Download presentation
Presentation is loading. Please wait.

1
Glaucoma

2
Glaucoma Intraocular pressure is usually a key modifying factor .
The term glaucoma refers to a group of diseases that have in common : A characteristic optic neuropathy Associated visual field loss Intraocular pressure is usually a key modifying factor .

3
The intraocular pressure (IOP)
The accepted range of IOP in the general population is mmHg. Normal physiological variations in IOP (1-2 mmHg), varies with : Respiration . BP, heartbeats . Time of day (maximum in the morning).
, varies with : Respiration . BP, heartbeats . Time of day (maximum in the morning).")
4
IOP measured by: -Indentation tonometry: Schiotz tonometry . -Applanation tonometry: Goldmann tonometry

5
Eye ball can be considered as a closed system with relatively constant contents, except the aqueous humor. The continuous turnover of aqueous is the main determinant of IOP.

6
Three factors determine the IOP
The rate of aqueous humor production by the ciliary body . Resistance to the aqueous outflow across the trabecular meshwork – Schlemm’s canal system . The level of episcleral venous pressure .

7
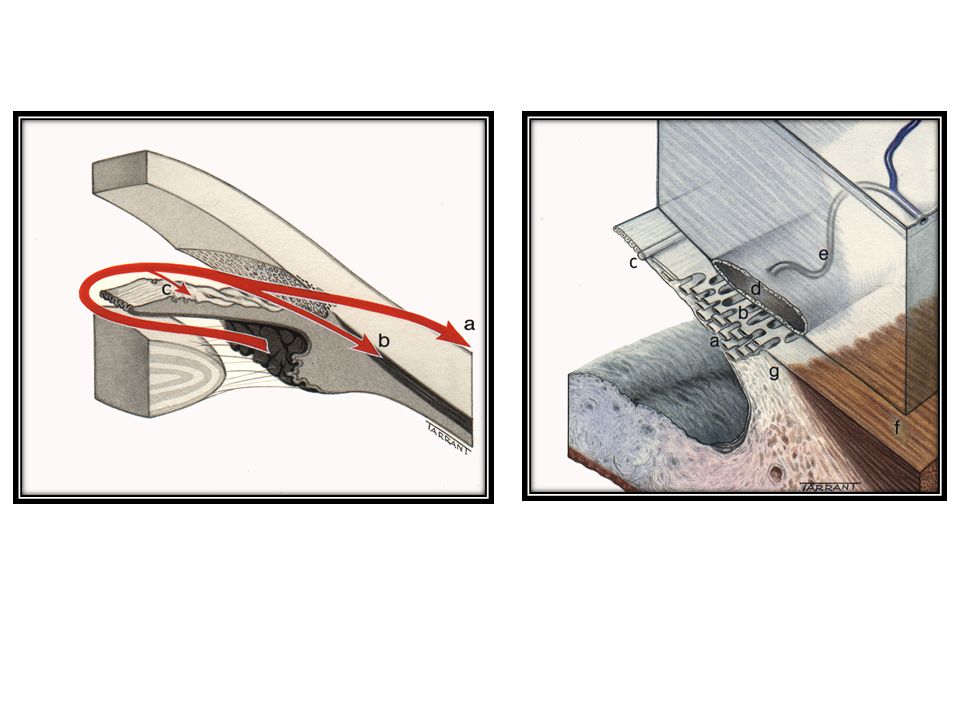
Aqueous Pathway: Aqueous is produced from ciliary processes into the posterior chamber, passes through the pupil into the anterior chamber and leave the eye through: Angle of anterior chamber ( 90%) the aqueous passes across trabecular meshwork into canal of schlemm, and then drained by the episcleral veins. Uveoscleral route (10%) the aqueous passes across the ciliary body into the suprachoroidal spaces and is drained by the venous circulation
 the aqueous passes across trabecular meshwork into canal of schlemm, and then drained by the episcleral veins. Uveoscleral route (10%) the aqueous passes across the ciliary body into the suprachoroidal spaces and is drained by the venous circulation.")
9
Angle of the anterior chamber :
The angle between the posterior surface of the cornea and the anterior surface of the iris.

10
At the angle there is a circumferential porous meshwork about 1 mm in width called Trabecular meshwork , through which aqueous drained from the anterior chamber to canal of Schlemm

11
The configuration of the angle indicate the pathogenesis of glaucoma.

12
Contact between the peripheral iris and the cornea signifies a closed angle .
while wide separation between the two indicate open angle .

13
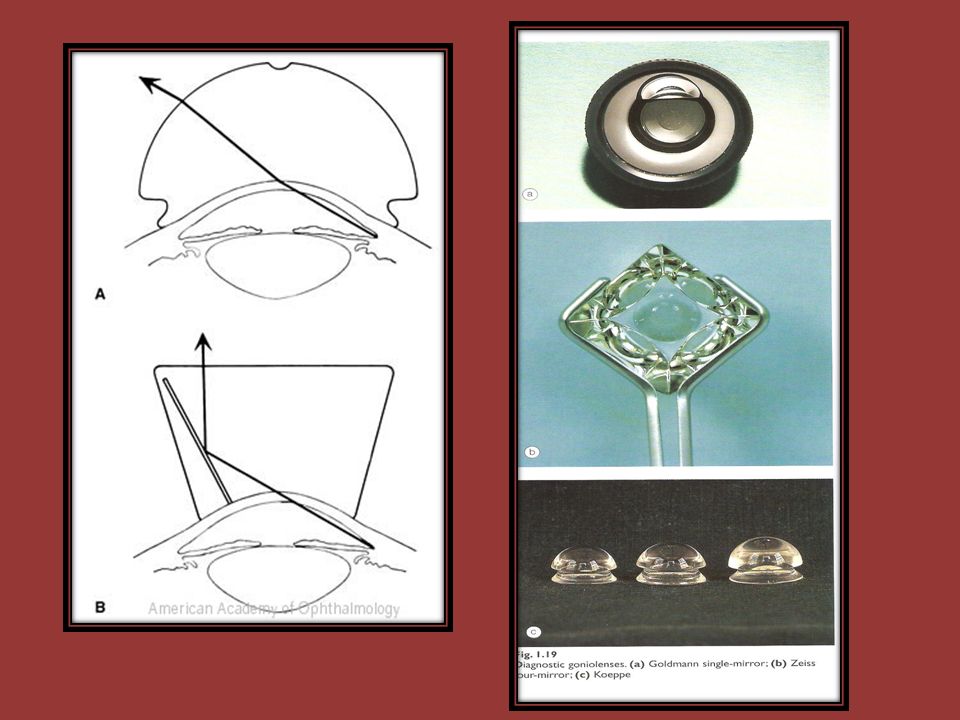
Gonioscopy: Examination of the angle of the anterior chamber performed by goniolenses

15
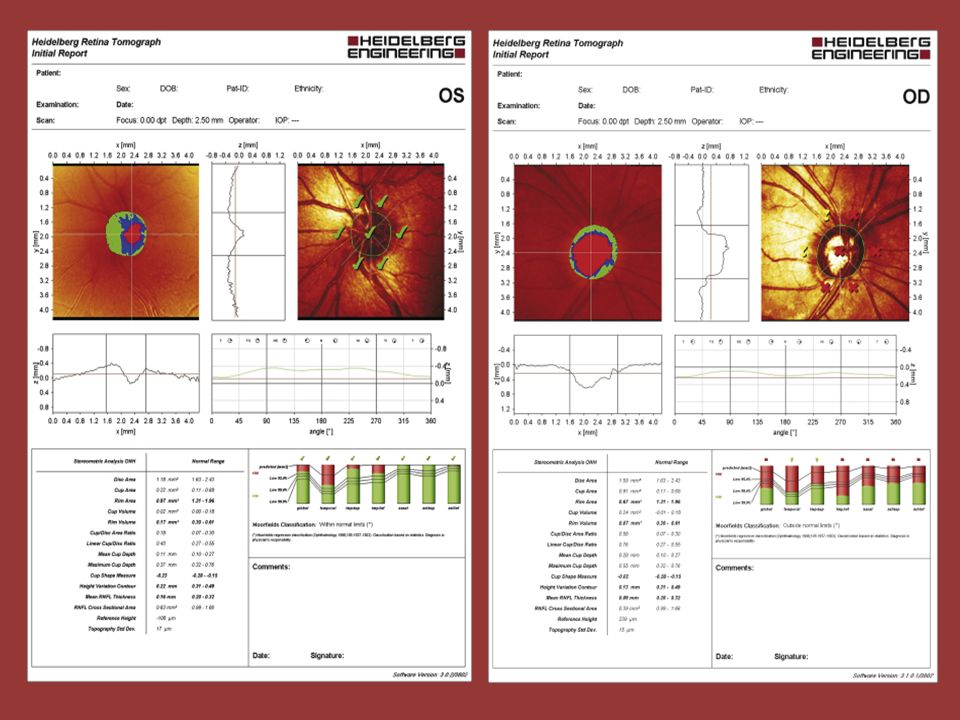
Optic disc: Anterior end of the optic nerve, about 1.5 mm in diameter. Lies about 3mm from the fovea. All retinal layers except the nerve fiber layer stop at the margin of the optic disc. The nerve fiber layer pass through the lamina cribrosa a sieve like structure, bridge the posterior scleral foramen. Optic cup; central depression in the optic disc not occupied by neural tissue. Cup/Disc ratio in most normal eyes is 0.3 or less, asymmetry of 0.2 or more is suspicion.

17
Visual Field

22
Classification of glaucoma:
Open angle glaucoma Primary open angle glaucoma Secondary open angle glaucoma Closed angle glaucoma Primary closed angle glaucoma Secondary closed angle glaucoma Congenital glaucoma Buphthalmus

23
Primary glaucomas are not associated with ocular or systemic disorders that cause increase resistance to aqueous outflow. Primary glaucomas usually affect both eyes and may be inherited. Secondary glaucomas are associated with ocular or systemic disorders that are responsible for increase resistance to aqueous outflow. Secondary glaucomas are usually unilateral and not inherited.

24
Primary Open Angle Glaucoma (POAG)
Definition : is generally bilateral disease (although not nessessarly a symmetrical disease ) of adult onset . characterized by : An IOP > 21 mmHg at some stage . Glaucomatous optic nerve damage . An open anterior chamber angle . Characteristic visual field loss as the damage progress .
 of adult onset . characterized by : An IOP > 21 mmHg at some stage . Glaucomatous optic nerve damage . An open anterior chamber angle . Characteristic visual field loss as the damage progress .")
25
Increase IOP caused by increase resistant to aqueous outflow due to thickening of the trabecular meshwork lamellae, with reduce in the pores size.

26
Theories of glaucomatous damage
Direct damage by pressure Capillary occlusion Interference with axoplasmic flow

27
Risk factors 1- Age 2- Race: more common and a more severe in Blacks .
3- Family history and inheritance. 4- Myopia: increased incidence of POAG. 5- D.M and vascular disease .

28
Diagnosis History Visual symptom will usually be absent , unless damage is advanced . Previous ophthalmic history (Refractive status and causes of secondary glaucoma ) F.H PMH Current medication and allergies . Examination V.A Pupil SLE Tonometry noting the time of the day Gonioscopy Optic disc examination Perimetry Optic disc or peripapillary RNFL imaging .
 F.H. PMH. Current medication and allergies . Examination. V.A. Pupil. SLE. Tonometry noting the time of the day. Gonioscopy. Optic disc examination. Perimetry. Optic disc or peripapillary RNFL imaging .")
29
IOP > 21mmHg is suspicious .

30
Optic nerve head damage : Increase in cup/disc ratio.
Most normal eyes have cup/disc of 0.3 or less Increase in cup/disc ratio or asymmetry between two eyes of 0.2 or more is suspicion.

31
Visual field defects : Paracentral scotoma . arcuate scotoma . peripheral field loss with nasal step generalized visual loss, leaving small central vision which is lost at the end

32
Open angle assessed by gonioscopy

33
Glaucomatous disc damage
IOP > 21 mmHg Open angle of normal appearance Visual field loss Glaucomatous disc damage

34
Management: The aim of management is to reduced IOP to the target pressure (safe pressure) at which no further damage occurs. Continuous follow up with checking IOP, examination of the optic disc and assessment of the visual field is essential. Initially primary open angle glaucoma is treated medically with topical eye-drops, but if IOP is not reduced to the target pressure then laser therapy or surgery has to be considered

35
Treatment: Medical: A-Beta adrenergic blocking drugs .
Mode of action: decrease the aqueous production e.g. Timolol 0.5% eye drops B-Topical carbonic anhydrase inhibitors; Mode of action: decrease the aqueous production e.g. Dorzolmide2% eye drops C- Cholinergic drug Mode of action: increase the aqueous outflow e.g. Pilocarpine 2% eye drops

36
D- Sympathomimetics drugs;
Mode of action: decrease the aqueous production and increase uveoscleral aqueous outflow e.g. Brimonidine 0.2% eye drops E- Prostaglandin derivatives Mode of action: increase uveoscleral aqueous outflow e.g. Latanoprost eye drops

37
2- Laser Trabeculoplasty is a procedure by which the application of discrete burns to the trabeculum meshwork enhance aqueous outflow and lower IOP.

38
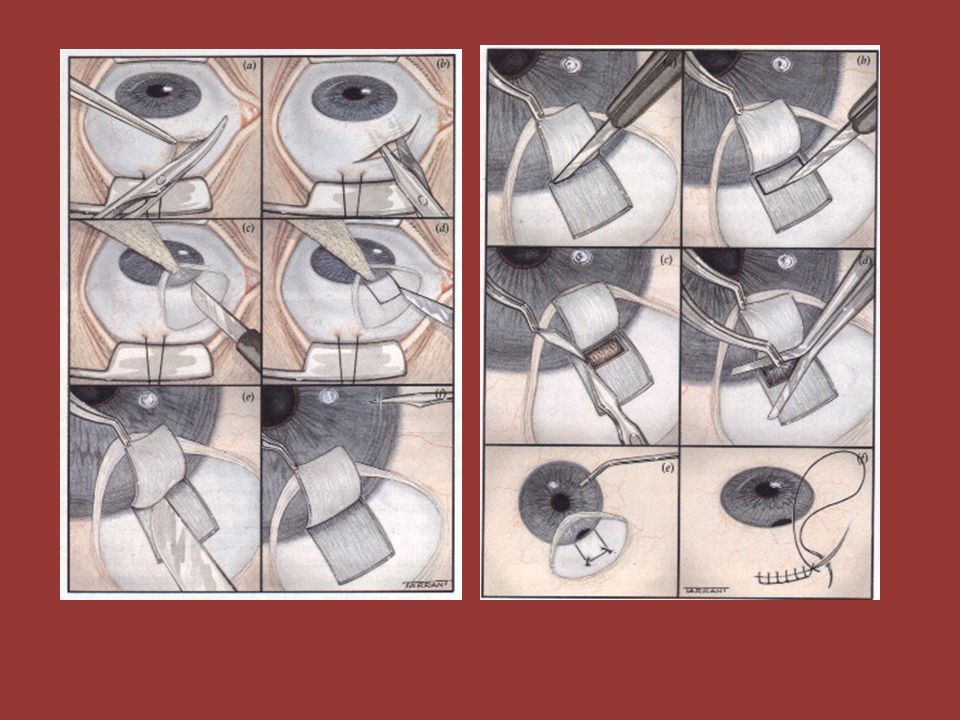
3- Surgical : Trabeculectomy (creating a fistula between the anterior chamber and sub-Tenon space to by pass the trabecular meshwork.

40
Secondary Open Angle Glaucoma
Angle is open, but the trabecular meshwork blocked by: Blood (hyphaema) following trauma Inflammatory cells(iritis) Pigment from the post pigment epithelium of the iris(pigment dispersion syndrome) Deposition of amyloid- like substance (pseudoexfoliative syndrome) Drug induced (steroid induced glaucoma)
 following trauma. Inflammatory cells(iritis) Pigment from the post pigment epithelium of the iris(pigment dispersion syndrome) Deposition of amyloid- like substance (pseudoexfoliative syndrome) Drug induced (steroid induced glaucoma)")
45
Ocular hypertension; IOP>21 without optic disc cupping and visual field defect. 7% of the general population above 40 have IOP>21 only 1% of them have glaucoma. Normal tension glaucoma; patients with IOP= or <21mmHg with optic disc cupping and visual field defect.

46
Primary angle closure glaucoma (PACG)
Is a condition in which elevation of IOP occurs as a result of obstruction of the aqueous drainage by closure of the angle with the peripheral iris.

47
Anatomical predisposing factors
1- Relative anterior location of iris-lens diaphragm. 2- Shallow anterior chamber (AC) due to short axial length of the eye ( e.g. hypermetropia). 3- Narrow entrance to anterior chamber angle.
 due to short axial length of the eye ( e.g. hypermetropia). 3- Narrow entrance to anterior chamber angle.")
48
Mechanism of angle closure
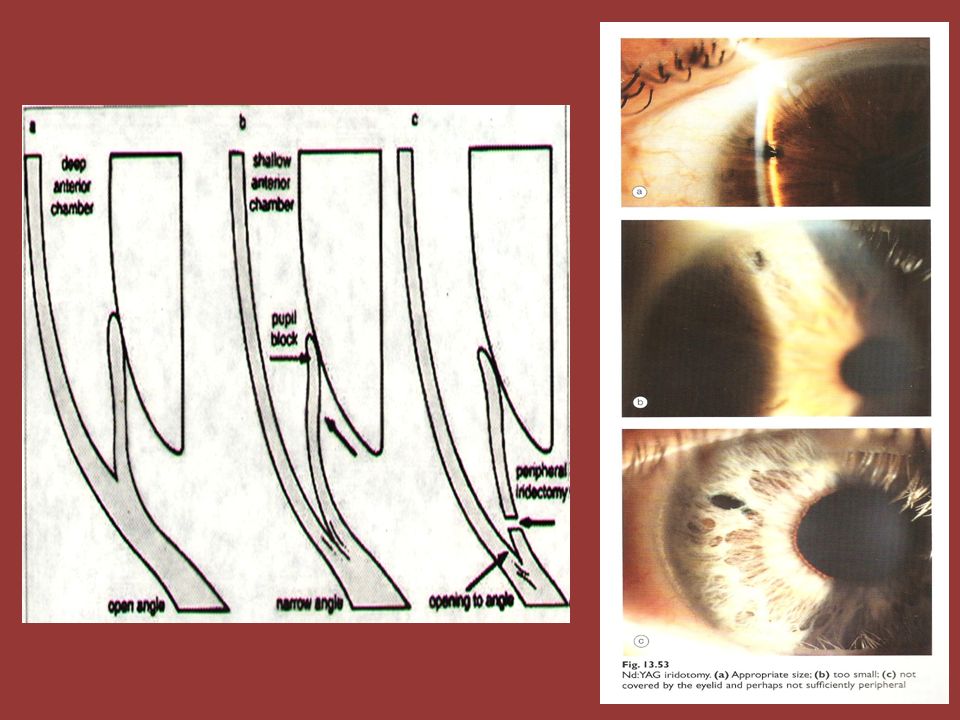
In most cases PCAG is initiated by; a- Pupillary Block : which is increase resistance to aqueous passage between posterior and anterior chamber by the iris lens contact . b- Iris bombe : increase pressure in the posterior chamber, the peripheral iris will bow forward c- Irido-corneal contact : obstructing the angle .

49
If this peripheral irido-corneal contact persist for few days then permanent peripheral anterior synachae (PAS) occurs
 occurs")
50
Presentation Average age of is about 60 years and above More common in females Frequently bilateral, although presentation is asymmetrical

51
Classification 1. Latent 2. Subacute 3. Acute 4. Chronic 5. Absolute

52
Subacute ( Intermittent) Angle Closure Glaucoma
A transient attack of sudden subtotal closure of the angle results in rapid increase in IOP, followed by spontaneous reopening of the angle with the IOP returns to normal.

53
Symptoms The attack may be precipitated by physiological mydriasis (dilation of the pupil) e.g. watching T.V. in dark room Sudden onset of 1-Blurring of vision 2-Halloes around light due to corneal edema 3- Sometimes eye-ache or headache The attack may last for 1-2 hours and usually broken by miosis (constriction of the pupil) e.g. exposure to bright light.
 e.g. exposure to bright light.")
54
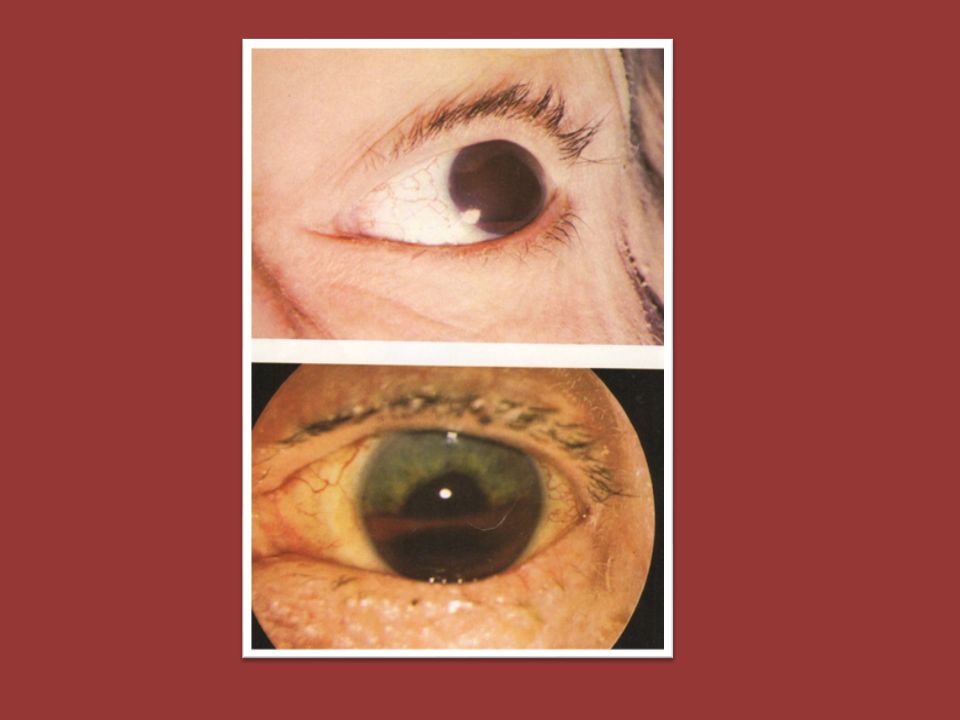
Signs During the attack Corneal edema Shallow anterior chamber Elevated IOP Between the attacks The eye looks normal apart from narrow angle

55
Treatment Laser iridotomy to create an opening between the posterior chamber and anterior chamber and bypass the pupillary block Both eyes must be treated with Laser iridotomies

56
Acute Angle Closure Glaucoma
Sudden total closure of the angle with rapid high increase in IOP.

57
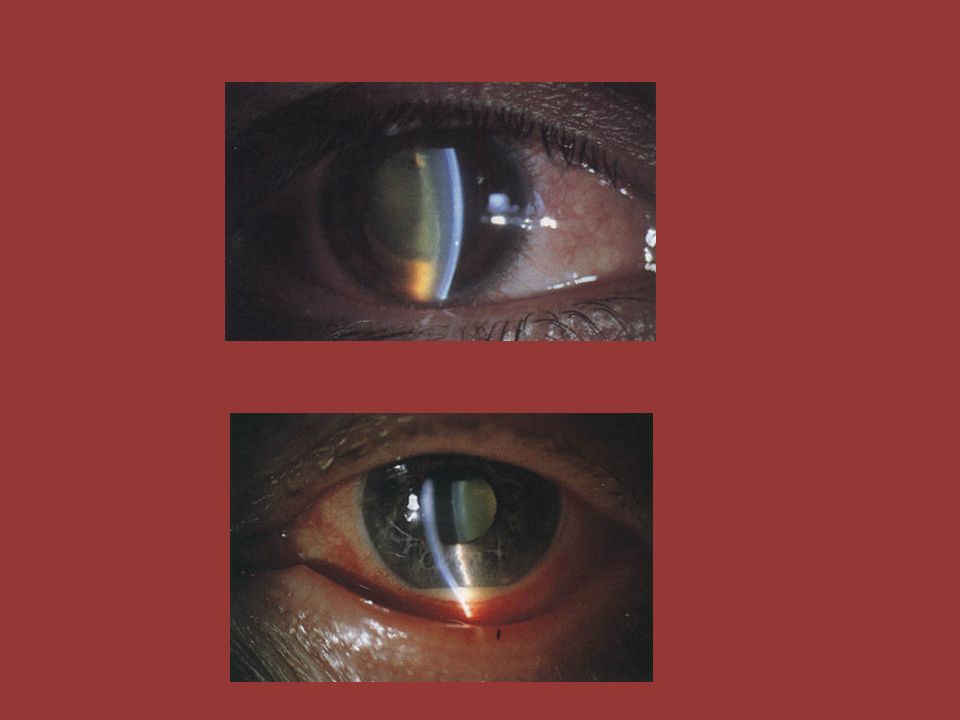
Clinical features Symptoms Signs Cicum-corneal congestion
Onset : Sudden Periocular pain and headache Bluring of vision Halloes around light due to corneal edema Redness of the eye Sometimes nausea and vomiting Signs Cicum-corneal congestion Corneal edema Shallow anterior chamber Mid-dilated ,fixed pupil IOP elevated

59
Treatment Admission to the hospital Medical treatment : Systemic Carbonic anhydrase inhibitors, initially Acetazolamide 500mg i.v. followed by 250 mg orally qds. Topical 2% pilocarpine qds. Topical 0.5% timolol bds. If IOP still high after one hour then hyper osmotic agent is given 20% mannitol 1-2 gm/kg i.v. over 45 minutes

60
After reducing IOP medically treatment is essentially by laser iridotomy in early cases without established PAS (to create an opening between the posterior chamber and anterior chamber and by pass the pupillary block). While in late cases with PAS, treatment is with surgical trabeculotomy to create an opening between the anterior chamber and sub-conjunctival space and by pass the PAS. The other eye must be prophylactically treated with laser iridotomy.

62
If urgent management is not given, there will irreversible damage to the optic nerve with permanent blindness

63
Secondary Closed Angle Glaucoma
1- Lens-related glaucoma 2- Neovascular glaucoma 3- Inflammatory glaucoma 4- Intra ocular tumor may push iris lens diaphragm forward and closing the angle

64
1-Lens-related glaucoma:
a- Phacolytic glaucoma. b- Phacomorphic (Intumescent) glaucoma: b- Phaco anaphylactic glaucoma:
 glaucoma: b- Phaco anaphylactic glaucoma:")
65
a- Phacolytic glaucoma

66
b- Phacomorphic (Intumescent) glaucoma
 glaucoma")
67
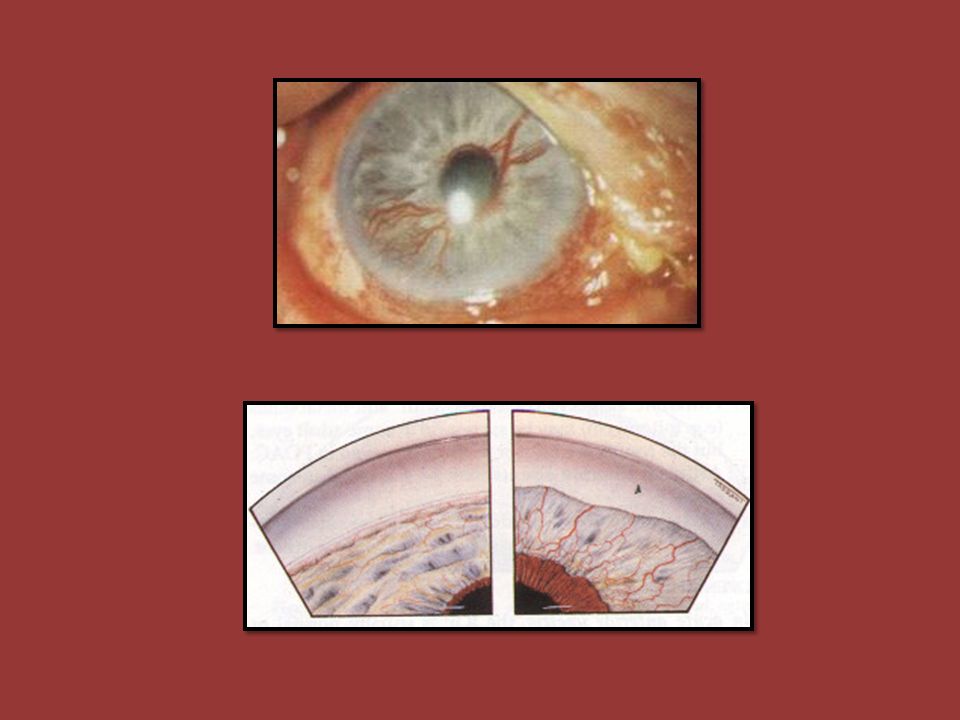
2- Neovascular glaucoma
Caused by rubeosis iridis associated with chronic, diffuse retinal ischaemia . Causes Central retinal vein occlusion. (commonest cause) Diabetes mellitus (proliferative diabetic retinopathy). Miscellaneous Carotid obstructive disease. Central retinal artery occlusion. Intraocular tumours. Long standing retinal detachment. Chronic intraocular inflammation.
 Diabetes mellitus (proliferative diabetic retinopathy). Miscellaneous. Carotid obstructive disease. Central retinal artery occlusion. Intraocular tumours. Long standing retinal detachment. Chronic intraocular inflammation.")
69
Inflammatory glaucoma

70
Congenital Glaucoma Affect 1:10,000 births
True congenital glaucoma: represents (40%) of all congenital glaucoma 2- Infantile glaucoma: represents (55%) of congenital glaucomas, Juvenile glaucoma: represents (5%) of congenital glaucomas, 75% bilateral 65% male
 of all congenital glaucoma. 2- Infantile glaucoma: represents (55%) of congenital glaucomas, Juvenile glaucoma: represents (5%) of congenital glaucomas, 75% bilateral. 65% male.")
71
Clinical features Corneal haze. Buphthalmos.
Breaks in descement membrane. (Haab striae) Optic cupping
 Optic cupping.")
72
Diagnosis Corneal diameter IOP C/D ratio

73
Treatment Surgical Goinotomy . Trabeculectomy .

Similar presentations










 Giovanni Caboto Club October 3, 2012.>")

 FRCOphth Consultant Ophthalmic Surgeon 9 October 2014.>")




. Optic nerve head damage. Corresponding loss.>")








