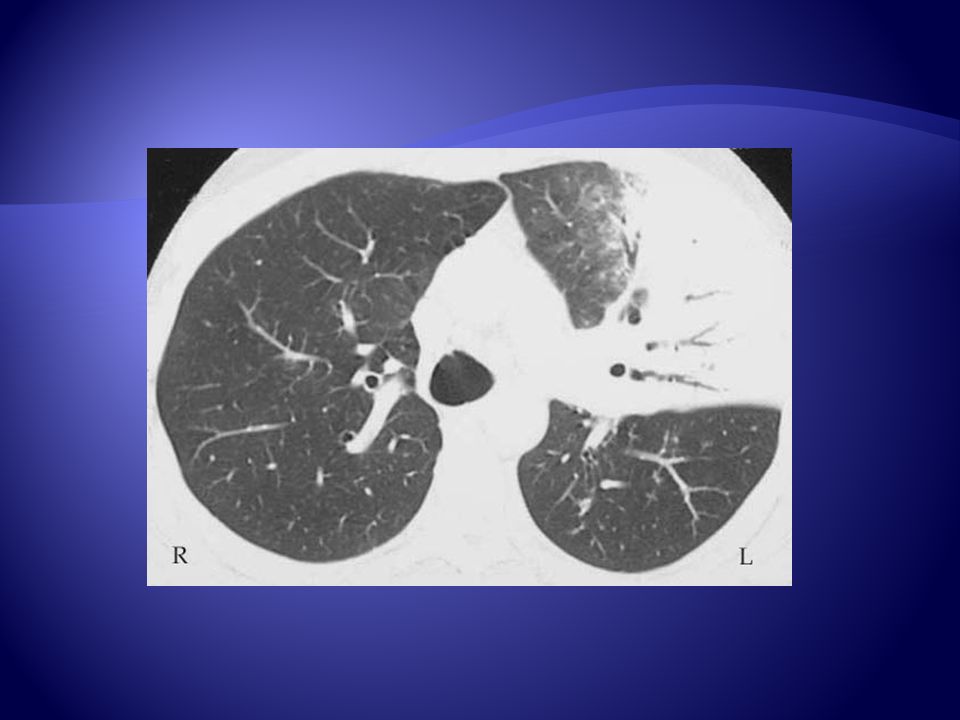
Abnormal opacity in the left upper lobe.
Left ► the opacity would best be described as a mass because it is well-defined. Right ► the opacity is poorly defined, belongs to airspace disease (pneumonia).
.")
51
Air Bronchogram ???

52
An air bronchogram is a tubular outline of an airway made visible by filling of the surrounding alveoli by fluid or inflammatory exudates. Etiology; lung consolidation, pulmonary edema, nonobstructive pulmonary atelectasis, severe interstitial disease, neoplasm, and normal expiration.

56
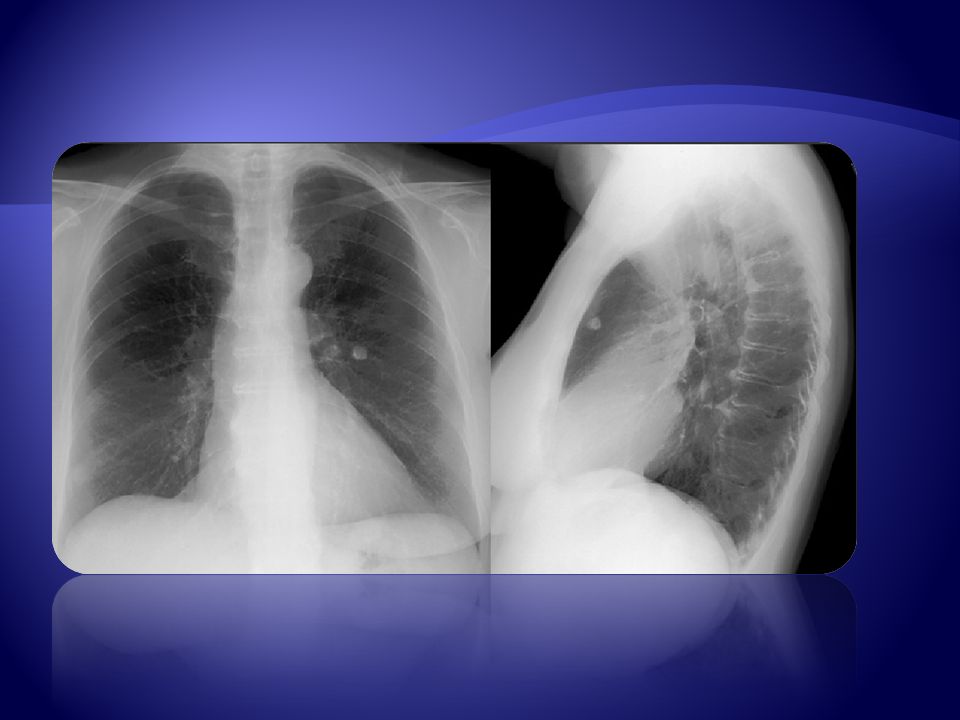
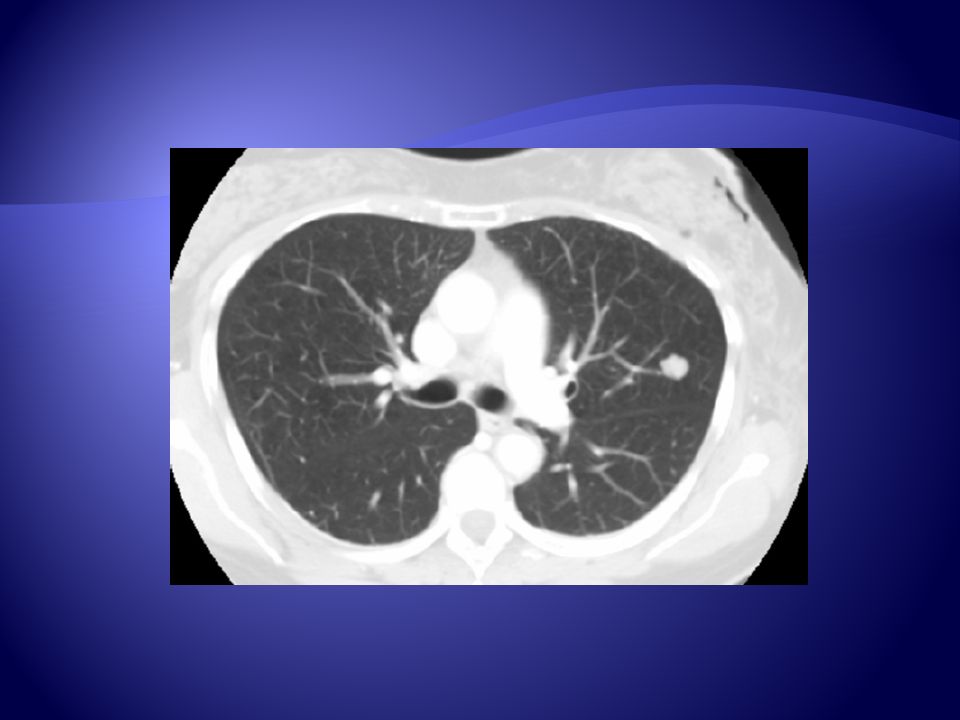
Solitary Pulmonary Nodule ???

59
A solitary nodule in the lung can be totally innocuous or potentially a fatal lung cancer.
Initial step in analysis is to compare the film with prior films if available. A nodule that is unchanged for two years is almost certainly benign. If the nodule is completely calcified or has central or stippled calcium it is benign. Nodules with irregular calcifications or those that are off center should be considered suspicious, and need to be worked up further with a PET scan or biopsy.

60
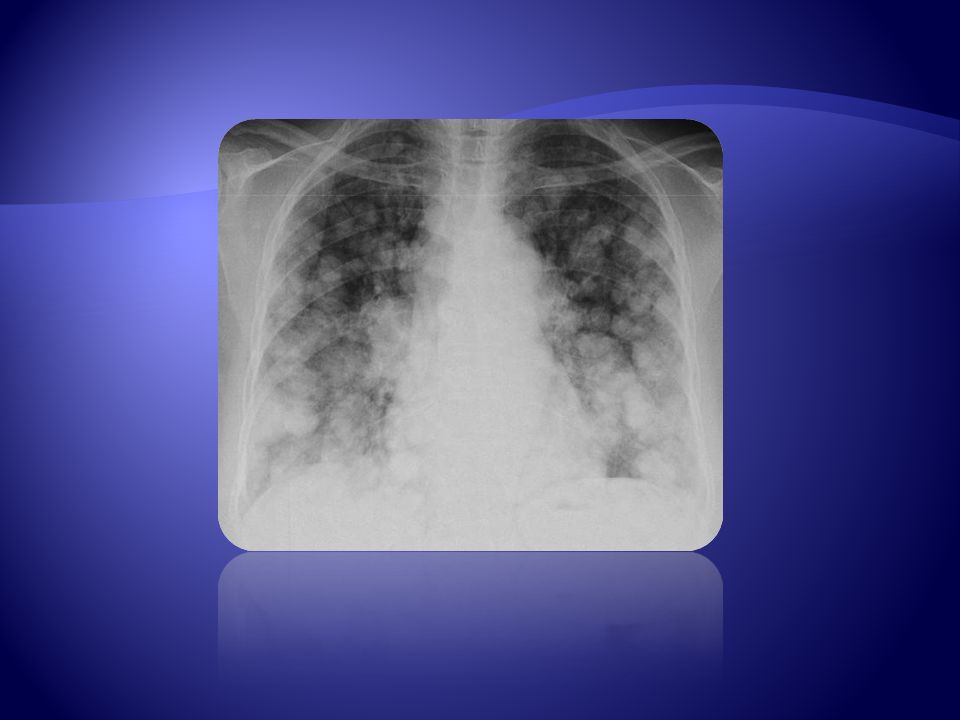
Multiple Pulmonary Nodules ???

63
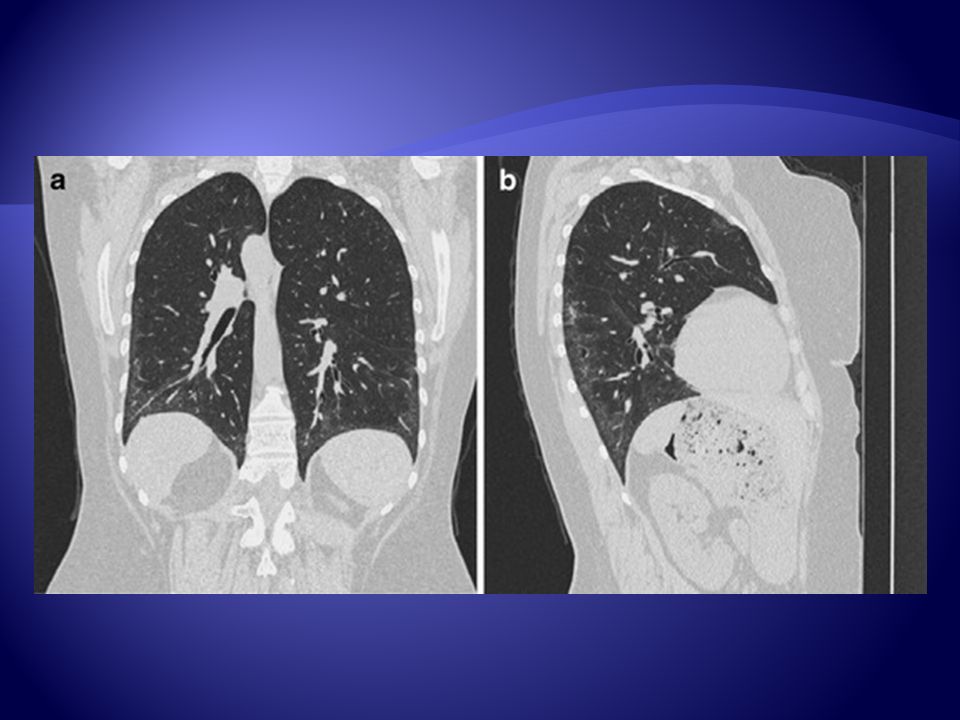
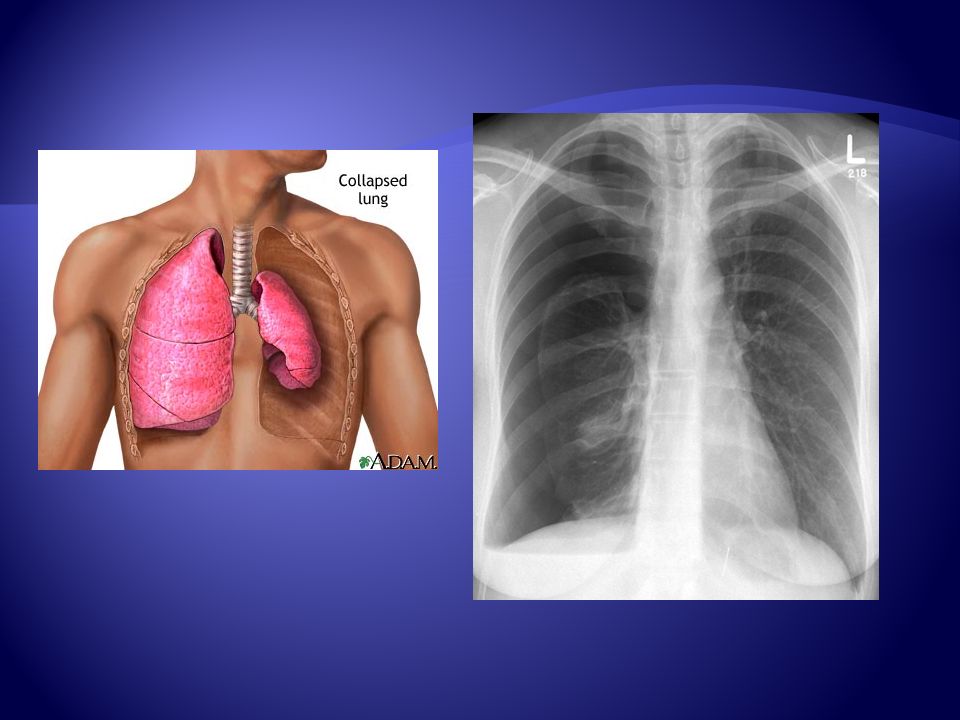
Atelectasis ???

64
Atelectasis is almost always associated with a linear increased density on chest x-ray.
The apex tends to be at the hilum. The density is associated with volume loss. Some indirect signs of volume loss include vascular crowding or fissural, tracheal, or mediastinal shift, towards the collapse. There may be compensatory hyperinflation of adjacent lobes, or hilar elevation (upper lobe collapse) or depression (lower lobe collapse).
 or depression (lower lobe collapse).")
68
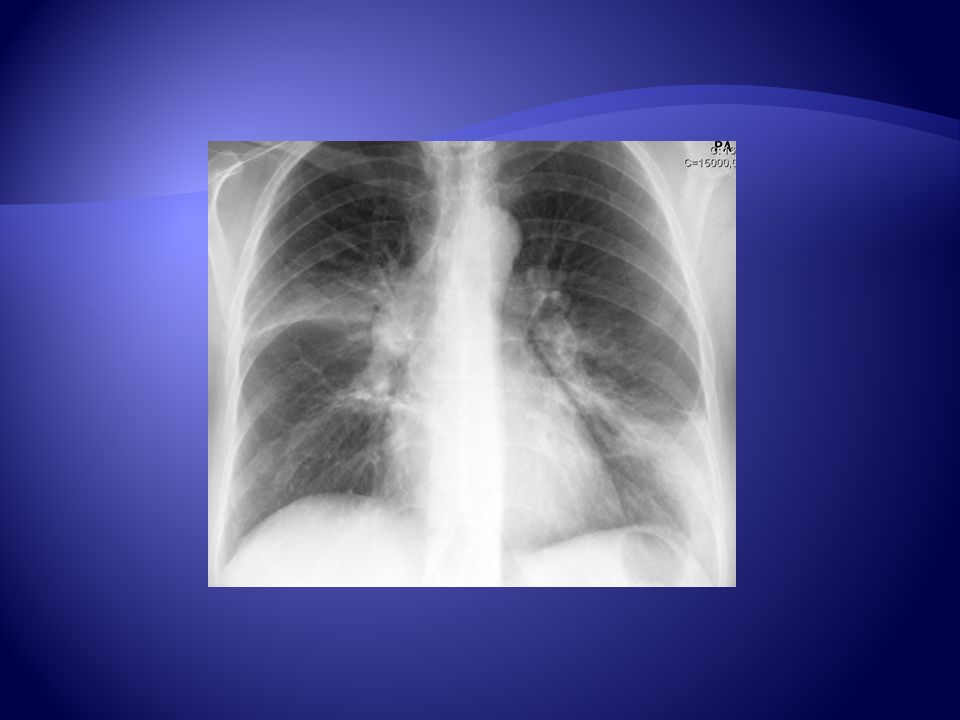
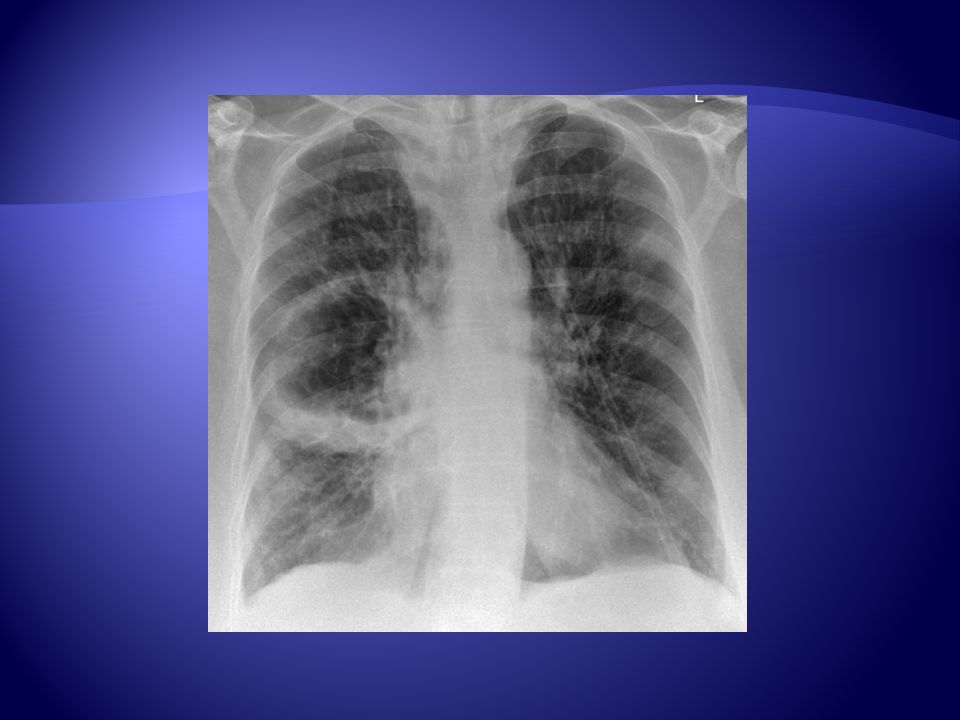
Pneumonia ???

69
airspace opacity, lobar consolidation with ill-defined borders, or interstitial opacities

70
Opacity ???

71
? ?
72
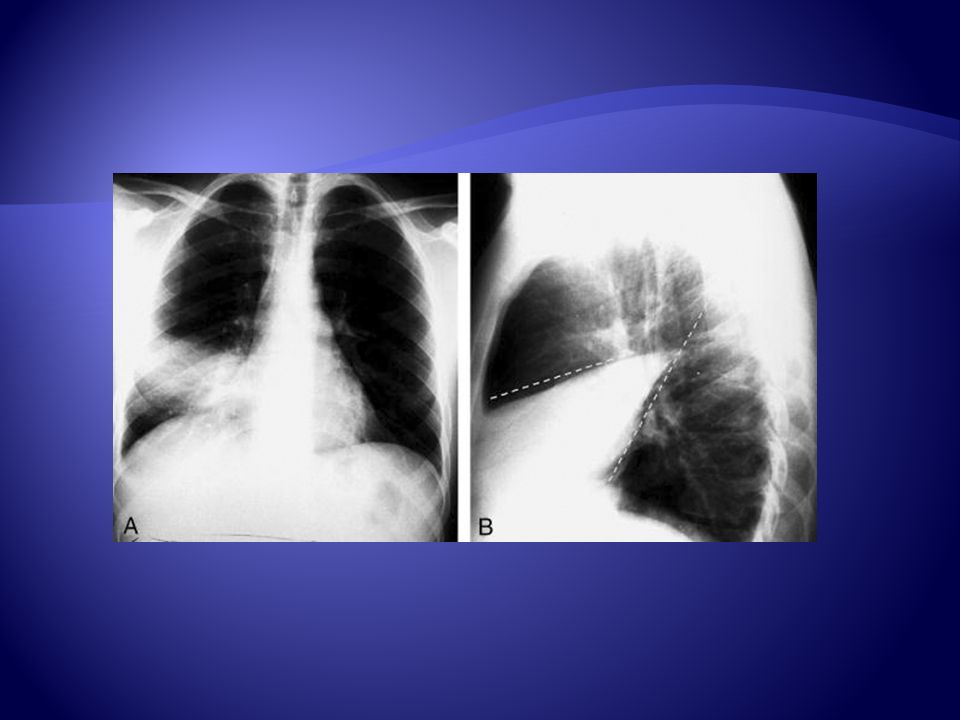
Pulmonary Embolism ???

73
Signs that may be present in PE are; Westermark's sign (oligemia in area of involvement), increased size of a hilum (caused by thrombus impaction), atelectasis with elevation of hemidiaphragm and linear or disk shaped densities, pleural effusion, consolidation, and Hampton's hump (rounded opacity). Roughly ten percent of pulmonary embolisms result in pulmonary infarction In the case of pulmonary infarctions, the main radiographic feature is multifocal consolidation at the pleural base in the lower lungs

75
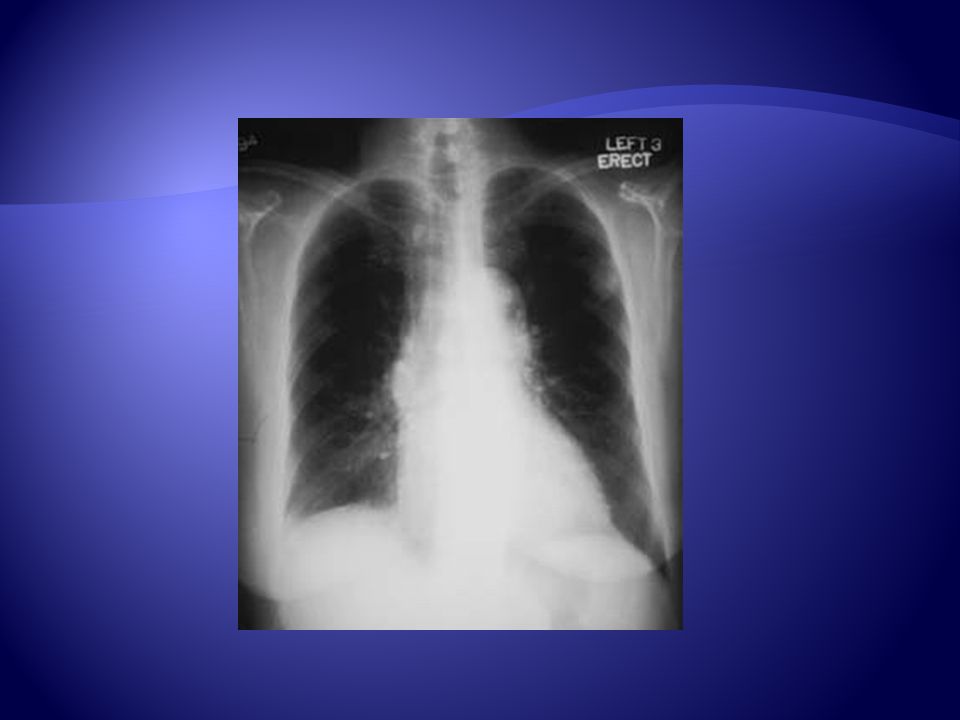
Pleural Effusion ???

77
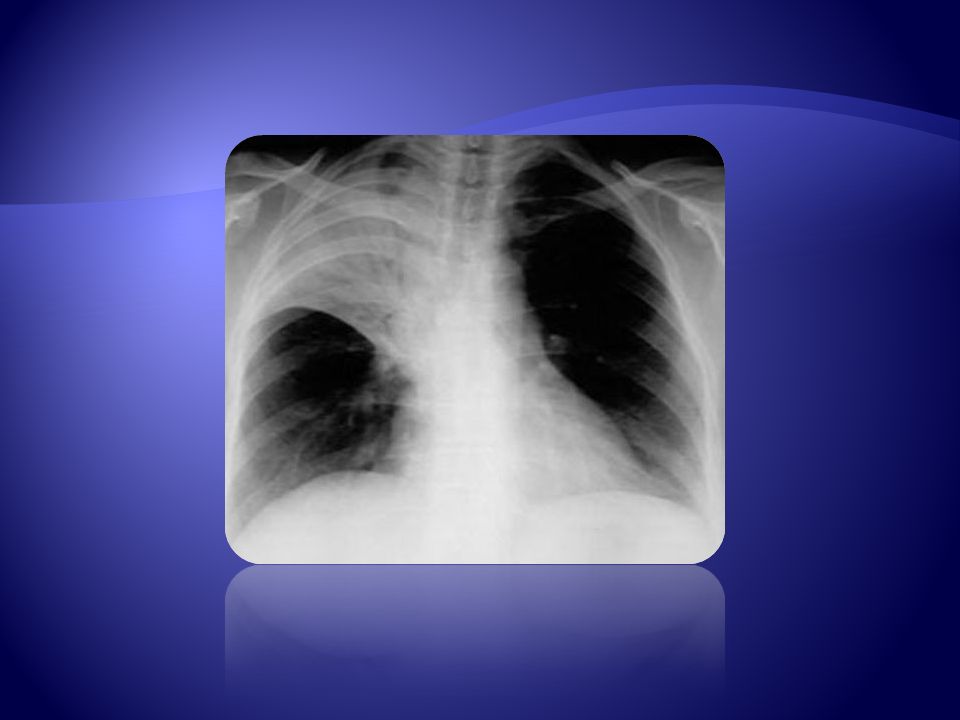
Pneumothorax ???

79
CASES

Similar presentations
















 –Partial.>")












