Download presentation
Presentation is loading. Please wait.

1
DIAGNOSIS, TREATMENT & MANAGEMENT OF TM JOINT UBC

3
TimeTopic 9.00 – 9.55 Embryology, Senses Primary Reflexes Anatomy of TM Joint, Muscles, Ligament, Fascia s & CV Joint 9:55 – 10.00 Trigeminal nerve 10:00– 10:15Break 10.15 – 10.45 Biomechanics of TMJ Cause, & Classifications of TMJ 10.45 – 12.00 Management of TMD 12:00- 1:00Lunch 1:00 – 3.00 Practical TMJ assessment 3.00– 3.10 break 3.10 – 5.00 Practical

5
Reflexes & Sensory processing Their influence on TMJ, posture & behaviour

6
EMBRYOLOGY AND CRANIAL NERVE LINKS Pharyngeal Arches- 5 & 20 weeks Trigeminal Facial Glossopharyn geal Vagus Art by Renee Peterson & John Chitty, based on Larsen, Human Embryology, p. 362

7
Cranium & TM Joint

8
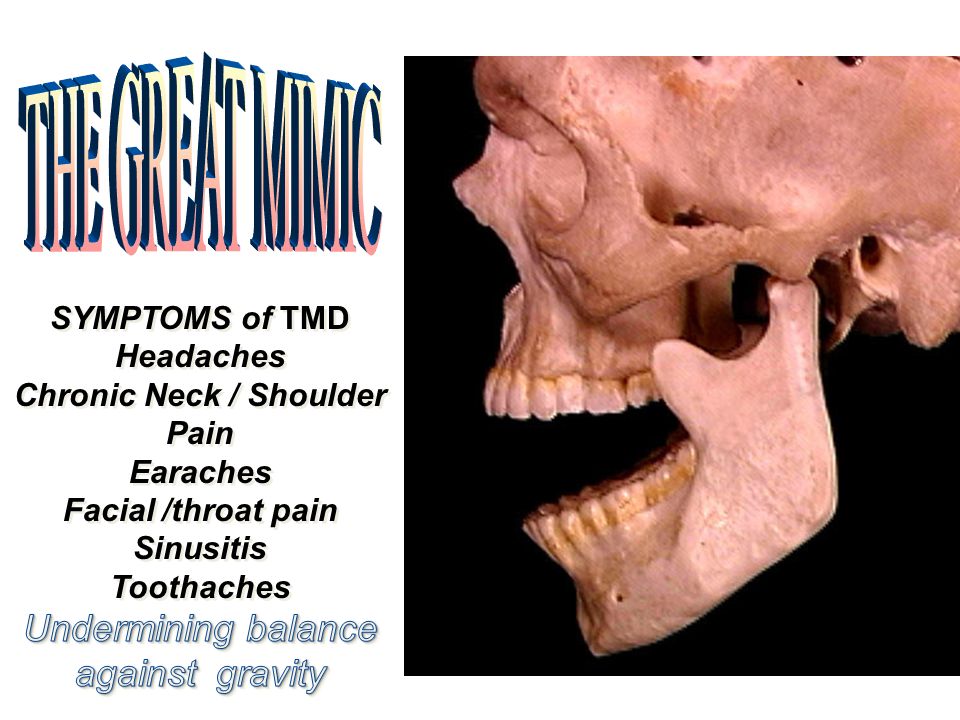
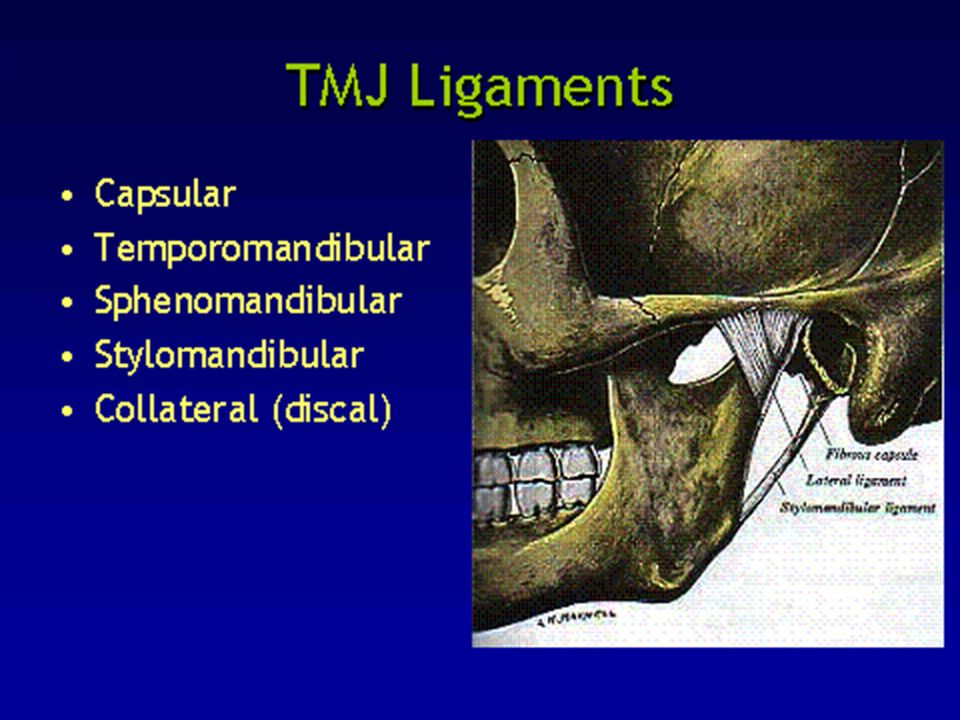
TM JOINT

11
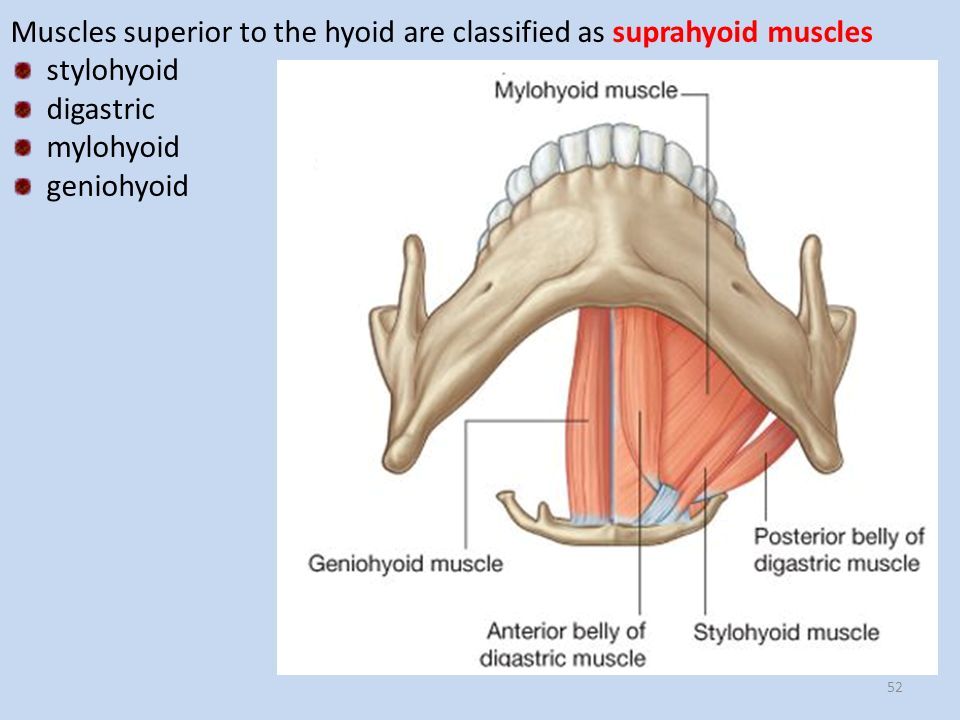
THE MUSCLES of MASTICATION

12
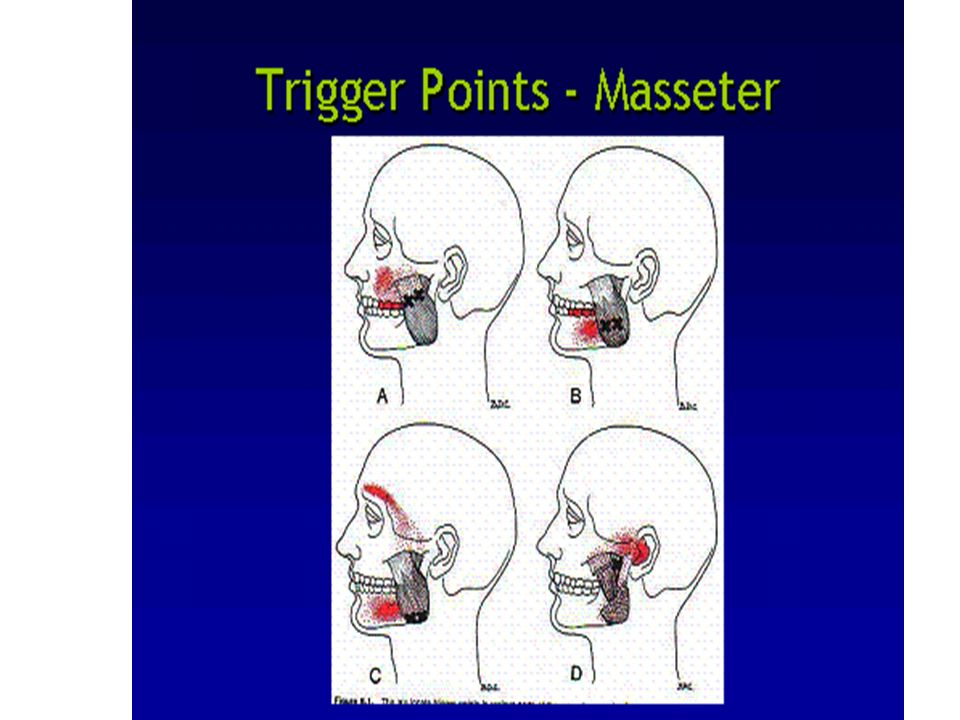
MASSETER MUSCLE

13
TEMPORALIS

14
MEDIAL PTERYGOID Initial Landmark- Inside edge of the Pterygomandibular Raphe

15
MOUTH OPENERS

17
TRIGEMINAL NERVE Sensory - face, scalp, teeth, mouth and nasal cavity Motor nerve to muscles of mastication 3 Nerve Branches Opthalmic Maxillary Mandibular

18
The Trigeminocervical nucleus.

19
SUMMARY OF BIOMECHANICS

20
ETIOLOGY Factors which may be involved in the onset of TMD/J: Specific onset event or No specific onset event

21
TMD SPECIFIC EVENT ONSET

22
MODEL OF TRAUMATIZATION FOR BRUXISM? TRAUMA IN MVA / HEALTH PROFESSIONAL VISITS Meaning of event… in state of relative helplessness Life history of specific traumatic events especially from childhood “fans the flames” Together may result in “Bruxism” which now becomes an unconscious activity incorporated into muscle tension when triggered by memories

23
Occipital lobe Pre- frontal cortex Amygdala Lanius, Hopper & Menon, 2003 HUSBAND WIFE

24
TMD POSTURAL ABNORMALITIES/ FORWARD HEAD POSTURE SINUSITUS/PROLONGED MOUTH BREATHING PARKINSON’S FIBROMYLAGIA IBS SURVIVAL & RIGHTING REFLEX CRANIUM SHAPES MALOCCLUSION NARROW VAULTED PALATE TENSION / STRESS BRUXISM NO SPECIFIC ONSET EVENT SLEEP DISORDERED BREATHING/APNEA

26
Diagnostics FOR TM JOINT RADIOGRAPH CF SCAN MRI

27
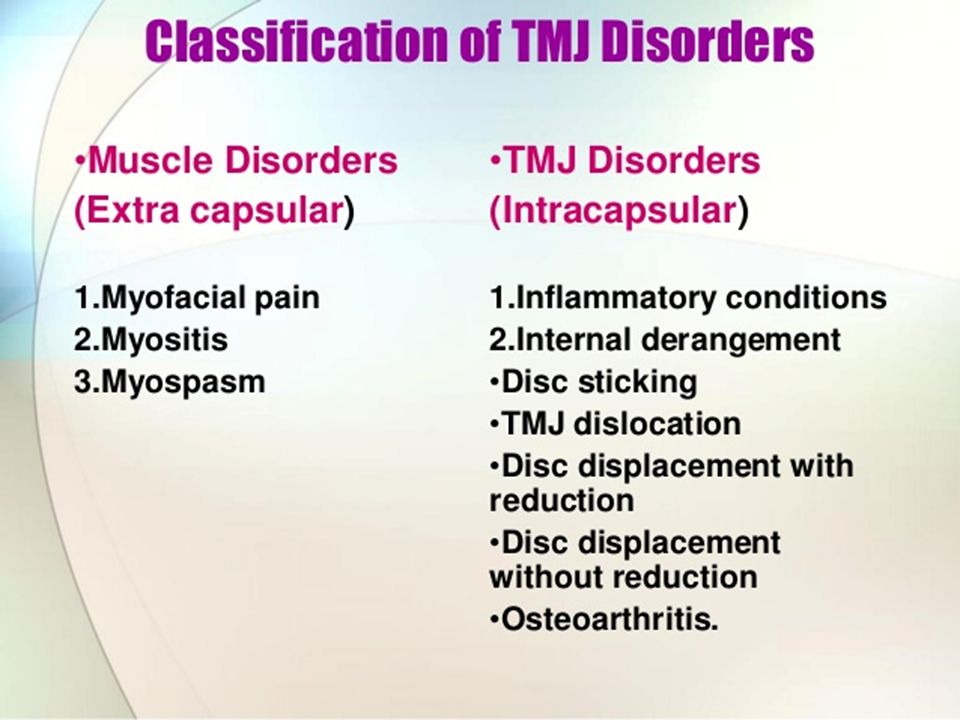
Temporomandibular Disorders Masticatory Muscle pain Myofascial pain (muscle and fascia pain) Symptoms Regional pain in area of Masseter or Temporalis Tinnitus, vertigo, toothache, tension type headache Fatigue with chewing May have limited mandibular function secondary to pain Signs Multiple tender areas in several MM upon palpation Tender areas may refer to other locations in face Sometimes limited active vertical range of motion Myalgia (muscle pain) Symptoms Pain in localized area of one masticatory muscle (usually masseter or Temporalis) Fatigue with chewing Signs Tender muscles on palpation Sometimes limited active vertical range of motion
 Symptoms Regional pain in area of Masseter or Temporalis Tinnitus, vertigo, toothache, tension type headache Fatigue with chewing May have limited mandibular function secondary to pain Signs Multiple tender areas in several MM upon palpation Tender areas may refer to other locations in face Sometimes limited active vertical range of motion Myalgia (muscle pain) Symptoms Pain in localized area of one masticatory muscle (usually masseter or Temporalis) Fatigue with chewing Signs Tender muscles on palpation Sometimes limited active vertical range of motion")
28
Group Two Disc Displacement With Reduction

29
DISC DISPLACEMENT WITH REDUCTION SYMPTOMS Clicking or popping noise in TMJ unilateral or bilateral Headache/neck involvement TMJ AROM < 35mm (less than or equal) TMJ PROM > 5mm greater than pain free opening SIGNS Reciprocal click May have deviation in active opening of mandibular motion and/or in protrusion Restriction in active opening of mandibular motion Excessive anterior glide +ve compression tests
 TMJ PROM > 5mm greater than pain free opening SIGNS Reciprocal click May have deviation in active opening of mandibular motion and/or in protrusion Restriction in active opening of mandibular motion Excessive anterior glide +ve compression tests")
30
Anterior Disc Displacement without reduction

31
Disc Displacement without reduction (closed lock) Symptoms History of clicking and popping in TMJ (past not now) Limited mandibular ROM Signs No TMJ sounds Restriction in active vertical mandibular ROM and laterotrusion,protrusion May have deflection in active vertical mandibular ROM and/ or in protrusion
 Symptoms History of clicking and popping in TMJ (past not now) Limited mandibular ROM Signs No TMJ sounds Restriction in active vertical mandibular ROM and laterotrusion,protrusion May have deflection in active vertical mandibular ROM and/ or in protrusion")
32
Arthritis of TMJ Symptom Pain in TMJ or in front of ear Pain exacerbated by jaw function May have limited mandibular function secondary to pain Signs TMJ tender to palpation TMJ pain worsened upon clenching Limited active mandibular range of motion, laterotrusion, protrusion TMJ sound: Fine to coarse crepitus Radiographic/Imaging: Bony changes:Articular,Glenoid fossa Bite changes

33
Muscles of mastication

34
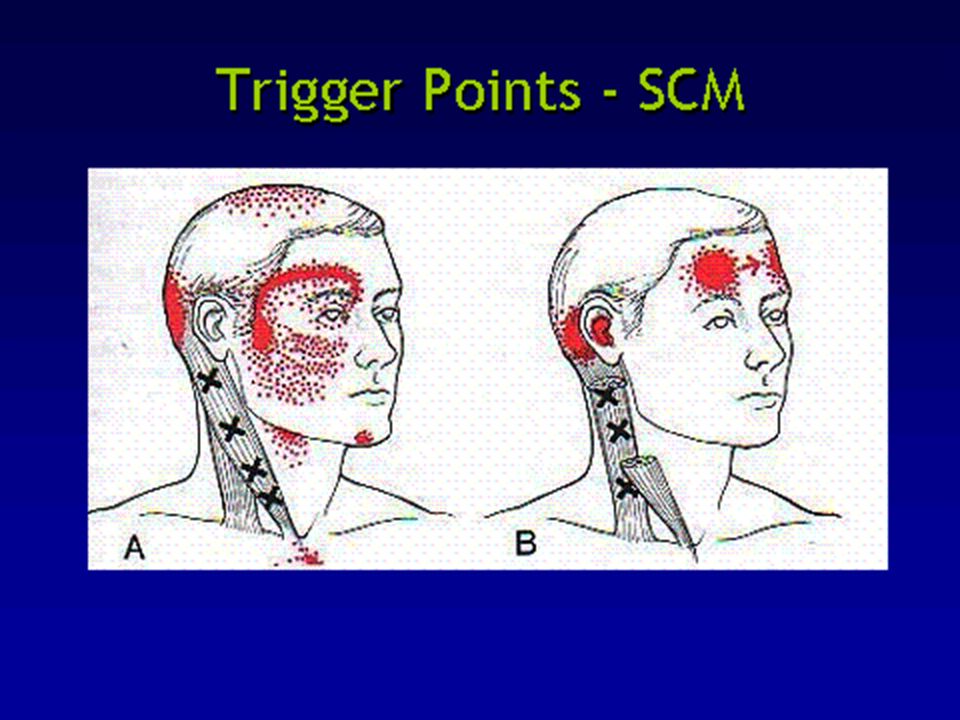
TRIGGER POINTS MYALGIA Trigger points are an area of muscle characterized by local area of firm hypersensitive bands of muscle tissue eg: Referred pain in TMJ - tension type headache painful teeth

35
From Janet Travell

39
MANAGEMENT OF TMD The Role of Health Professionals & Physiotherapist Always a solution to complex issues!

41
THE ROLE OF DENTAL PROFESSIONAL 1.DIAGNOSTIC CRITERIA CHECKLIST & HISTORY

42
Screening for TMJ (After: Epstein 1993) Variable onset and duration of jaw area pain Night pain and bruxism Pain with function, eating, wide opening Joint noise variable, clicking, crepitus Limited opening, deviation on opening Associated symptoms: headaches, dizziness, tinnitus, fatigue, chronic pain syndrome, Sleep apnea Referred pain: neck, ears, face, upper ant chest, headaches Sometimes general dysfunction state PATIENT SYMPTOMS
 Variable onset and duration of jaw area pain Night pain and bruxism Pain with function, eating, wide opening Joint noise variable, clicking, crepitus Limited opening, deviation on opening Associated symptoms: headaches, dizziness, tinnitus, fatigue, chronic pain syndrome, Sleep apnea Referred pain: neck, ears, face, upper ant chest, headaches Sometimes general dysfunction state PATIENT SYMPTOMS")
43
CLICK –MORE THAN 3 IN SUCCESSION

44
Observe

45
Higher risk for TMD

46
Skeletal anterior overbite Over jets < 6mm Retruded cuspal position/intercuspal position Slides < 4mm Unilateral lingual crossbite 5 or more missing posterior teeth Reference: Occlusion, Orthodontic treatment and TMJ disorders: a review. McNamara JA Jr, Seligman DA Okeson JP. J Orofac Pain 1995 Winter;9 (1) ;73-90
 ;")
47
TMJ Dental Examination: PLAN Pain Limitation and Noise

48
Observe jaw clenching, bruxism Limited jaw range of motion, opening, lateral, and protrusion Palpable clicking or crepitus in TMJ TMJ tenderness to palpation Muscle tenderness and tightness in muscles of mastication Screening for TMJ (After: Epstein 1993) CLINICAL SIGNS
 CLINICAL SIGNS")
49
Screening Examination & Range of Mandibular motion

50
HYPER MOBILITY SYNDROME “painful and possible end range clicking/clunking TMJ” On opening, the lateral deflection will be towards the Hypo mobile side On opening, the lateral deflection will always be away from the Hypermobile / subluxing side Inconsistent opening late click and early closing click Right Left Over 55mm opening

51
Right Left On opening, the lateral deflection will be towards the Hypo mobile side Crepitus ++ On opening, the lateral deflection will always be away from the Hypermobile / subluxing side HYPOMOBILITY SYNDROME “Inability to open mouth fully and difficulty chewing, yawning, talking” Less than 35mm opening

52
PHYSIOTHERAPY AND FURTHER ASSESSMENT HISTORY OBSERVATION PALPATION OF JOINT & MUSCLES ACTIVE & PASSIVE RANGE ACCESSORY MOBILITY TESTS RESISTED MUSCLE TESTING STRESS TESTS DYNAMIC LOADING TESTS

53
MORE PALPATION Look for pain using numerical scale in TM JOINT lateral pole Masticatory Muscles Neck and shoulders Neurological

54
How do you manage the anxious patient?

55
PHYSIOTHERAPY TREATMENT EDUCATION ON ETIOLOGY OF TMD HOW TO MANAGE PAIN USING: DIET EXERCISES STRESS MANAGEMENT USING SENSORY MOTOR PSYCHOTHERAPY

56
EXERCISE IS KEY! ROCABADO

57
OBSERVE & ASK QUESTIONS YOU CAN HELP

58
DENTAL SENSORY MODULATION TOOLS & TECHNIQUES TOOLS: THIN HEAD PILLOW HOT TOWELS HEAVY BLANKET HEAD PHONES GLASSES SQUISHY BALL RUBBER BAND TAPPING PATIENT BODY POSITION LIGHT TOUCH /FREQUENT BREAKS/ & A SMILE !

59
QUESTIONS

61
Learning with Laughter Cathy Russell. Dip PT (UK), MCPA, ATM www.cathymrussell.com http://www.cathymrussell.com/blog/ Humor helps us relax… When we relax we learn
, MCPA, ATM Humor helps us relax… When we relax we learn.")
62
Left TM Joint with DD with reduction

Similar presentations






















, MCPA, ATM Humor helps us relax… When we relax.>")

