Download presentation
Presentation is loading. Please wait.

1
Kirk N. Garratt, MD, FSCAI Welcome to the 11:40am Treatment of Thrombotic Lesions

2
Kirk N. Garratt MSc MD FSCAI FACC Associate Director, Division of Cardiac Interventions Clinical Director of Research Associate Director, Coronary Intensive Care Unit Kirk N. Garratt MSc MD FSCAI FACC Associate Director, Division of Cardiac Interventions Clinical Director of Research Associate Director, Coronary Intensive Care Unit

3
Disclosure Information Treatment of Thrombotic Lesions Kirk N. Garratt MSc MD, FSCAI The following relationships exist related to this presentation: The Medicines Company: (G) (AC) (SB) BMS/sanofi-aventis: (SB) Boston Scientific Corp: (G) (C) (SB) (AC) (O) Daiichi-Sankyo/Lilly: (SB) (E ): Employment (M): Management Position (I): Independent Contractor (G): Grant/Research Support (C): Consultant (SB): Speaker’s Bureau (AC): Advisory Committee (B): Board Member (O): Other Off label use of products will not be discussed in this presentation
 (AC) (SB) BMS/sanofi-aventis: (SB) Boston Scientific Corp: (G) (C) (SB) (AC) (O) Daiichi-Sankyo/Lilly: (SB) (E ): Employment (M): Management Position (I): Independent Contractor (G): Grant/Research Support (C): Consultant (SB): Speaker’s Bureau (AC): Advisory Committee (B): Board Member (O): Other Off label use of products will not be discussed in this presentation.")
4
CP1132959-6 6 prospective RCT 7,917 patients – PCI 1986-95 Assess outcome in thrombus vs no thrombus 2,752 with 5,165 without 6 prospective RCT 7,917 patients – PCI 1986-95 Assess outcome in thrombus vs no thrombus 2,752 with 5,165 without No CAT 66% CAT 34% Angiographic Trials’ Pool Singh et al: JACC 38(3):624, 2001
:624, 2001")
5
In-Hospital Adverse Outcome Thrombus Patients CP1132959-3 All patientsChi-squareP MI8.10.004 Death/MI 7.250.007 Excluding pt with only vein grafts MI 5.110.024 Death/MI 4.830.028 All patientsChi-squareP MI8.10.004 Death/MI 7.250.007 Excluding pt with only vein grafts MI 5.110.024 Death/MI 4.830.028

6
6-Month Survival After AMI Thrombus vs Nonthrombus Lesions Probability of survival Days to 6-month MI Nonthrombus Thrombus

7
Things That Didn’t Work

8
TEC Device Acolysis Device

9
The EMERALD Trial Enhanced Myocardial Efficacy and Removal by Aspiration of Liberated Debris AMI <6° (N=500) Primary or rescue PTCA Native coronary or SVG PercuSurge eligible 2.5 - 6.0 mm vessel 2.5 - 6.0 mm vessel GpIIb/IIIa optional Cath lab 3rdgeneration 3rd generation0.028” PercuSurge distal protection PCI with PCIwithoutprotection 1º Endpoints Resolution of ST segment elevation Infarct size by tc-99m-sestamibi 2º Endpoints 2º Endpoints Myocardial blush MACE No shock
 Primary or rescue PTCA Native coronary or SVG PercuSurge eligible mm vessel mm vessel GpIIb/IIIa optional Cath lab 3rdgeneration 3rd generation0.028 PercuSurge distal protection PCI with PCIwithoutprotection 1º Endpoints Resolution of ST segment elevation Infarct size by tc-99m-sestamibi 2º Endpoints 2º Endpoints Myocardial blush MACE No shock")
10
EMERALD ST Resolution Stone G, ACC 2004 Primary endpoint

11
EMERALD Final Infarct Size (99Tc-SPECT Scan) Stone G, ACC 2004 P=0.09 P=0.26 P=0.28
 Stone G, ACC 2004 P=0.09 P=0.26 P=0.28")
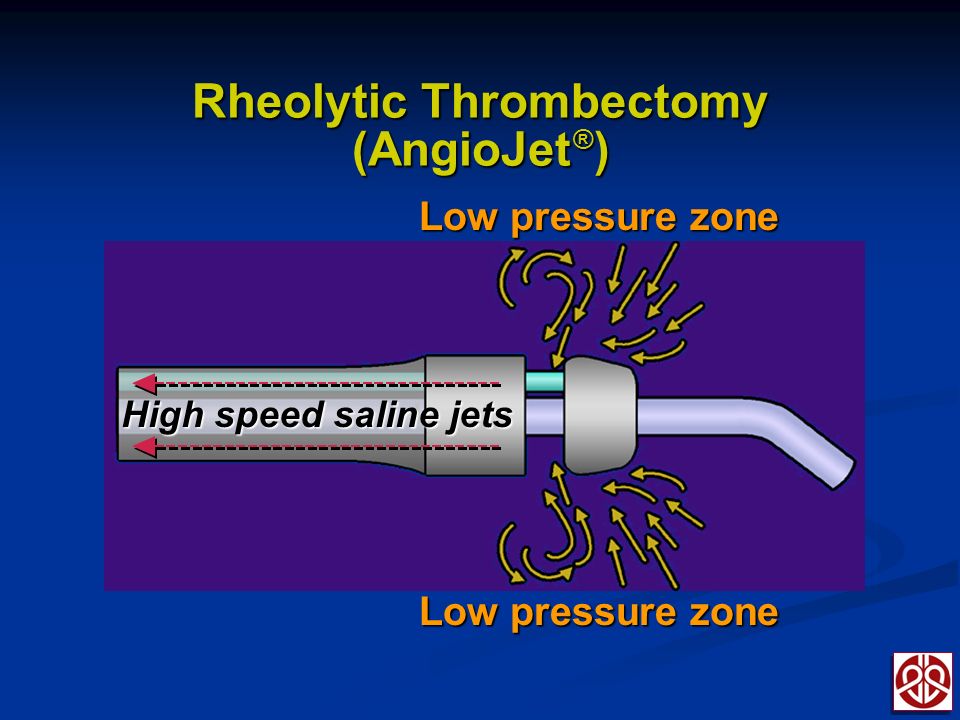
13
The AIMI Trial AngioJet Rheolytic Thrombectomy In Patients Undergoing Primary Angioplasty for Acute Myocardial Infarction AMI <6° (N=480) Primary PTCA Native coronary AngioJet eligible Culprit vessel >2mm Culprit vessel >2mm GpIIb/IIIa optional Cath lab AngioJet Rheolytic thrombectomy PCI with PCIwithoutthrombectomy 1º Endpoint Infarct size by tc-99m-sestamibi 2º Endpoints 2º Endpoints ST segment resolution Myocardial TIMI flow & blush LVEFMACE No shock
 Primary PTCA Native coronary AngioJet eligible Culprit vessel >2mm Culprit vessel >2mm GpIIb/IIIa optional Cath lab AngioJet Rheolytic thrombectomy PCI with PCIwithoutthrombectomy 1º Endpoint Infarct size by tc-99m-sestamibi 2º Endpoints 2º Endpoints ST segment resolution Myocardial TIMI flow & blush LVEFMACE No shock")
14
AiMI Trial Final Infarct Size 99Tc-SPECT From www.medscape.com, accessed 12/4/08www.medscape.com

15
Comparison of AngioJET Rheolytic Thrombectomy Before Direct Infarct Artery STENTing with Direct Stenting Alone in Patients with Acute Myocardial Infarction: the JETSTENT trial David Antoniucci on behalf of the JETSTENT Investigators

16
Co-Principal Investigators David Antoniucci, MD; Florence Antonio Colombo, MD; Milan Clinical Event Adjudication Committee Issam Moussa, M.D., Weill Cornell Medical Center, NYC Gian Battista Danzi, M.D., Ospedale Maggiore, University of Milan, Milan Carlo Di Mario, M.D., PhD, Royal Brompton Hospital, London Data Management and Monitoring Director: Maria Cristina Jori, M.D. Mediolanum Cardio Research, Milan ECG Core Laboratory Serenella Castelvecchio, M.D. Mediolanum Cardio Research, Milan Angiographic Core Laboratory Maria Antonietta Bonardi, M.D. Mediolanum Cardio Research, Milan Nuclear Scan Core Laboratory Prof. Roberto Sciagrà, University of Florence, Florence Steering Committe D Antoniucci, A Colombo, F-J Neumann, A Rodriguez, A Stabile, J Gustafson Sponsor: Medrad Interventional/Possis

17
After angiography and IRA wiring: thrombus grade 3 to 5 Pts with STEMI admitted within 12 hours from symptom onset Lysis Stroke < 30 days Surgery < 6 weeks Pre-stented IRA Rheolytic Thrombectomy +DSDirect Stenting (DS) Study Design Randomization 1:1 N = 500
 Study Design Randomization 1:1 N = 500")
18
Technique for AngioJet Use and DS Single pass anterograde technique (activate AngioJet proximal to thrombus) Angiographic check after first AngioJet pass. Temporary pacemaker strongly discouraged. Balloon pre-dilation strongly discouraged. DS had to be attempted in all cases in both arms. Routine Abciximab in both arms.

19
JETSTENT TRIAL Primary surrogate end points: Early ST-segment resolution (≥ 50% ST segment elevation reduction at 30 minutes) Infarct size (1-month 99m Tc sestamibi scintigraphy) Clinical end points: MACE at 1, 6, and 12 months Death and Readmission for CHF at 12 months Secondary surrogate end points: TIMI flow, cTFC, and TIMI blush
 Infarct size (1-month 99m Tc sestamibi scintigraphy) Clinical end points: MACE at 1, 6, and 12 months Death and Readmission for CHF at 12 months Secondary surrogate end points: TIMI flow, cTFC, and TIMI blush")
20
Baseline Angiographic Characteristics RTDS n=256 n=245 p value Multivessel disease114 (44)95 (39).192 IRA.483 LAD107 (42)91 (37) RCA112 (44)120 (49) LCx37 (14)34 (14) RVD (mm)2.94 [2.67-3.24] 2.91 [2.62-3.25].670 Pre-wiring TIMI flow 0-1212/254 (83.5)203/242 (83.9).899 Post-wiring TIMI flow 0-1 142/231 (61.5) 129/222 (58.1).465 Thrombus grade.640 1-23 (1.4)3 (1.4) 373 (32.5)80 (37.4) 483 (37.4)79 (36.9) 563 (28.4)52 (24.3)
![Baseline Angiographic Characteristics RTDS n=256 n=245 p value Multivessel disease114 (44)95 (39).192 IRA.483 LAD107 (42)91 (37) RCA112 (44)120 (49) LCx37 (14)34 (14) RVD (mm)2.94 [ ] 2.91 [ ].670 Pre-wiring TIMI flow /254 (83.5)203/242 (83.9).899 Post-wiring TIMI flow /231 (61.5) 129/222 (58.1).465 Thrombus grade (1.4)3 (1.4) 373 (32.5)80 (37.4) 483 (37.4)79 (36.9) 563 (28.4)52 (24.3)](http://images.slideplayer.com/35/10379199/slides/slide_20.jpg "Baseline Angiographic Characteristics RTDS n=256 n=245 p value Multivessel disease114 (44)95 (39).192 IRA.483 LAD107 (42)91 (37) RCA112 (44)120 (49) LCx37 (14)34 (14) RVD (mm)2.94 [ ] 2.91 [ ].670 Pre-wiring TIMI flow /254 (83.5)203/242 (83.9).899 Post-wiring TIMI flow /231 (61.5) 129/222 (58.1).465 Thrombus grade (1.4)3 (1.4) 373 (32.5)80 (37.4) 483 (37.4)79 (36.9) 563 (28.4)52 (24.3)")
21
RTDS n=256n=245 p value ER-PCI (min)34 [15-67]31 [18-60].727 Procedural time (min) 59.5 [44.7-70] 46 [35-60] <.001 Predilation before RT5/246 (2) TIMI flow 3 after RT159/ 222 (72) Predilation before stenting25 (9.8)34 (13.9).149 Stent per pt 1.26 ± 0.541.40 ± 0.73.022 Mean stent length (mm) 23.7 ± 10.925.9 ± 14.1.050 Abciximab249 (97)239 (98).841 Procedural success237 (93)229 (93).696 Procedural Characteristics
![RTDS n=256n=245 p value ER-PCI (min)34 [15-67]31 [18-60].727 Procedural time (min) 59.5 [ ] 46 [35-60] <.001 Predilation before RT5/246 (2) TIMI flow 3 after RT159/ 222 (72) Predilation before stenting25 (9.8)34 (13.9).149 Stent per pt 1.26 ± ± Mean stent length (mm) 23.7 ± ± Abciximab249 (97)239 (98).841 Procedural success237 (93)229 (93).696 Procedural Characteristics](http://images.slideplayer.com/35/10379199/slides/slide_21.jpg "RTDS n=256n=245 p value ER-PCI (min)34 [15-67]31 [18-60].727 Procedural time (min) 59.5 [ ] 46 [35-60] <.001 Predilation before RT5/246 (2) TIMI flow 3 after RT159/ 222 (72) Predilation before stenting25 (9.8)34 (13.9).149 Stent per pt 1.26 ± ± Mean stent length (mm) 23.7 ± ± Abciximab249 (97)239 (98).841 Procedural success237 (93)229 (93).696 Procedural Characteristics")
22
Surrogate Endpoints RT DS p value n=246n=240 STR ≥ 50% at 30 min 211 (85.8)189 (78.8).043 n=217n=208 Infarct Size (%)11.8 [3.1-23.7] 12.7 [4.7-23.3].398 n=252n=241 Final TIMI 3 flow 203 (80.6) 207 (85.9).113 n=228n=216 cTFC 20 [15.0-27.2] 20 [14.0-25.7].357 n=215n=211 Blush grade.207 0-117 (8)11 (5) 243 (20)33 (16) 3 155 (72)167 (79)
![Surrogate Endpoints RT DS p value n=246n=240 STR ≥ 50% at 30 min 211 (85.8)189 (78.8).043 n=217n=208 Infarct Size (%)11.8 [ ] 12.7 [ ].398 n=252n=241 Final TIMI 3 flow 203 (80.6) 207 (85.9).113 n=228n=216 cTFC 20 [ ] 20 [ ].357 n=215n=211 Blush grade (8)11 (5) 243 (20)33 (16) (72)167 (79)](http://images.slideplayer.com/35/10379199/slides/slide_22.jpg "Surrogate Endpoints RT DS p value n=246n=240 STR ≥ 50% at 30 min 211 (85.8)189 (78.8).043 n=217n=208 Infarct Size (%)11.8 [ ] 12.7 [ ].398 n=252n=241 Final TIMI 3 flow 203 (80.6) 207 (85.9).113 n=228n=216 cTFC 20 [ ] 20 [ ].357 n=215n=211 Blush grade (8)11 (5) 243 (20)33 (16) (72)167 (79)")
23
One-Month Outcome P = 0.050

24
6-Month Outcome RT DS

25
Conclusions AngioJet rheolytic thrombectomy before direct IRA stenting as compared to direct stenting alone is associated with: o Better myocardial reperfusion (higher rate of early STR) o Improved 6-month clinical outcome (lower MACE rate) The results of the JETSTENT trial support the routine use of AngioJet rheolytic thrombectomy in AMI patients with evidence of thrombus.
 o Improved 6-month clinical outcome (lower MACE rate) The results of the JETSTENT trial support the routine use of AngioJet rheolytic thrombectomy in AMI patients with evidence of thrombus.")
26
Added Security

27
What’s Really Made A Difference

29
TAPAS Trial Design

30
TAPAS Myocardial Blush Grade

31
TAPAS ST Segment Resolution

32
TAPAS Cardiac Death At One Year

33
TAPAS Cardiac Death or Non-fatal MI At One Year

34
Meta-analysis of Aspiration Thrombectomy Device Use Mortality at 30 Days De Luca G, Eur Heart J 2008 (Sept e-publication)
")
35
Meta-analysis of Aspiration Thrombectomy Device Use De Luca G, Eur Heart J 2008 (Sept e-publication)
")
36
Meta-analysis Of Distal Protection Or Thrombectomy Device Use Stone et al: Circulation 2008; 118:552

37
Treatment of Thrombus Containing Lesions Thrombotic lesions have increased risk Thrombotic lesions have increased risk Adjunctive devices largely disappointing Adjunctive devices largely disappointing May be some benefit for rheolytic thrombectomy in bulky thrombus May be some benefit for rheolytic thrombectomy in bulky thrombus Aspiration thrombectomy as routine adjunct to thrombotic lesions is standard of care for ACS/STEMI Aspiration thrombectomy as routine adjunct to thrombotic lesions is standard of care for ACS/STEMI

Similar presentations



















: 934-43 Within the past 12 months, our institution has had a financial.>")
