Download presentation
Presentation is loading. Please wait.

1
When Children Die Gary D. Ceneviva, MD Penn State Children’s Hospital Division of Pediatric Critical Care

2
Introduction Over 50,000 children die annually in the United States 1 Approximately 500,000 children cope with life-threatening conditions annually in the United States 2 1. Arias E. et al. Pediatrics 2003;112:1215 2. Himelstein BP et al. N Eng J Med 2004;350:1752

3
Introduction Between 1997-2001, an average of 2,060 children less than age 19 die annually in Pennsylvania 1 Approximately 480 deaths occur annually in the PSCH primary and secondary service regions 2. PA Department of Health

4
Definitions Hospice – Describes a philosophy, program, or site of care – A philosophy of care which addresses the physical, social, emotional, and spiritual needs of children and adolescents with life threatening conditions and their families from the time of diagnosis, through bereavement, if cure is not attained

5
Hospice Describes a philosophy, program, or site of care A philosophy of care which addresses the physical, social, emotional, and spiritual needs of children and adolescents with life- threatening conditions and their families from the time of diagnosis, through bereavement, if cure is not attained

6
Definitions Palliative Care – Intervention that focuses on the reduction or abatement of physical and emotional symptoms of children with life threatening illnesses and their families – Can be provided concurrently with curative or life-prolonging care

7
Palliative Care Intervention that focuses on the reduction or abatement of physical and emotional symptoms of children with life threatening illnesses and their families Can be provided concurrently with curative or life-prolonging care

8
Definitions End-of-Life Care – Focuses on preparing for an anticipated death and managing the end stage of a fatal medical condition

9
End-of-Life Care Focuses on preparing for an anticipated death and managing the end stage of a fatal medical condition

10
Definitions Life-Threatening Conditions – Carry a substantial probability of death in childhood – Perceived as having a fatal outcome

11
Life-Threatening Conditions Carry a substantial probability of death in childhood Perceived as having a fatal outcome

14
Unique Features of Pediatric Palliative Care 1 Life-threatening conditions and causes of death differ within childhood, adolescence, and adulthood Life-threatening conditions can be rare resulting in an uncertain prognosis Developmentally, infants, children and adolescents have distinctive concerns and needs Infants, children, and adolescents express their concerns, needs, feelings, and beliefs differently

15
Unique Features of Pediatric Palliative Care 1 Ethical and legal issues of decision making Role of significant others in patient a child or adolescents death Nature and duration of bereavement following death Effects of the dying process and death of a child on health care providers 1. Papadatou D et al. Education and Training Curriculum for Pediatric Palliative Care. Alexandria, Va.: Children's International project on Palliative/Hospice Services, NHPCO, 2003

16
Distinctive features of Pediatric Palliative Care 1 The nature of life-threatening conditions & causes of death in children and adolescents The unusual features of some life-threatening conditions in childhood The nature of concerns and needs of dying infants, children, & adolescents Distinctive ways in which infants, children, & adolescents express their concerns and needs Unique issues of decision making, as well as ethical and legal issues, of self determination

17
Distinctive features of Pediatric Palliative Care 1 The role of significant others in patient care Populations and individuals affected by a death Distinctive aspects of the nature and duration of bereavement following death Effect of the dying process and death of a child on health care professionals and care providers 1. Papadatou D et al. Education and Training Curriculum for Pediatric Palliative Care. Alexandria, Va.: Children's International project on Palliative/Hospice Services, NHPCO, 2003

18
Leading Causes of Infant Death Congenital & Chromosomal Anomalies Disorders related to SGA & LBW SIDS Maternal Complications of Pregnancy Complications of Placenta, Cord & Membranes Respiratory Distress Accidents Bacteria Sepsis Diseases of the Circulatory System Intrauterine Hypoxia & Birth Asphyxia Arias E. et al. Pediatrics 2003;112:1215

19
Leading Causes of Death (1-19 years) Arias E et al. Pediatrics 2003;112:1215
 Arias E et al. Pediatrics 2003;112:1215")
20
Leading Causes of Childhood Death (1-19 years) Accidents (unintentional injuries) Assault (homicide) Malignant Neoplasms Intentional Self Harm (suicide) Congenital & Chromosomal Anomalies Diseases of Heart Influenzae and Pneumonia Septicemia Chronic Lower Respiratory Diseases In situ, Benign, or neoplasms of uncertain behavior Arias E et al. Pediatrics 2003;112:1215

21
Conditions Appropriate for Palliative Care Conditions for which curative treatment is possible but may fail (Cancer) Conditions requiring long-term treatment aimed a maintaining the quality of life (Cystic Fibrosis) Progressive conditions in which treatment is exclusively palliative after diagnosis (Trisomy 13) Conditions involving severe, nonprogressive disability (Hypoxic Brain Injury) Himelstein BP et al. N Engl J Med 2004;350:1752

22
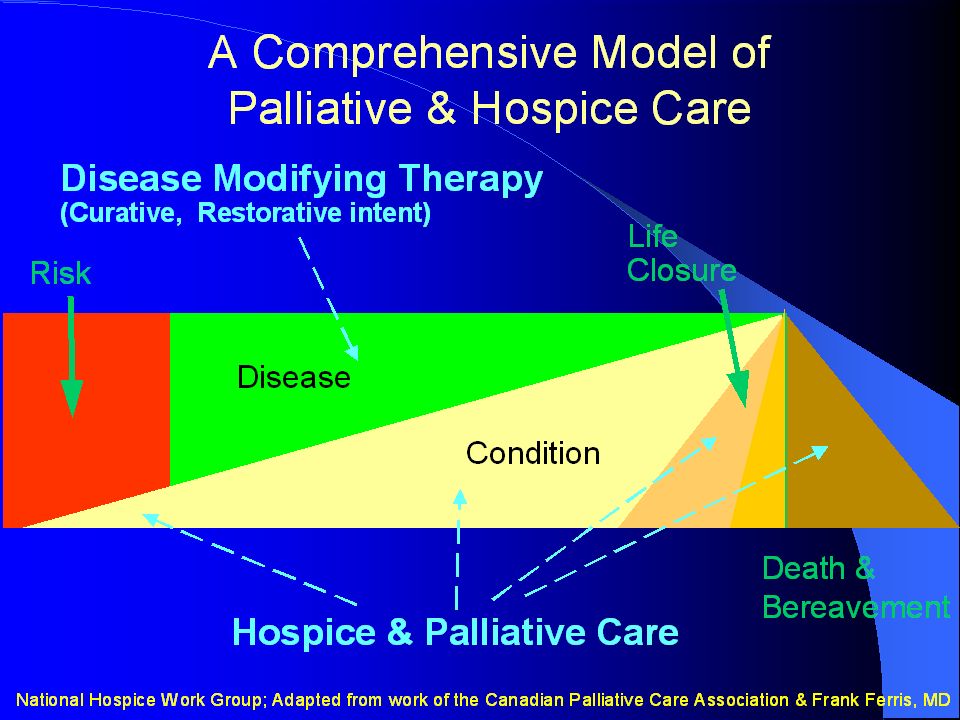
American Academy of Pediatrics Recommendations Palliative & respite programs need to be developed & available An integrated model of palliative care should be offered at diagnosis & continued throughout the course of illness regardless of the outcome Changes in regulation & reimbursement of palliative and hospice services are necessary

23
American Academy of Pediatrics Recommendations All general & subspecialty pediatricians need to become familiar and comfortable with the provision of palliative care An increase in support for research is necessary Physician assisted suicide or euthanasia is not supported Palliative Care for Children Pediatrics 2000;106:351

24
Barriers Psychological Fragmented Health Care System Financial & Regulatory Ethical & Legal Research Educational

25
Psychological Decreased childhood mortality Perception that palliative or hospice care = death Discomfort with counseling or managing a child and family in palliative care Advanced technology can result in prognostic uncertainty or perception that death is a therapeutic misadventure Palliative Care for Children Pediatrics 2000;106:351 Himmelstein BP et al. N Eng J Med 2004;35:1752 Field MF, Behrman R, eds. When Children Die. Washington, D.C.: National Academies Press, 2003

26
Fragmented Care Children with complex medical problems often require inpatient, home, and community-based services from different professionals and, organizations which may be restricted geographically, institutionally, & financially

27
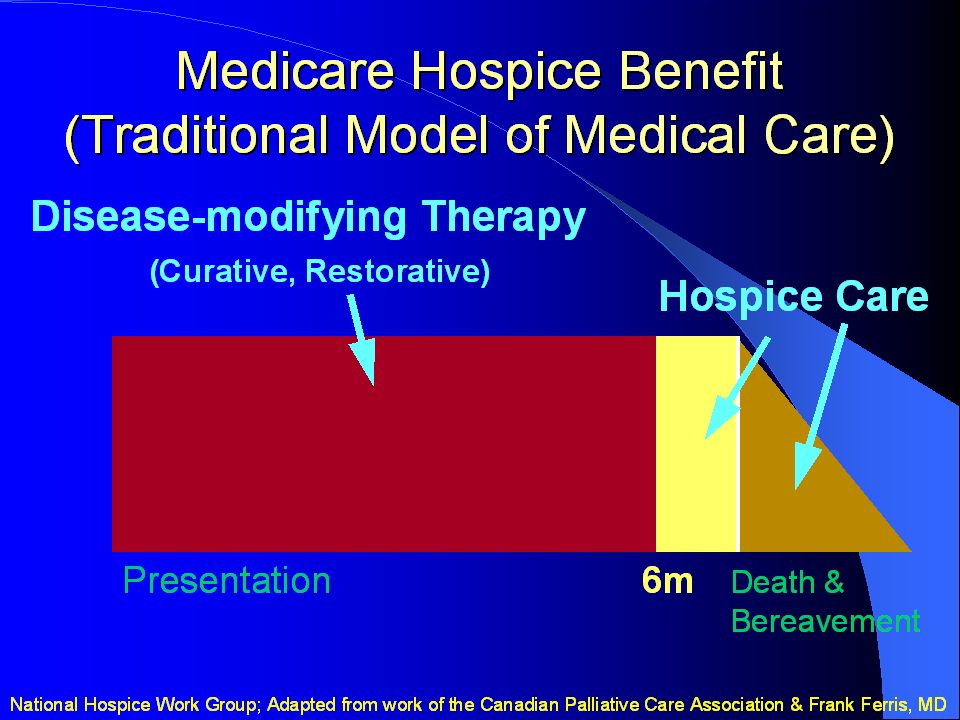
Financial and Regulatory Medicare Hospice Benefit – Limits care to patients with a life expectancy < 6 months – May require patients to forgo life prolonging or curative therapies Reimbursement for comprehensive palliative care & hospice services are often limited Palliative Care for Children Pediatrics 2000;106:351 Himmelstein BP et al. N Eng J Med 2004;35:1752 Field MF, Behrman R, eds. When Children Die. Washington, D.C.: National Academies Press, 2003

28
Legal & Ethical Decisions About who decides 1,2 – Appropriateness of surrogate decision making by parents About treatements 1,3 – When to start, limit, or stop medical interventions About the criteria for decisions 1 – Quality of life – Resources 1. Field MF, Behrman R, eds. When Children Die. Washington, D.C.: National Academies Press, 2003 2. Sabatino C. J Law Med Ethics 1999;27:297 3. Kunin H. Ethics Behav 1997;7(1):43
:43.")
29
Research Limited Systematic data are often not available Results in decision making about the care of children with little guidance documenting the potential burdens or benefits of medical interventions Field MF, Behrman R, eds. When Children Die. Washington, D.C.: National Academies Press, 2003

30
Educational Limited Training High Reliance on “Trial and Error” Limited Curricula or Formal Courses Limited Pediatric Palliative Care Specialists Collins JJ Hematol Oncol Clin North Am. 2002;16(3):657
:657.")
31
Education & Training in End- of-Life Care 228 Pediatric oncologists surveyed: – > 90 % reported a high reliance on “trial and error” – Only 10 % attended a formal course – Only 2 % rotated on a palliative care or hospice service Hilden JM et al. J Clin Oncol 2001;19:205

32
AAP Recommendations Residency, fellowships, and continuing education Programs should include topics on: – Palliative Medicine – Communication Skills – Grief and Loss – Managing prognostic uncertainty – Spiritual Care – Decision to forgo life sustaining medical treatment – Alternative medicine Palliative Care for Children Pediatrics 2000;106:351

33
Initiative for Pediatric Palliative Care (IPPC) Education and quality improvement effort Comprehensive, interdisciplinary curriculum which addresses knowledge, attitudes, & skills necessary to enhance family center care for children living with life-threatening conditions
 Education and quality improvement effort Comprehensive, interdisciplinary curriculum which addresses knowledge, attitudes, & skills necessary to enhance family center care for children living with life-threatening conditions")
34
IPPC Curriculum Six Modules – Engaging with Children and Families – Relieving Pain and Other Symptoms – Analyzing Ethical Challenges in Pediatric End-of-Life Decision Making – Responding to Suffering and Bereavement – Improving Communication and Strengthening Relationships – Establishing Continuity of Care

35
Engaging with Children and Families Need to pick a video and then facilitate a some of the questions

36
Educational Plans 2 Day Symposium 2 Symposia per year – October 12 th & 13 th, 2004 at the Harrisburg Wyndham Hotel October 12 th - Principles, Values, and Ethics of Pediatric Palliative Care October 13 th - Pain Assessment and Management – May 3 rd & 4 th, 2005 at the Hershey Lodge and Convention Center (tentative) May 3 rd – Palliative Care for Adolescence May 4 th – End-of-Life Care and Bereavement
 May 3 rd – Palliative Care for Adolescence May 4 th – End-of-Life Care and Bereavement")
37
Educational Objectives To obtain specialized knowledge in palliative, end-of-life, and bereavement care To acquire relevant technical and psychosocial skills To become aware of one’s feelings and thoughts towards death, dying, and bereavement To develop attitudes that will enable health care professionals to provide quality palliative care To develop strategies to enhance palliative care services offered by the Penn State Children's Hospital

38
Challenges Changing attitudes and practices are often difficult to achieve Educational reform is certainly not the solution to deficits in palliative and end-of- life care

39
Summary Children with life threatening conditions and their families often fail to receive care that meets their emotional, spiritual, and physical needs Current methods of organizing and financing palliative care limits the provision and coordination of these services Integrating effective palliative care from the time a child is diagnosed with a life threatening condition should improve care for both the children and their families

40
Summary Improving Palliative and Hospice care will require: – System changes not just individual changes – Research to increase our knowledge of what constitutes the best palliative, end-of-life, and bereavement care – Changes in attitudes, policies, and practice involving health care professionals and those who manage, finance, and regulate health care

Similar presentations