Download presentation
Presentation is loading. Please wait.

1
Human Factors in Healthcare Education Chris Hancock – Programme Manager, Rapid Response to Acute Illness (RRAILS), 1000 Lives Plus
, 1000 Lives Plus")
2
“ It may seem a strange principle to enunciate as the very first requirement in a hospital – that it should do the sick no harm” (Florence Nightingale: Notes on Hospitals,1859)
")
3
Hospital Mortality and Harm There is a one in 300 chance of accidental death through errors in care. (Institute of Medicine, 2000) More than one in ten people admitted to hospital are harmed unintentionally by its care. (Vincent et al. 2001)
 More than one in ten people admitted to hospital are harmed unintentionally by its care. (Vincent et al. 2001).")
4
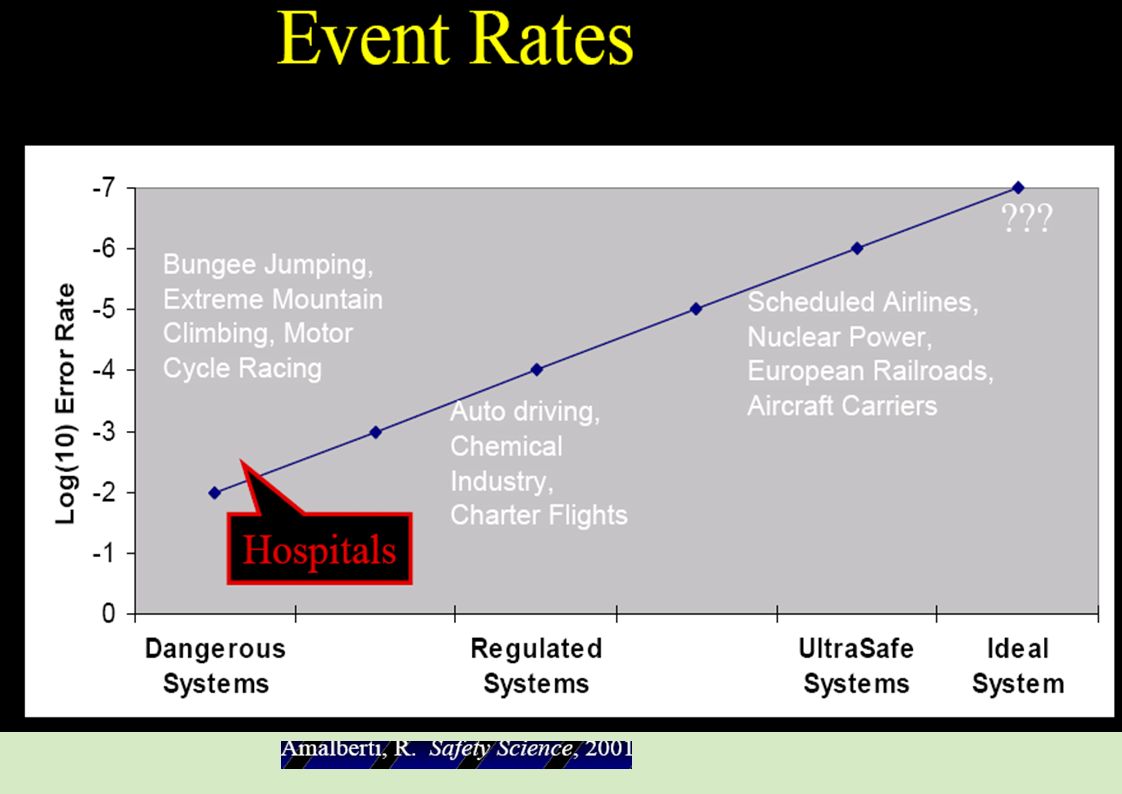
Patient Safety—A Global Issue “In effect a new public health risk”

6
Patient Safety 3,283 patients dead through preventable error, another 7,000 suffer severe harm Equivalent to 9 medium size aircraft (Boeing 737/Airbus A320) being written off with total loss of life every year…… …..in the UK!
 being written off with total loss of life every year…… …..in the UK!")
7
Errors In Aviation % of Accidents Time (The History of Powered Flight) 2011 Human Failure Aircraft Failure
 2011 Human Failure Aircraft Failure")
8
Accidents Still Happen! Some 80% of aviation accidents are attributable in whole or part to Human Factors.

9
Human Error Situational Awareness Limits of Performance Decision Making Communications Leadership Motivation Synergy Personality Morale Culture Ethos Stress/Sleep Workload Management Tech Knowledge Tech Skills Human Factors

10
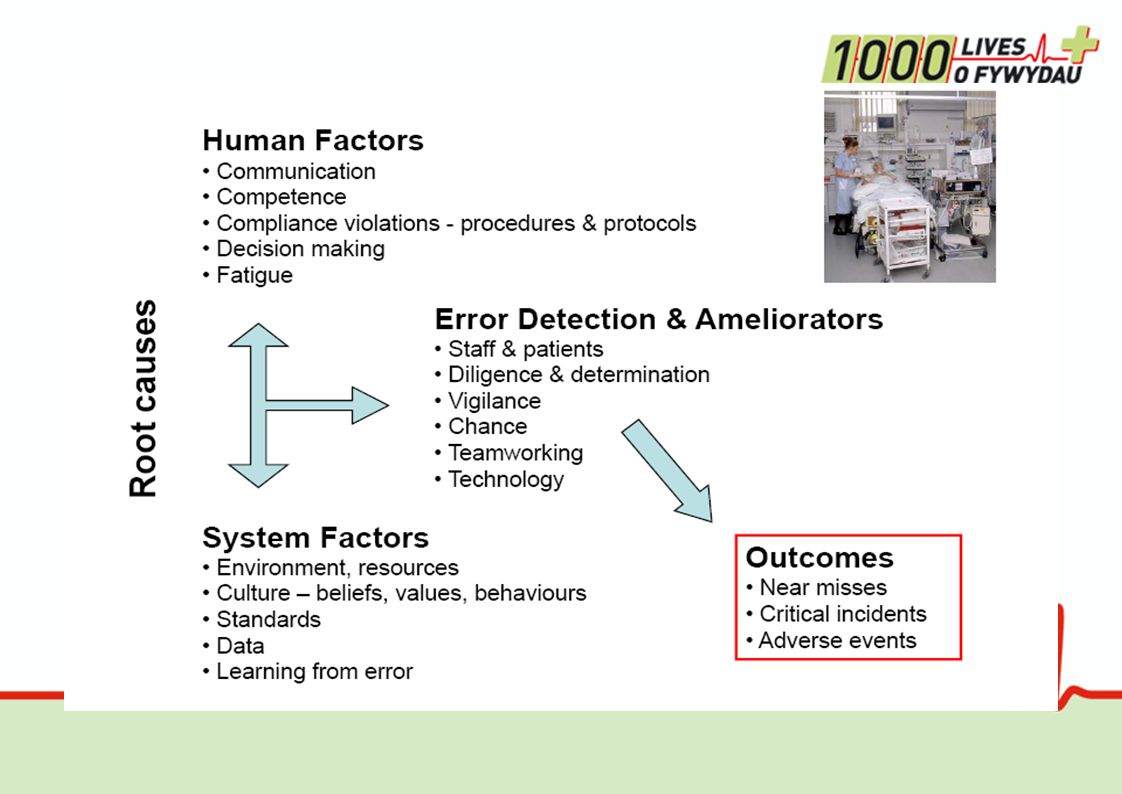
What are the top five causes of harm and waste in the acute ward?

11
Errors of Omission/ Adverse Events The Defect Rate in technical quality of American health care is approximately: 45% McGlynn, et al: The quality of health care delivered to adults in the United States. NEJM 2003; 348: 2635-2645 (June 26, 2003) It’s what we don’t do that causes the harm
 It’s what we don’t do that causes the harm.")
12
Error is Inevitable Because of Human Limitations Limited memory capacity – 5 pieces of information in short term memory Negative effects of stress – error rates Tunnel vision Negative influence of fatigue and other physiological factors Limited ability to multitask – cell phones and driving Flawed judgment

13
Concept of foresight training ‘Error wisdom on the frontline’ James Reason 2004

14
How do Accidents Happen? Organisation and processes -Pre-op, missing notes- latent Prior conditions – patient factors “Unsafe” acts – active failures Multiple Defences Patient Safety Patient Safety Incident

15
Adapted from REASON, 2005 People Environment Workspace Task Equipment Staff Patients The ‘system’ Factors within the healthcare system that could potentially lead to harm Staff act as harm absorbers Organisation

16
Insert name of presentation on Master Slide

18
The fact that we can misperceive situations despite the best of intentions is one of the main reasons that our decisions and actions can be flawed such that …

19
Human beings make “silly” mistakes Regardless of their experience, intelligence, motivation or vigilance, people make mistakes

20
One definition of “human error” is “human nature” Error is the inevitable downside of having a brain!

21
What is an error? the failure of a planned action to achieve its intended outcome a deviation between what was actually done and what should have been done Reason A definition that may be easier to remember is: ○“Doing the wrong thing when meaning to do the right thing.”

22
Situations associated with an increased risk of error unfamiliarity with the task* inexperience* shortage of time inadequate checking poor procedures poor human equipment interface Vincent * Especially if combined with lack of supervision

23
Individual factors that predispose to error limited memory capacity further reduced by: ○fatigue ○stress ○hunger ○illness ○language or cultural factors ○hazardous attitudes

24
Fatigue 24 hours of sleep deprivation has performance effects ~ blood alcohol content of 0.1% Dawson – Nature, 1997

25
Stress and performance The relationship between stress and performance Stress level Area of “optimum” stress Low stress Boredom High stress Anxiety, panic Performance level Yerkes, R. M., & Dodson, J. D. (1908) The relation of strength of stimulus to rapidity of habit-formation. Journal of Comparative Neurology and Psychology, 18, 459-482
 The relation of strength of stimulus to rapidity of habit-formation. Journal of Comparative Neurology and Psychology, 18,")
26
Apply human factors thinking to your work environment (WHO) 1.Avoid reliance on memory 2.Make things visible 3.Review and simplify processes 4.Standardize common processes and procedures 5.Routinely use checklists 6.Decrease the reliance on vigilance
 1.Avoid reliance on memory 2.Make things visible 3.Review and simplify processes 4.Standardize common processes and procedures 5.Routinely use checklists 6.Decrease the reliance on vigilance")
27
1. Avoid reliance on memory Insert name of presentation on Master Slide

28
2. Make things visible PSAG Board Single Point of Ward Information Safety Briefings

29
3.Review and simplify processes Insert name of presentation on Master Slide

30
4. Standardise common processes and procedures Insert name of presentation on Master Slide

31
5. Routinely use checklists Insert name of presentation on Master Slide

32
6. Decrease the reliance on vigilance Insert name of presentation on Master Slide

33
Background - Improving Reliability Level 1 Prevent Initial Failure –standardise, train, measure & feedback Level 2 Identify failure and mitigate –decision aids, desired action by default, clear specification of the standard that can be articulated –Human factor changes –Redundancy function Level 3 Redesign from failure modes –Identify critical failures and then redesign prevent identify redesign

34
Crew Resource Management Training Focus on teamwork, communication, flattening hierarchy, managing error, situational awareness, decision making Non-punitive reporting of near misses, 500,00 reports over 15 years Very open culture with regard to error and safety

36
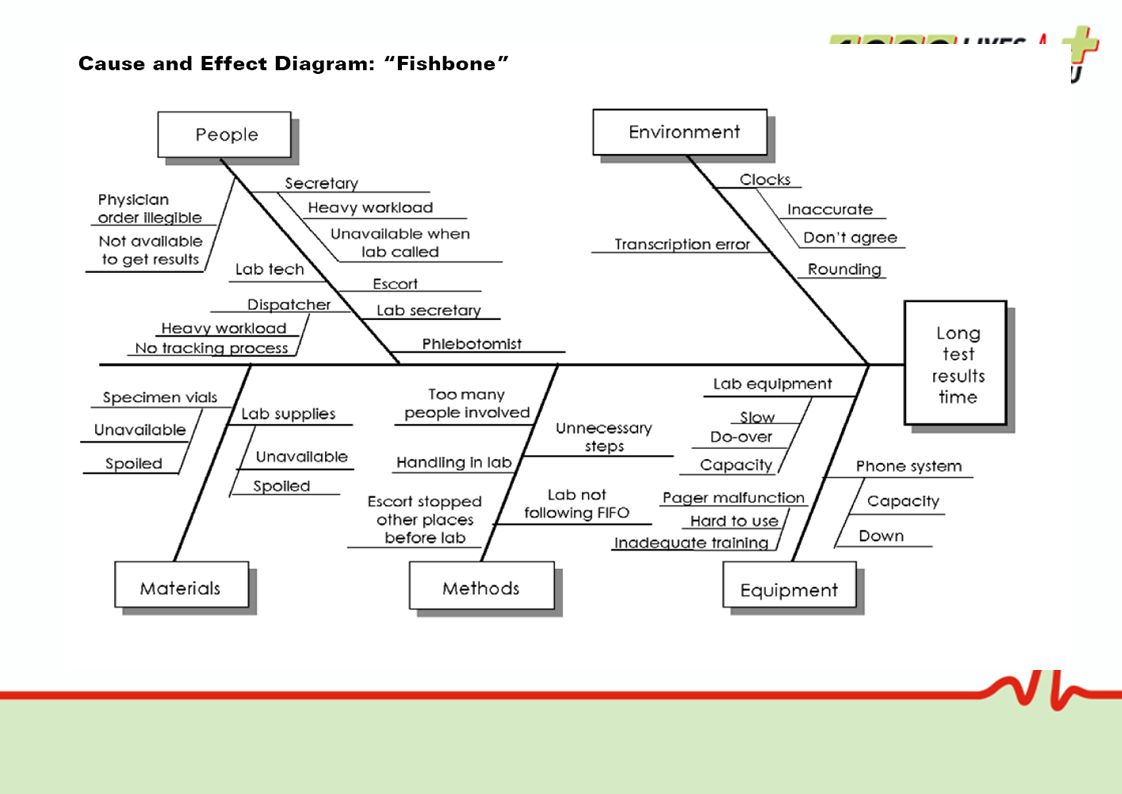
Root Cause Analysis using the 5 Whys Invented in the 1930’s by Toyota Founder Kiichiro Toyoda’s father Sakichi Made popular in the 1970s by the Toyota Production System The 5 Whys strategy involves looking at any problem and asking “Why?” and “What caused this problem?”

38
Education Insert name of presentation on Master Slide

39
The ‘three bucket’ model for assessing risky situations (Reason, 2004) 1 2 3 SELFCONTEXTTASK The fuller your buckets, the more likely something will go wrong, but your buckets are never empty.
 SELFCONTEXTTASK The fuller your buckets, the more likely something will go wrong, but your buckets are never empty.")
40
Self Bucket Level of knowledgenewly qualified Level of skillcompetence and experience Level of experienceinvoluntary automaticity, under/over confidence Current capacity to do the task fatigue, time of day, negative life events

41
Equipment and devicesusability, not available Physical environmentlighting, noise, temperature Workspaceworking environment, writing space, Team and supportleadership, stability and familiarity, trust Organisation and management safety culture, culture, targets and workload Context Bucket

42
Errorsomission errors, primary goal achieved before all steps complete, lack of cues from previous steps Task complexity calculations Novel taskunfamiliar or rare events Processtask overlap, multi-tasking Task Bucket

43
Simulation Those who work together should train together. D. Cumin et al Standards for simulation in anaesthesia: creating confidence in the tools Br. J. Anaesth. (2010) 105(1): 45-51
 105(1):")
44
Teaching Human Factors Action learning – all the collaboratives learn important lessons about human factors Insert name of presentation on Master Slide

Similar presentations