Download presentation
Presentation is loading. Please wait.

1
Clinical cases in ENT AND picture quiz

2
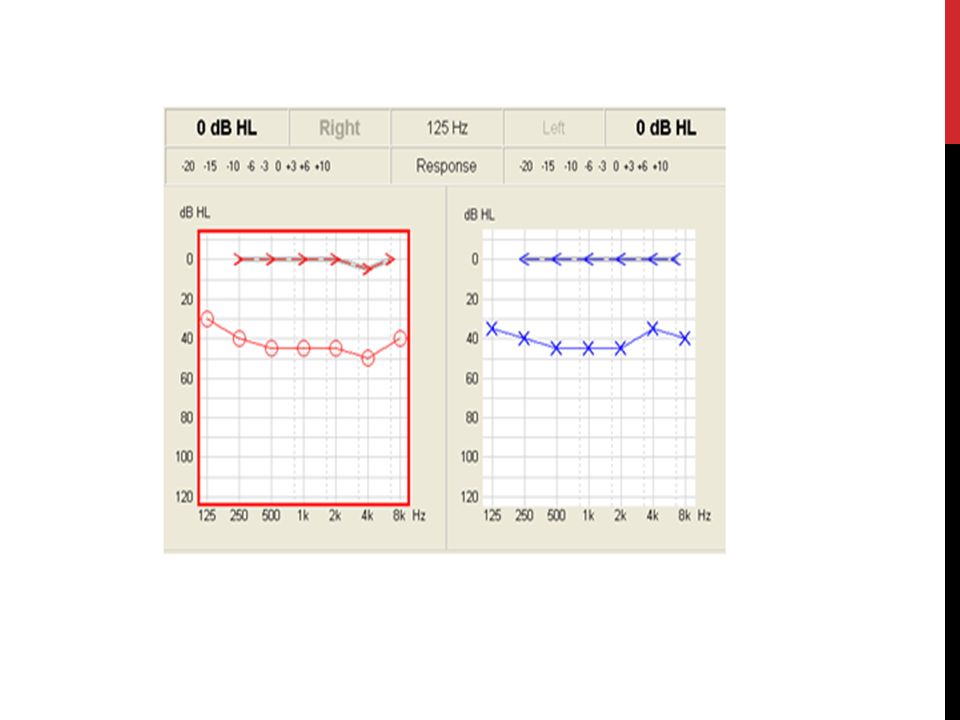
CASE 1 A 36-year-old woman presents with recurrent episodes of right-sided tinnitus, hearing loss and vertigo. Episodes typically last between minutes. He also describes a 'full' sensation in his right ear. Otoscopy is unremarkable and the cranial nerve examination is normal.

3
Diagnosis? Meniere's disease More common in middle-aged adults Triad of Recurrent episodes of vertigo, tinnitus and hearing loss (which type?) Episodes last minutes to hours What other features can be seen? Nystagmus and positive Romberg test
 Episodes last minutes to hours What other features can be seen. Nystagmus and positive Romberg test .")
4
Management of acute attacks
Management of acute attacks? Bed rest, vestibular sedatives (Diazepam), Prochlorperazine for N&V Prevention of attacks? Betahistine,? Salt restriction
, Prochlorperazine for N&V Prevention of attacks Betahistine, Salt restriction")
5
Let’s say this patient had absent corneal relfex on examination
Let’s say this patient had absent corneal relfex on examination. Would your differential diagnosis change? Acoustic neuroma

6
CASE 2 A 31-year-old man presents with bilateral hearing loss and tinnitus. There is a family history of similar problems. Examination of the tympanic membranes:

8
Diagnosis? Otosclerosis What is otosclerosis? Autosomal dominant. Replacement of normal bone by vascular spongy bone. Onset is usually at years conductive deafness tinnitus tympanic membrane - 10% of patients may have a 'flamingo tinge', caused by hyperaemia positive family history

9
Case 3 Which one of these is the correct technique to stop epistaxis?

10
Picture A- So-called ‘Hippocratic technique’ Where do most nose bleeds come from? Little’s area in the anterior inferior part of the nasal septum.

11
TYPES OF EPISTAXIS 1) ANTERIOR: Most common site
Known as little’s area (Kiesselbach’s plexus) Nose picking & Infection 2) POSTERIOR: Known as Woodruff’s plexus hypertension +/- anticoagulants 3) Lateral wall/Nasal mucosa/Postnasal space
 Nose picking & Infection. 2) POSTERIOR: Known as Woodruff’s plexus. hypertension +/- anticoagulants. 3) Lateral wall/Nasal mucosa/Postnasal space.")
12
Local Causes: Trauma, Infection, Foreign body, Previous surgery Tumors: Rare Juvenile Nasopharyngeal Angiofibroma -> recurrent unilat. Epistaxis. Illicit drug use: Cocaine/septal perforation Systemic Causes: Hypertension Hepatic disease Blood Dyscrasias Endometriosis patient will give history of cyclical epistaxis Genetic: Osler-weber-Rendu syndrome ( Hereditary Haemorrhagic telangiectasia) Autosomal Dominant Vascular malformation where vessel walls lack contractile elements Affect respiratory and GI systems Medication: Aspirin, warfarin, heparin, NSAIDS
 Autosomal Dominant. Vascular malformation where vessel walls lack contractile elements. Affect respiratory and GI systems. Medication: Aspirin, warfarin, heparin, NSAIDS.")
13
Management of epistaxis?
ABC- make sure the patient is adequately resuscitated Identify the source of bleeding Apply local anaesthetic and vasoconstrictor to nasal mucosa. (Do not use vasoconstrictors if the patient is hypertensive) If bleeding point can be identified, cauterise (either chemical with silver nitrate or electro- cautery) If no source can be identified or cautery has failed: Anterior packing If cannot be localized anteriorly or controlled with anterior packing: Posterior packing Arterial embolisation or arterial ligation
 If bleeding point can be identified, cauterise (either chemical with silver nitrate or electro- cautery) If no source can be identified or cautery has failed: Anterior packing. If cannot be localized anteriorly or controlled with anterior packing: Posterior packing. Arterial embolisation or arterial ligation.")
14
When to admit the patient
When to admit the patient? If bleeding continues Nasal pack (don’t forget Ab cover) Posterior bleed Elderly, frail When sending home, patient education and Naseptin (Avoid with nut allergy!)
 Posterior bleed Elderly, frail When sending home, patient education and Naseptin (Avoid with nut allergy!)")
15
CaseS 4-8 1) 24 year old primary school teacher. Gradual onset of voice change, worse at the end of day. Vocal nodules 2) 62 year old smoker; 3 month history of sudden onset change in voice. Has a cough. Had one episode of hemoptysis. Left vocal cord paralysis 3) 42 year old female publican; smokes 20 cigarettes a day. Enjoys curry twice a week. Takes Gaviscon. Noticed her voice has become deeper over last 9 months. Was upset when she was mistaken for a man on the phone during a dating agency interview. Reinke’s oedema 4) 30-year old lead singer in a famous rock band. Felt a sharp pain at the level of larynx during the last concert. Was unable to finish the concert. Vocal fold hemorrhagic polyp
 24 year old primary school teacher. Gradual onset of voice change, worse at the end of day. Vocal nodules 2) 62 year old smoker; 3 month history of sudden onset change in voice. Has a cough. Had one episode of hemoptysis. Left vocal cord paralysis 3) 42 year old female publican; smokes 20 cigarettes a day. Enjoys curry twice a week. Takes Gaviscon. Noticed her voice has become deeper over last 9 months. Was upset when she was mistaken for a man on the phone during a dating agency interview. Reinke’s oedema 4) 30-year old lead singer in a famous rock band. Felt a sharp pain at the level of larynx during the last concert. Was unable to finish the concert. Vocal fold hemorrhagic polyp")
16
2 year old child is presenting with fever and otalgia.
Case 9 2 year old child is presenting with fever and otalgia.

17
What is the diagnosis? Acute otitis media 2) Most common pathogens? 50% Viral; Bacterial: o Streptococcus pneumoniae o Haemophilus influenzae o Moraxella catarrhalis 3) Management? Most likely spontaneous rupture and resolution + management of symptoms. 4) Most serious possible complication? Brain abscess
 Management Most likely spontaneous rupture and resolution + management of symptoms. 4) Most serious possible complication Brain abscess.")
18
Glue ear (Otitis media with effusion)
6 months later, mom is concerned about his hearing and delayed speech. You can see from the notes he had 2 other episodes of otitis media since last time. Glue ear (Otitis media with effusion)
")
19
Case 10 This is the right ear of a 28-year-old man with recurrent ear discharge.

20
What is the diagnosis? Cholesteatoma Main features: foul smelling discharge hearing loss Other features are determined by local invasion: vertigo facial nerve palsy cerebellopontine angle syndrome Management: Refer to ENT for consideration of surgical removal

21
Picture quiz RHINOPHYMA

22
Reinke’s oedema (Gross oedema of the vocal folds)
")
23
This patient is presenting with renal failure and nose deformity.
WEGENER’S GRANULOMATOSIS

24
CAULIFLOWER EAR- UNTREATED AURICULAR HEMATOMA

25
QUINSY (PERITONSILLAR ABSCESS)
")
26
THANK YOU! ANY QUESTIONS?

Similar presentations






Primary Tumours: Benign Glomus tumour Malignant Carcinoma,sarcoma 2)Secondary Tumours: a) From adjacent areas like.>")












