Download presentation
Presentation is loading. Please wait.

1
Mississippi Association of Grantmakers January 9, 2015

3
Heart Disease Death Rate - Mississippi Rank Among States 2012 - of 50 2012 - 1 st of 50 (1= highest ) Source: National Center for Health Statistics Alabama– 2 nd Alabama – 2 nd
 Source: National Center for Health Statistics Alabama– 2 nd Alabama – 2 nd")
4
Accident Death Rate – Mississippi (unintentional injury) Rank Among States 2012 - of 50 2012 - 5 th of 50 (1= highest ) Source: National Center for Health Statistics West Virginia – 1st New Mexico – 2 nd Kentucky – 3 rd Oklahoma – 4 th
 Rank Among States of th of 50 (1= highest ) Source: National Center for Health Statistics West Virginia – 1st New Mexico – 2 nd Kentucky – 3 rd Oklahoma – 4 th")
5
Motor Vehicle Accident Death Rate – Mississippi Rank Among States 2012 - of 50 2012 - 1 st of 50 (1= highest ) Source: National Center for Health Statistics
 Source: National Center for Health Statistics")
6
Cancer Death Rate - Mississippi Rank Among States 2012 - 2 nd of 50 (1= highest ) Source: National Center for Health Statistics Kentucky- 1 st Kentucky - 1 st
 Source: National Center for Health Statistics Kentucky- 1 st Kentucky - 1 st")
8
Adult American Smokers - 2013 U.S. Adults 19.0% Smokers

9
Adult Mississippi Smokers - 2013 Non-Smokers 24.8% Smokers Source: CDC: Behavioral Risk Factor Surveillance System (BRFSS)
")
10
Adult Smoking Rate - Mississippi Rank Among States 2013 - 4 th* of 50 (1= highest ) Source: CDC: Behavioral Risk Factor Surveillance System (BRFSS) West Virginia 1 st Kentucky 2 nd Arkansas – 3 rd
 Source: CDC: Behavioral Risk Factor Surveillance System (BRFSS) West Virginia 1 st Kentucky 2 nd Arkansas – 3 rd")
11
MS Public Schools Current Smokers, 1998 – 2012* *Mississippi Youth Tobacco Survey

12
MS Public Schools Current Smokers, 1998 - 2012

13
35.1% Obesity, United States - 2013 Obesity, United States - 2013 29.4% 21.3 % Source: Behavioral Risk Factor Surveillance System, CDC 35.1% 34.6%

14
7 4 8# 10 1 8 1 State Rank, Obesity - 2013 Top Ten Source: Behavioral Risk Factor Surveillance System, CDC * = tied 5 6 3 9

15
7 4 10 1 8 1 Obesity, US, 2013 States with >30% Obesity Obesity, US, 2013 States with >30% Obesity Source: Behavioral Risk Factor Surveillance System, CDC 5 6 3 9

16
9.7% Adults with Diagnosed Diabetes - 2012 12.5% 13.0% 7.0%

17
3* State Rank, Diagnosed Diabetes - 2012 Top Ten States * = tied 2 1 5 7 8 3* 10 6 9

18
3* State Rank, Diagnosed Diabetes - 2012 States With >10% Diabetes * = tied 2 1 5 7 8 3* 10 6 9

20
Infant Mortality Rate - Mississippi Rank Among States 2012 - 2 nd of 50 (1= highest ) Source: National Center for Health Statistics, Deaths: Final Data for 2010. NVSR Volume 61, Number 4, May 8, 2013

21
8.9 8.8 Infant Mortality, 2012 Infant Mortality, 2012 Deaths per 1000 Live Births 6.0 Source: National Center for Health Statistics, Deaths: Final Data for 2012.

22
Mississippi Infant Mortality, by Year, 1997 - 2013 *US IM 2010: 6.1

23
Mississippi Infant Mortality, by Year, 1997 - 2013 *US IM 2010: 6.1

24
2005 2004 2003 2002 2001 20001999 1998 Infant Mortality – State Rank (1=worst) 2006 2007 2008 ■#1 2009 2010 20112012
 ■#")
25
Teen Birth Rate - Mississippi Rank Among States 2012 - 3 rd of 50 (1= highest ) Source: National Center for Health Statistics, Births: Final Data for 2012 NVSR Volume 62, Number 9, December, 2013. http://www.cdc.gov/nchs/data/nvsr/nvsr62/nvsr62_09.pdf New Mexico – 1 st Oklahoma – 2nd

26
Infant Deaths by Age of Mother Mississippi, 2013 Mother 20 & Older 322 (86.3%) Teenage Mother Mother 50 (13.4%) Total infant deaths, 373
 Teenage Mother Mother 50 (13.4%) Total infant deaths, 373")
27
Infant Deaths by Birthweight Mississippi, 2013 Very Low Birthweigh t 183 (49.1%) LowBirthweight 70 (18.7%) NormalBirthweight 119 (31.9%) Total infant deaths, 373
 LowBirthweight 70 (18.7%) NormalBirthweight 119 (31.9%) Total infant deaths, 373")
28
Low Birthweight - Mississippi Rank Among States 2012 - 1 st of 50 (1= highest ) Source: National Center for Health Statistics, Births: Final Data for 2011. NVSR Volume 62, Number 1, June, 2013. http://www.cdc.gov/nchs/data/nvsr/nvsr62/nvsr62_01_tables.pdf

29
Very Low Birthweight - Mississippi Rank Among States 2012 - 1 st of 50 (1= highest ) Source: National Center for Health Statistics, Births: Final Data for 2011. NVSR Volume 62, Number 1, June, 2013. http://www.cdc.gov/nchs/data/nvsr/nvsr62/nvsr62_01_tables.pdf

31
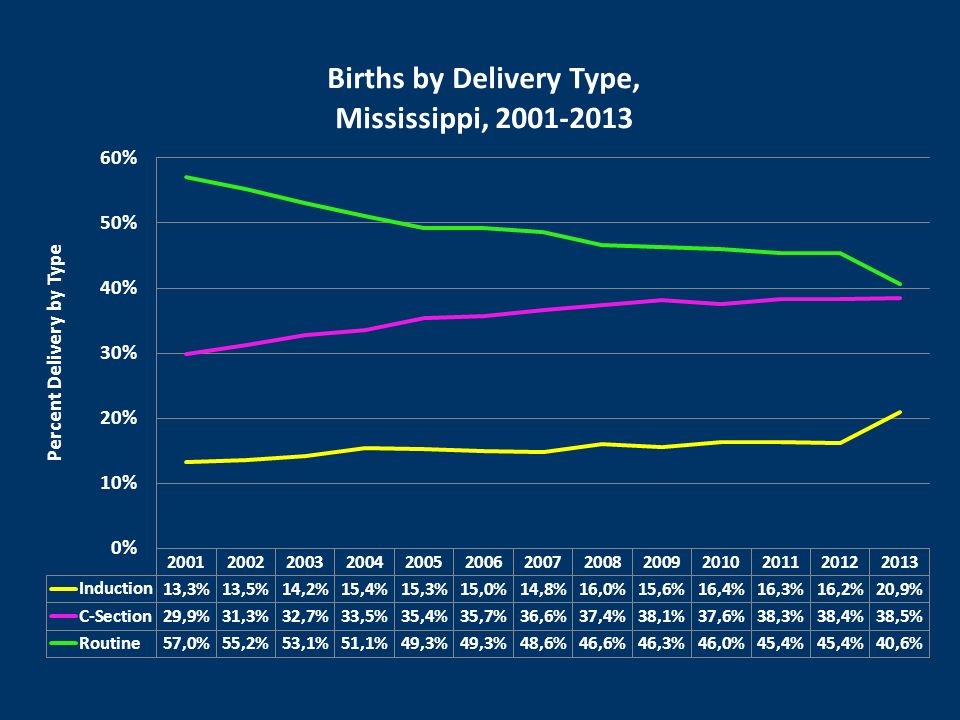
% of Total Births of Known Gestational Age Year of Birth Births by Gestational Age, by Year Mississippi

32
% Early Term (37 – 38 Weeks) Deliveries, Mississippi, 2011 – 2014, by Quarter
 Deliveries, Mississippi, 2011 – 2014, by Quarter")
35
Number of Reported Cases of HIV Disease, Mississippi, 2000 - 2013

36
HIV Disease Reported by Race/Ethnicity, Mississippi, 2013

37
Note. Data include persons with a diagnosis of HIV infection regardless of stage of disease at diagnosis. a) Includes data from areas with confidential name-based HIV infection reporting since at least January 2006. Estimated numbers resulted from statistical adjustment that accounted for reporting delays, but not for incomplete reporting. Rates are per 100,000. http://www.cdc.gov/hiv/pdf/statistics_2011_HIV_Surveillance_Report_vol_23.pdf#Page=68
 Includes data from areas with confidential name-based HIV infection reporting since at least January Estimated numbers resulted from statistical adjustment that accounted for reporting delays, but not for incomplete reporting. Rates are per 100,")
39
Tuberculosis Case Rates, by year, MS vs US

41
Source Data: US data1976-2010 CDC MS data 1976-2011 CDC, 2012, MSDH

42
Less than the national average rate for the first time since 2006

43
What do these health indicators have in common High infant mortality High death rates from heart disease, cancer, injuries High rates of smoking and obesity Low rates of physical activity and healthy eating

44
Social Determinants of Health Health is related to –Education –Economic stability –Neighborhood and the built environment –Health and health care –Social and Community Context

45
Social Determinants of Health Health is related to –Education: high school graduation, enrollment in higher education, language and literacy, early childhood education and development –Economic stability: poverty, employment, food security, housing stability

46
Social Determinants of Health Health is related to –Neighborhood and the built environment: access to healthy foods, quality of housing, crime and violence, environmental conditions –Health and health care –Health and health care: access to health care, access to primary care, health literacy –Social and community context –Social and community context: social cohesion, civic participation, perceptions of discrimination and equity, incarceration/institutionalization

47
National Prevention Strategy

48
Economic Benefits of Preventing Disease Disease can cause significant economic burdens to the economy, families, and businesses through lost productivity and health care costs; Prevention can reduce significant economic burden of disease as well as improve the length and quality of people’s lives; Prevention: can be cost-effective, reduce health care costs, and improve productivity.

49
Economic Benefits of Preventing Disease Examples – lowering health care costs: –A 5 percent reduction in the prevalence of hypertension would save $25 billion in 5 years. 323 –Annual health care costs are $2,000 higher for smokers, $1,400 higher for people who are obese, and $6,600 higher for those who have diabetes than for nonsmokers, people who are not obese, or people do not have diabetes. 324

50
Economic Benefits of Preventing Disease Examples – lowering health care costs: –Increasing use of preventive services, including tobacco cessation screening, alcohol abuse screening and aspirin use, to 90 percent of the recommended levels could save $3.7 billion annually in medical costs. 326 –Medical costs are reduced by approximately $3.27 for every dollar spent on workplace wellness programs, according to a recent study. 327 –For every HIV infection prevented, an estimated $355,000 is saved in the cost of providing lifetime HIV treatment. 319

51
Economic Benefits of Preventing Disease Examples – increasing productivity: –Asthma, high blood pressure, smoking, and obesity each reduce annual productivity by between $200 and $440 per person. 333 –Workers with diabetes average two more work days absent per year than workers without diabetes. 334 –Absenteeism costs are reduced by approximately $2.73 for every dollar spent on workplace wellness programs, according to a recent study. 327

52
Direction of the Health Department History: –Inside the clinic walls –One patient at a time Include prevention in clinic interactions –Safe sleep –Smoking cessation –Early elective deliveries –Nutrition education, etc.

53
Direction of the Health Department Move outside those clinic walls, back the community –Include non-traditional partners (but don’t leave the traditional partners behind) –Promote health as a consideration in all policies
 –Promote health as a consideration in all policies")
54
Partners Traditional partners: –health care providers and facilities, –non-profit health agencies Plus: –Schools –Faith-Based Organizations –Employers –City planners, –Elected officials –Economic development groups –Any other organization that is interested in improving the health and quality of life for Mississippi residents –All Mississippi residents

55
Direction of the Health Department Examples –Mayors’ Health Councils Joint use agreements, smoke free air, sidewalks and street lights required, farmer’s markets –Congregational nurses Health screenings, improved nutritional foods, safe sleep education for families (grandmothers seem to be important!), these congregations form a network –Mississippi Perinatal Quality Collaborative Hospitals, providers, insurers, March of Dimes, public health working together to improve perinatal outcomes
, these congregations form a network –Mississippi Perinatal Quality Collaborative Hospitals, providers, insurers, March of Dimes, public health working together to improve perinatal outcomes")
57
The town of Arcola received donated land, a mini grant, and raised funds to begin a new children and adult softball league

59
Direction of the Health Department Examples –Tobacco coalitions Increasing comprehensive smoke free air ordinances in communities and counties statewide –Assuring day care regulations are healthy Physical activity requirements Screen time Healthy meals and snacks –Diabetes self management education – Group meetings to provide education and support for better diabetes control and prevention of complications

62
healthy foods, an example Policy: assuring policies (e.g., tax policies, EBT card policies, zoning, school nutrition policies) friendly to grocery stores, farmer’s markets, gas stations with a healthy food isle. Environment: assuring improved access to healthy foods such as farmers’ markets placement, less access to vending machines and school stores with junk food Systems: to include easy access to prevention/screening and nutrition education/healthy cooking education

63
MSDH must change with the times to meet the needs of the state and improve health. The Bower Foundation is helping us do it!

64
Thank you

65
Funding Request for Infant Mortality Reduction Priority areas Preconception health – improving health before pregnancy 17 Hydroxyprogesterone (17 P) - access to weekly hormone injection that decreases repeat preterm deliveries Premature elective deliveries – reducing non-medically indicated deliveries before 39 weeks gestation Maternal smoking – smoking cessation and limiting secondhand smoke exposure among pregnant women Safe sleep environment for infants - infants should sleep alone, in a crib, on their back, in a smoke free environment Systems for risk based perinatal care – getting the mom to the right place to deliver in the shortest amount of time
 - access to weekly hormone injection that decreases repeat preterm deliveries Premature elective deliveries – reducing non-medically indicated deliveries before 39 weeks gestation Maternal smoking – smoking cessation and limiting secondhand smoke exposure among pregnant women Safe sleep environment for infants - infants should sleep alone, in a crib, on their back, in a smoke free environment Systems for risk based perinatal care – getting the mom to the right place to deliver in the shortest amount of time")
66
Funding Request for Infant Mortality Reduction Address the target areas through –Strengthening surveillance and data analysis capacity –Building capacity through training, public private collaboration, and community engagement Among health care providers Among policy makers at all levels (especially homes, hospitals and communities) Among the public
 Among the public")
67
Funding Request for Infant Mortality Reduction Priority areas

68
Fiscal Year 2016 Requested Increase Purpose Requested Services: Maternity Early Intervention 1,020,800 4,789,937 Infant Mortality Task Force Initiative1,512,385 Admin: New Lab Support Patient/Insurance Billing System State MAGIC Fin. Fee Increase 560,000 1,000,000 551,214 Personnel: Pos/Reclass/Reallo/Benchmark7,495,169 Phase I Underwood Building Renovation SRF Match 5,200,000 1,800,000 Medicaid Patient Managed Care Reimb.3,226,000 27,155,506

69
69 Public & Provider Education SyphilisSyphilisTuberculosisTuberculosisHIV/AIDSHIV/AIDS Control

70
70 SyphilisSyphilisTuberculosisTuberculosisHIV/AIDSHIV/AIDS Control Case/Contact Intervention Rapid identification of cases Intensive case interviews Locate and evaluate contacts often with limited locating information Prevent contacts from transmitting Rapid identification of cases Intensive case interviews Locate and evaluate contacts often with limited locating information Prevent contacts from transmitting

72
Your first line of defense.

73
FY 15 Budget $365 million Employees 2,208 District Offices 9 County Offices 104 WIC Dist. Centers 95 Home Health Offices 0 Mississippi State Department of Health

74
Public Health Accreditation Prerequisites for accreditation: – State health assessment – State health improvement plan – MSDH strategic plan

75
10 Essential Public Health Services

76
School Immunization Law Miss. Code Ann. § 41-23-37 Medical exemptions No religious exemptions (48 states allow them)– declared unconstitutional by the MS Supreme Court Philosophical exemptions –(18 states have them) – Many states with philosophical exemptions now have more measles and more pertussis
– declared unconstitutional by the MS Supreme Court Philosophical exemptions –(18 states have them) – Many states with philosophical exemptions now have more measles and more pertussis.")
Similar presentations