Download presentation
Presentation is loading. Please wait.

2
Who is considered elderly? “Young old” 65-75 years “Old, old” >75 years

4
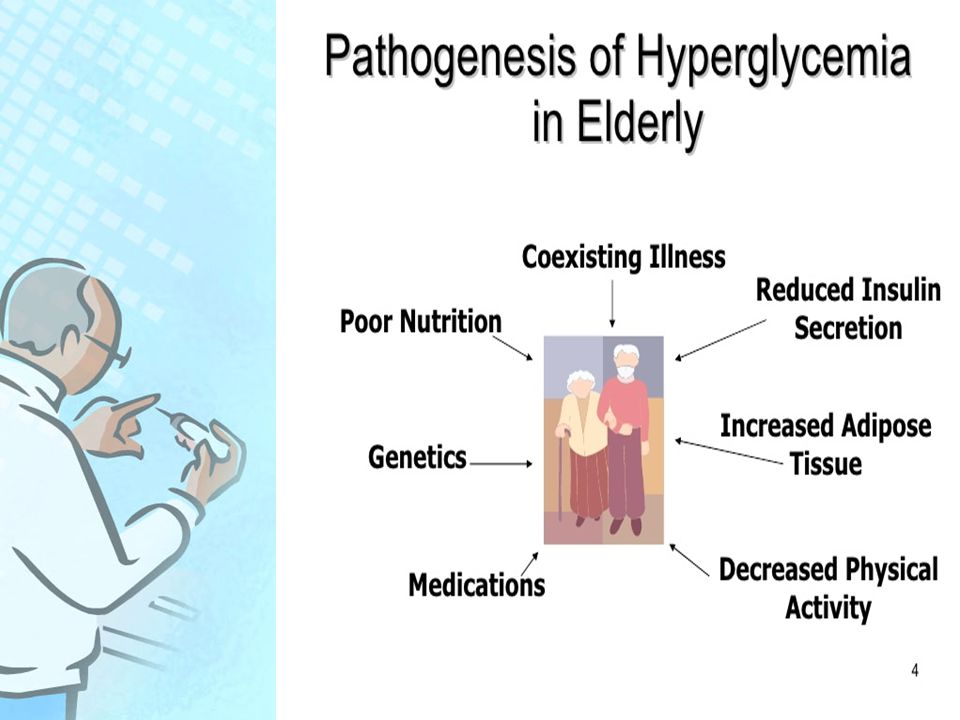
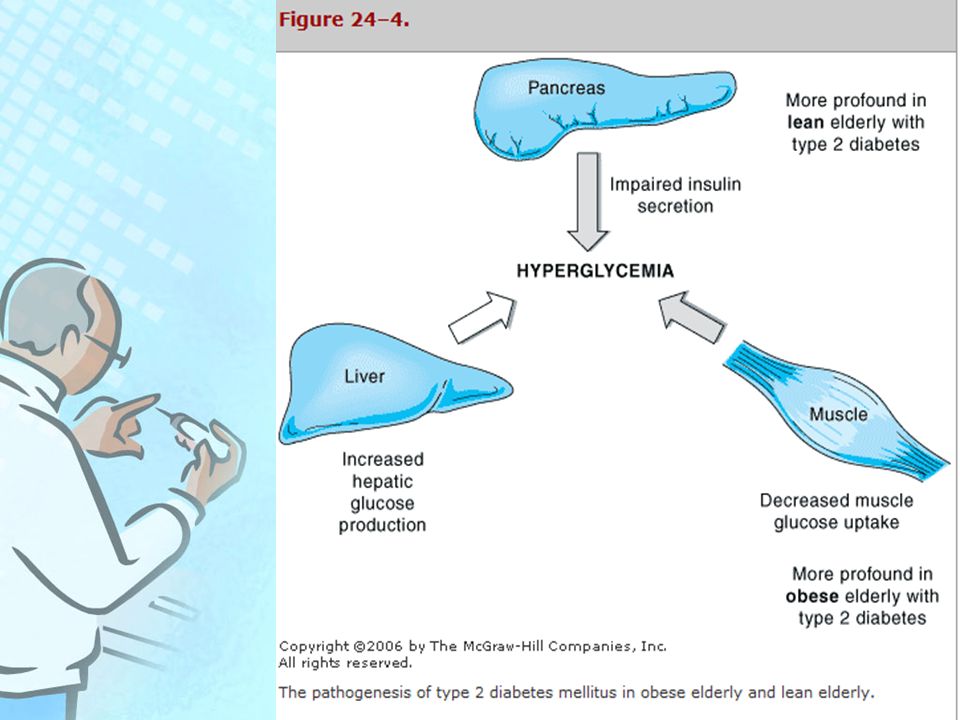
Why does Diabetes increase with Age? Changes in insulin secretion, action and hepatic glucose production with aging Genetic predisposition Medications that may change glucose metabolism (?thiazides?) Older patients more likely to be “lean” diabetics: more problem with insulin secretion than insulin sensitivity as seen in obese, middle aged diabetics Latent Autoimmune Diabetes of Adults: LADA
 Older patients more likely to be lean diabetics: more problem with insulin secretion than insulin sensitivity as seen in obese, middle aged diabetics Latent Autoimmune Diabetes of Adults: LADA.")
5
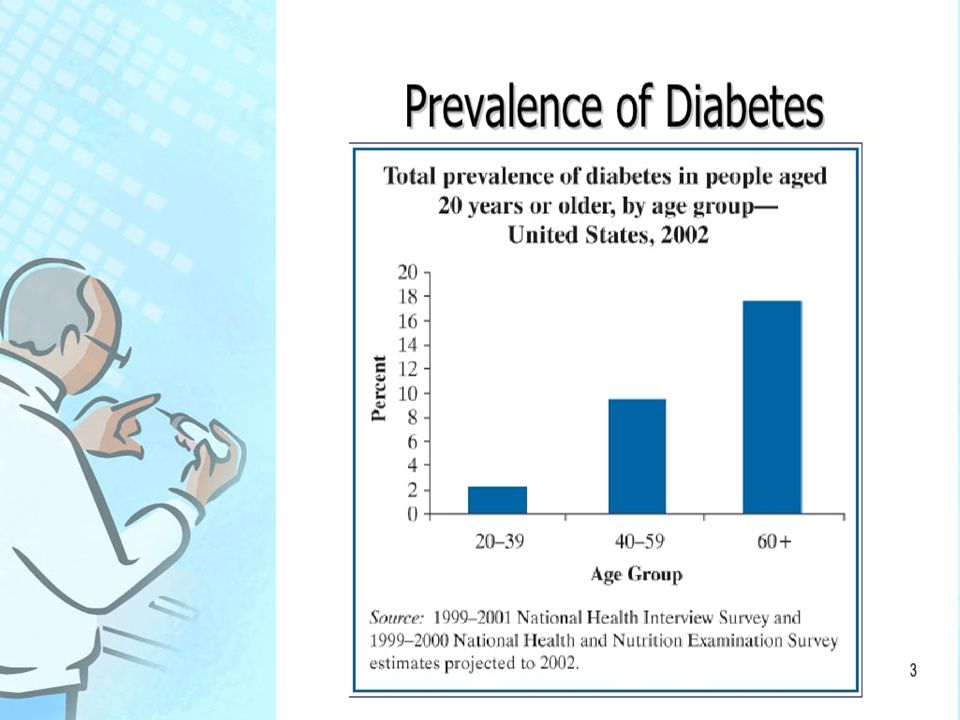
Even healthy elderly individuals :age-related increase in fasting blood glucose (1 mg/dL per decade). And increase in blood glucose (5 mg/dL per decade) in response to a standard glucose tolerance test. Nearly 10% of the elderly have some degree of glucose intolerance.
 in response to a standard glucose tolerance test. Nearly 10% of the elderly have some degree of glucose intolerance..")
8
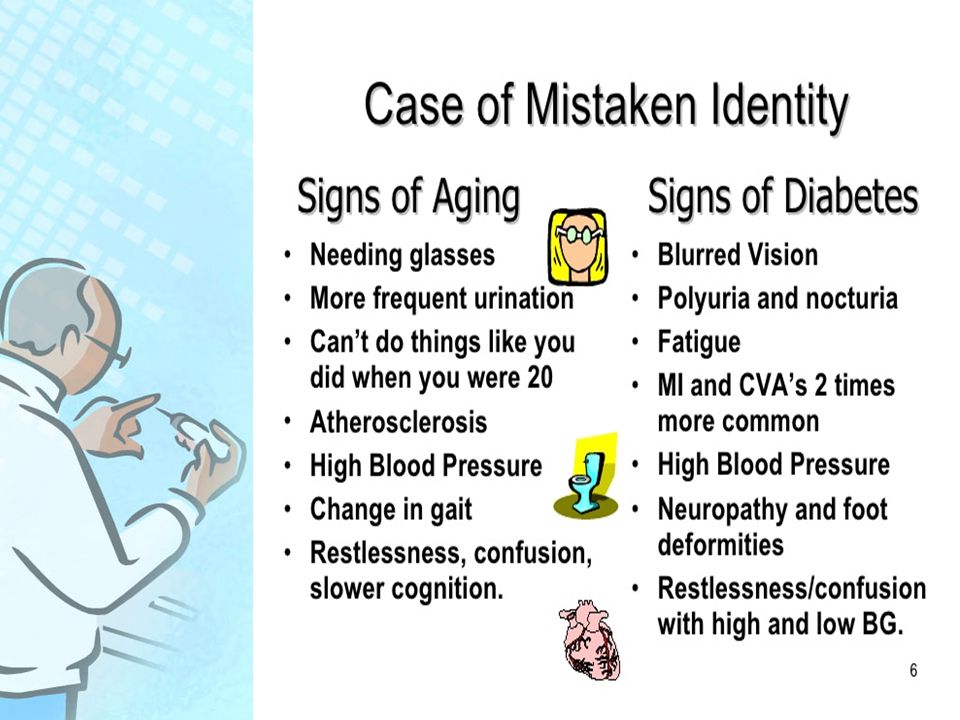
Most diabetes in the elderly is type 2 diabetes Diabetes may be difficult to diagnose in the elderly because of its often atypical and asymptomatic presentation.

11
Signs and symptoms of Type 2 Excessive urination Thirst Recurrent infections / Thrush Tiredness / Drowsiness Weight change Blurred vision Hyperglycaemia Dehydration Urinary ketones Glycosuria

12
ADA criteria are NOT adjusted for age

13
Case detection and diagnosis Asymptomatic elderly people should be screened for undiagnosed diabetes by measurement of fasting plasma glucose as recommended for the general population

14
Screening Review >>45 and older every 3 years, Risk factors: Family history of coronary heart disease, Cigarette smoking Hypertension Obesity Kidney disease Dyslipidemia.

15
Aging and Diabetes Poor diabetes control exacerbates the aging process. Poor diabetes control causes age related disease to develop earlier. Poor diabetes control makes co – morbid conditions worse and harder to manage.

16
Treatment Recommendations Glycemic Control Hypertension Lipids Tobacco cessation Eye care Foot care Nephropathy Diabetes Self-Management Training

17
Treatment goals for diabetes Symptom free Prevent short term complications Prevent long term complications Quality of life =Lifestyle focus

18
Treatment Options Individualized Weigh risks of hyperglycemia with hypoglycemia No data that tight control prevents stroke or cardiovascular events or improves mortality in this age group Consider cost of medications, limited coverage Risk of “polypharmacy”, increased risk of side effects and drug-drug interactions Treatment must be practical: are there functional limitations that will make plan of care difficult

19
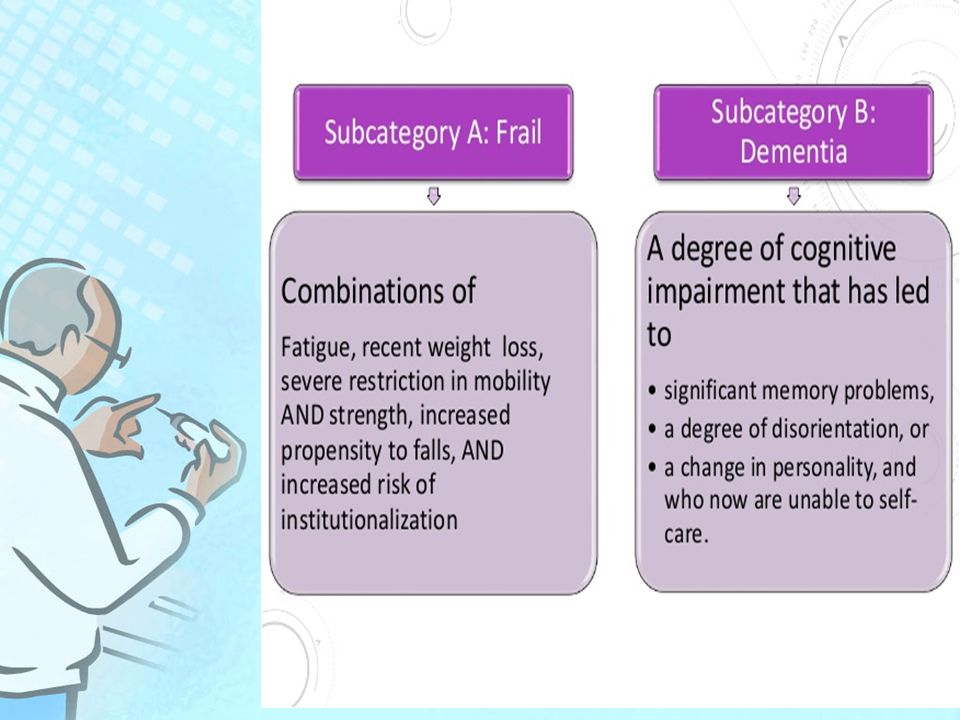
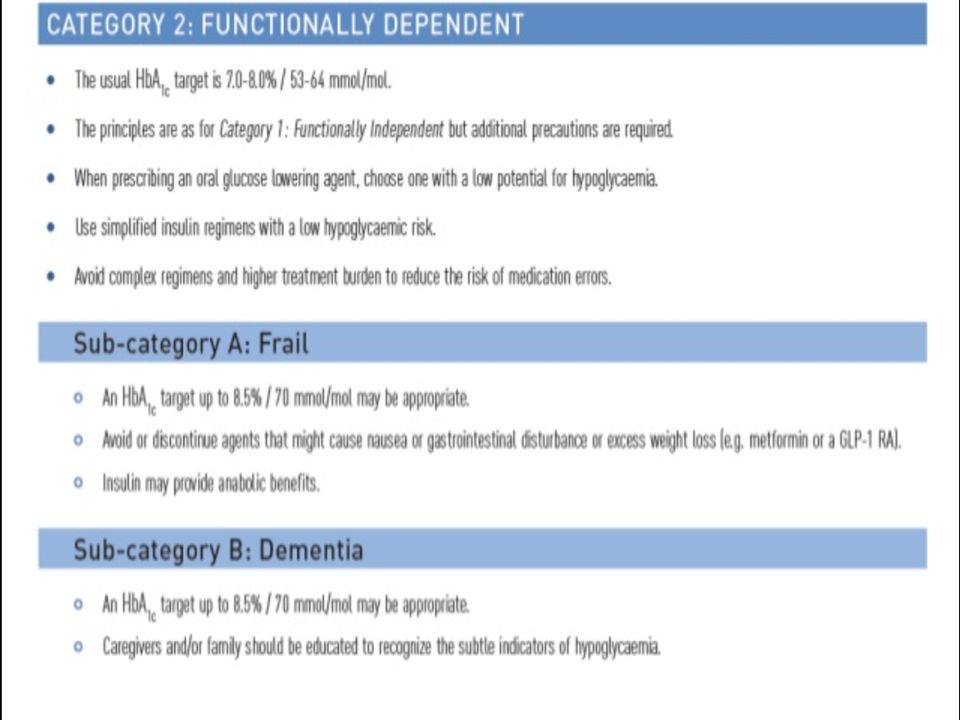
Guidelines focus Guidelines focus on “healthy” person with diabetes over the age of 65 years Needs of “frail” elderly should be considered on individual basis with special consideration of physical and mental status

20
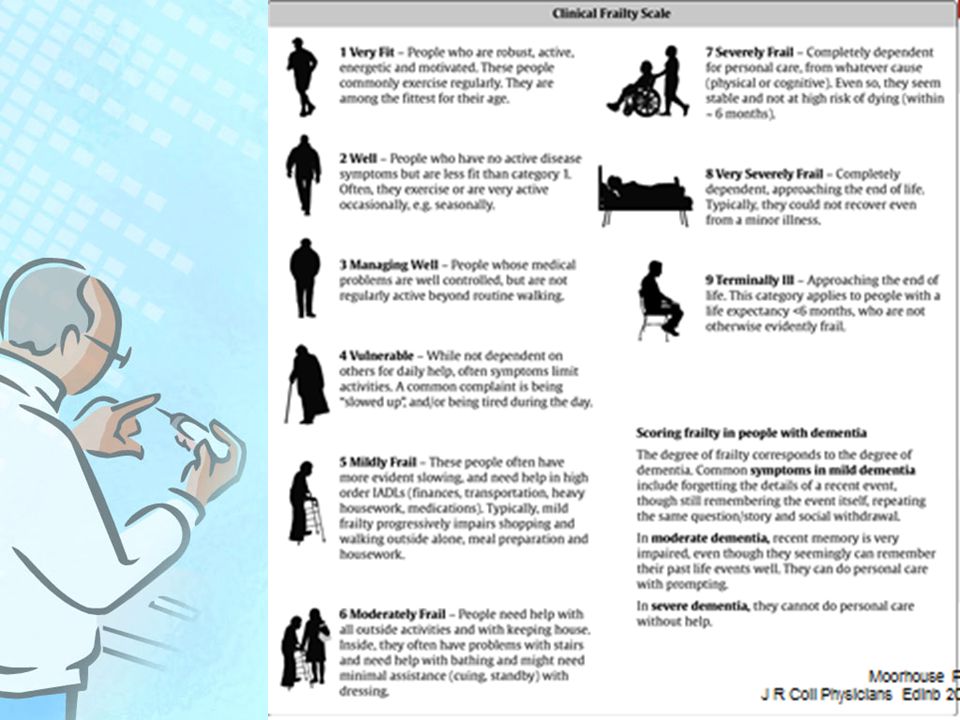
Functional categories of older people with diabetes

21
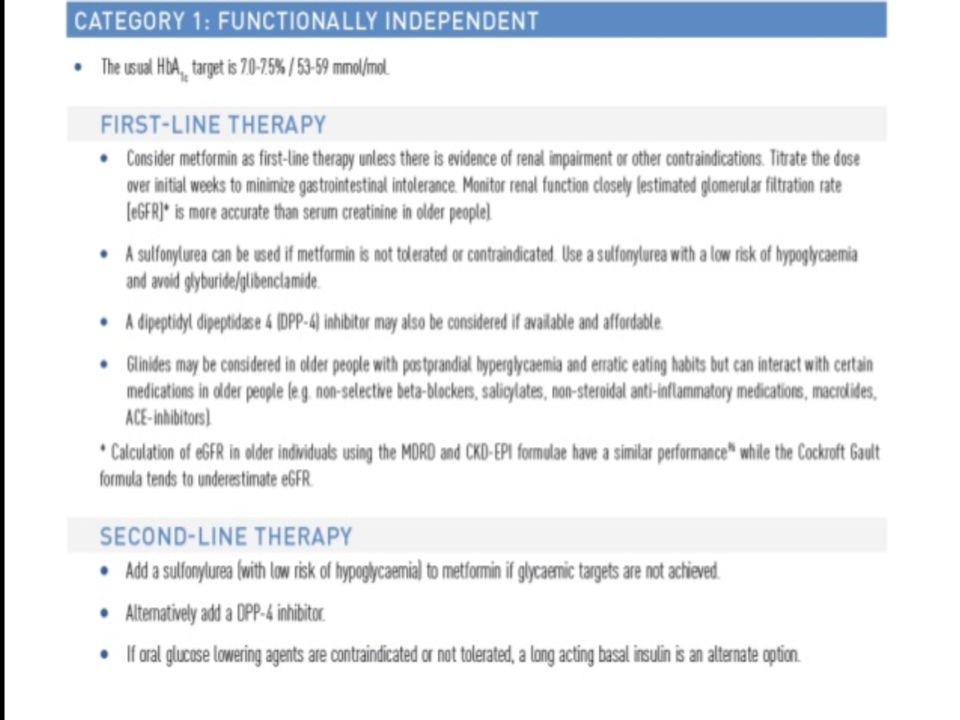
Category1: Functionally independent This category is characterized by people who are living independently have no important impairments of activities of daily living (ADL ), and who are receiving non or minimal caregiver support
, and who are receiving non or minimal caregiver support")
22
Category 2: Functionally dependent This category represents those individuals who, due to loss of function, have impairments of ADL. This increases the likelihood of requiring additional medical and social care. Such individuals living in the community are at particular risk of admission in HOSPITAL

24
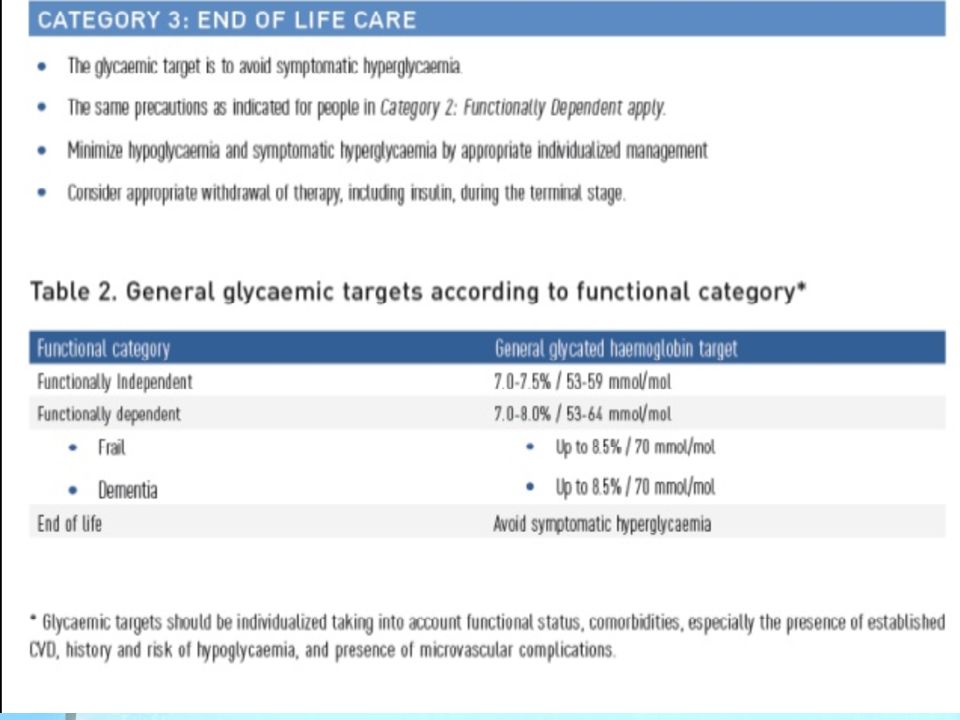
Category 3: end of life care These individuals are characterized by a significant medical illness or malignancy and have a life expectancy reduced to less than 1 year

28
Controlling blood glucose levels Healthy Eating: Regular carbohydrate High in fibre Low in fat (particularly saturated fat) Low in added sugar Adequate energy /protein/fluids/ vits and mins
 Low in added sugar Adequate energy /protein/fluids/ vits and mins")
29
Special treatments Nutrition assessment Distribution and intake of carbohydrate important Weight loss not recommended unless > 20% above weight range Encouraged to follow National Physical Activity Guidelines: 30 minutes of physical activity each day (tailored for frail elderly)
")
30
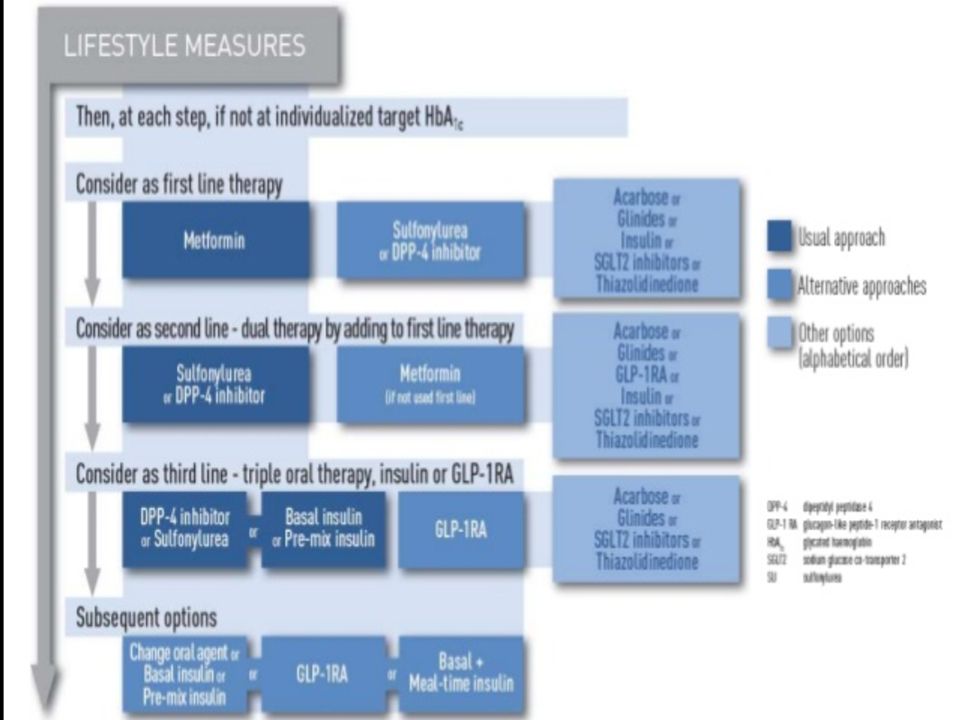
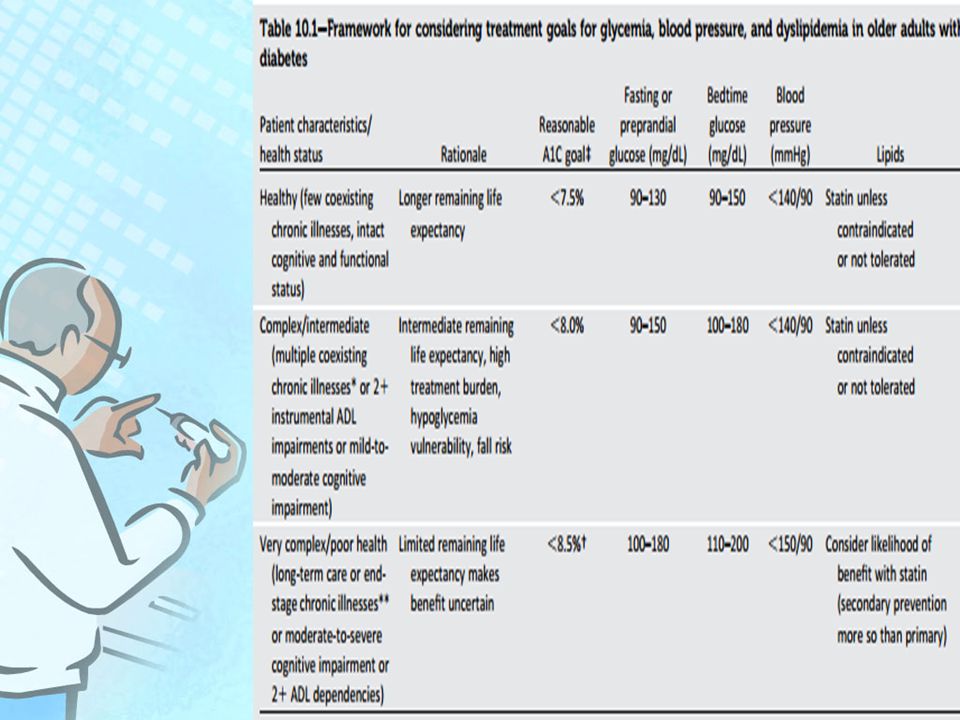
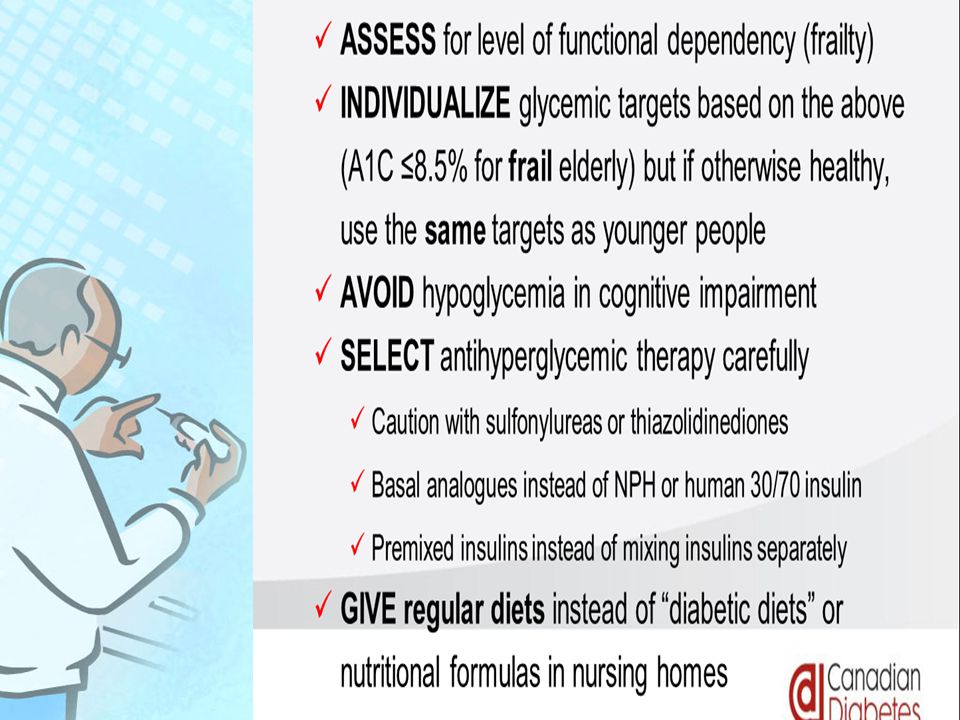
Recommendations :General Glycaemic control targets should be individualized taking into account functional status,comorbidities, history and risk of hypoglycaemia, and presence of complication. Begin oral glucose lowering therapy when lifestyle interventions alone are unable to maintain target blood glucose levels.

31
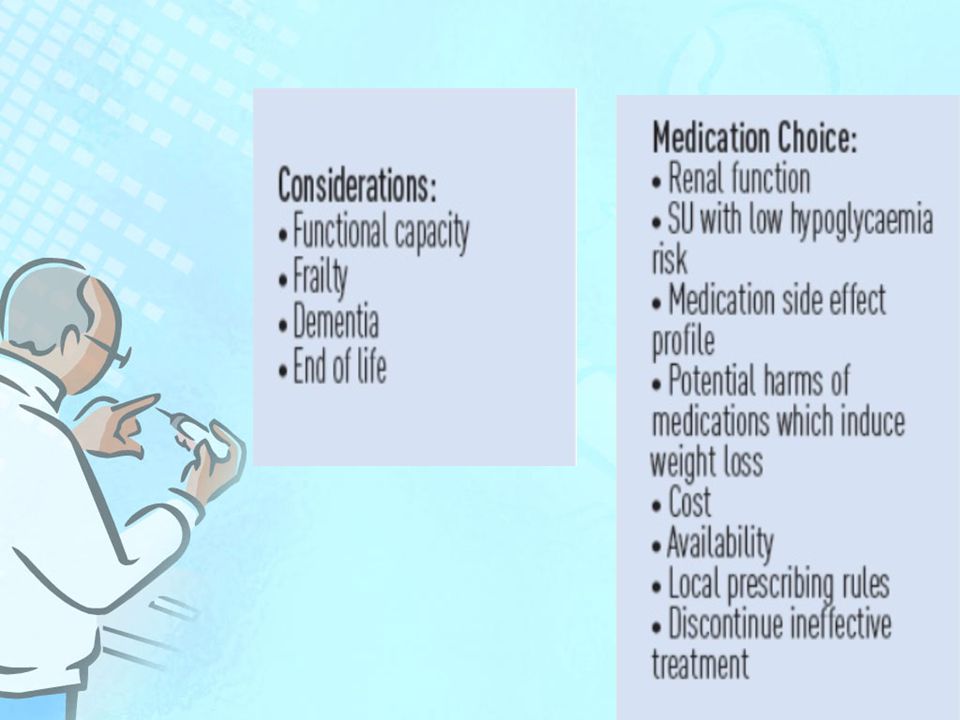
Use the “start low and go slow ” principle in initiating and increasing medication and monitor response to each initiation or dose increase for up to a 3 month trial period. Consider discontinuing ineffective and unnecessary therapies. Consider the cost and the risk- to – benefit ratio when choosing a medicine

47
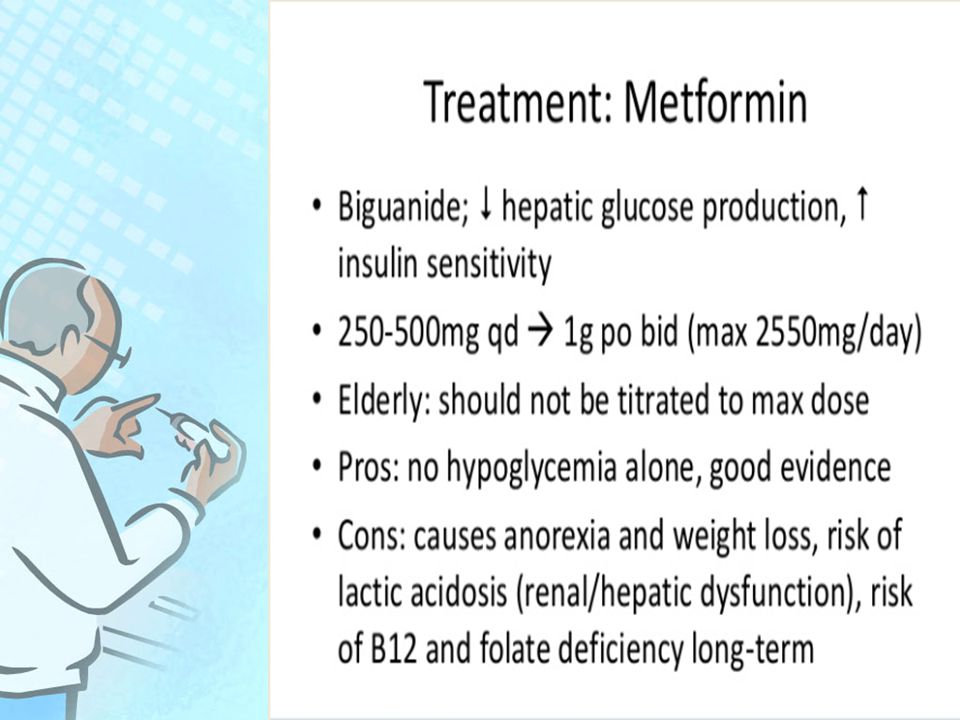
Lifestyle intervention is preferable to treatment with metformin in reducing the risks of type 2 diabetes In non – obese older adults with elevated fasting and postload plasma glucose levels

48
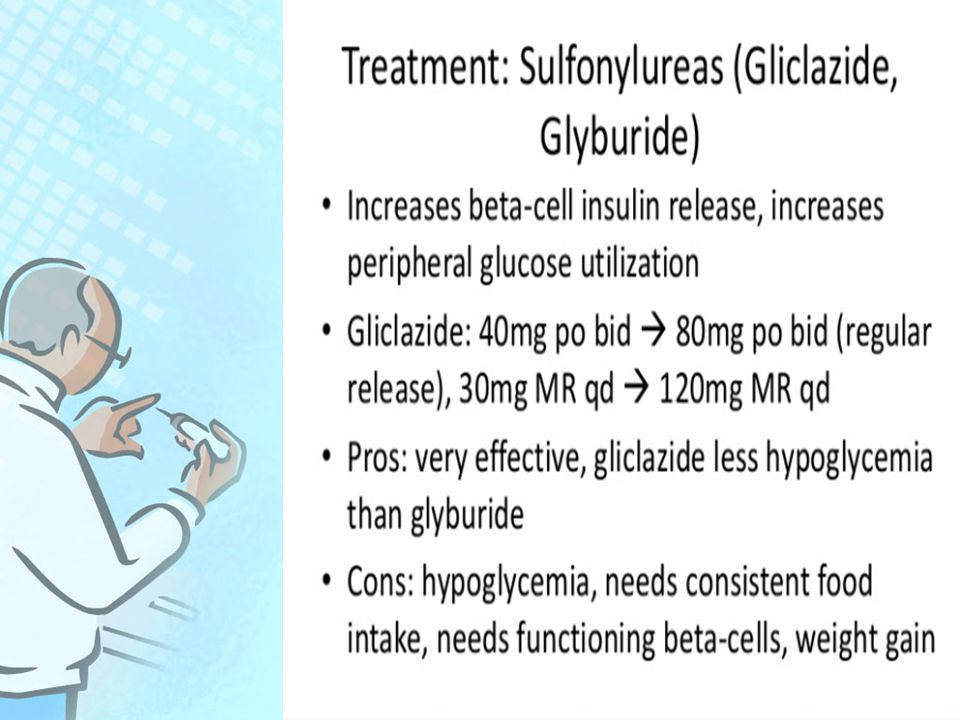
Metformin should normally be first line therapy for overweight older adults with type2 diabetes. In non- obese older people with diabetes first line therapy with an insulin secretagogue (normally a sulphonylurea ) or metformin should be offered
 or metformin should be offered.")
49
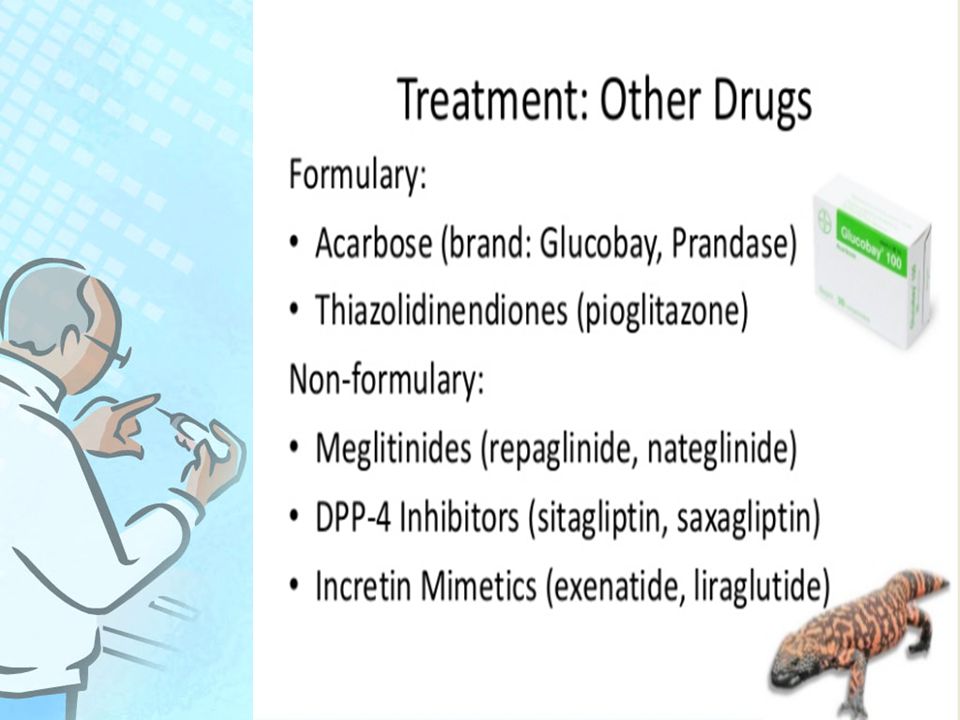
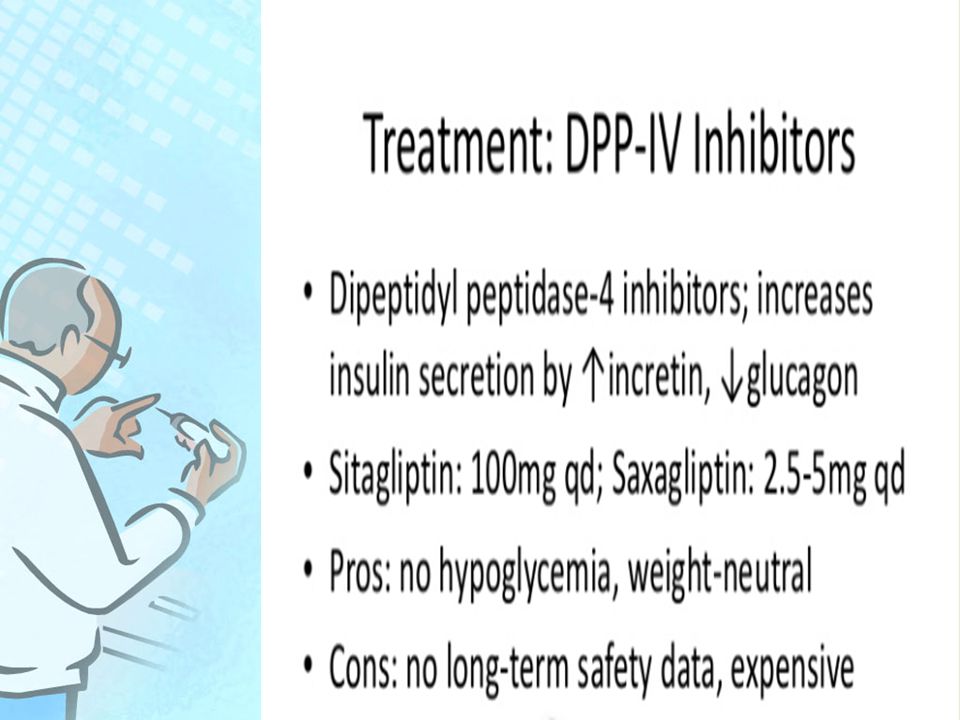
Glibenclamide should be avoided for newly diagnosed cases of type 2 diabetes in older adults (>70 years ) because of the marked risk of hypoglycaemia. Less risk :Glipizide, Glimepride. A DPP-4 inhibitor as an add-on to metformin when use of a sulphonylurea may pose an unacceptable hypoglycaemia risk can be considered in an older patient with diabetes.

50
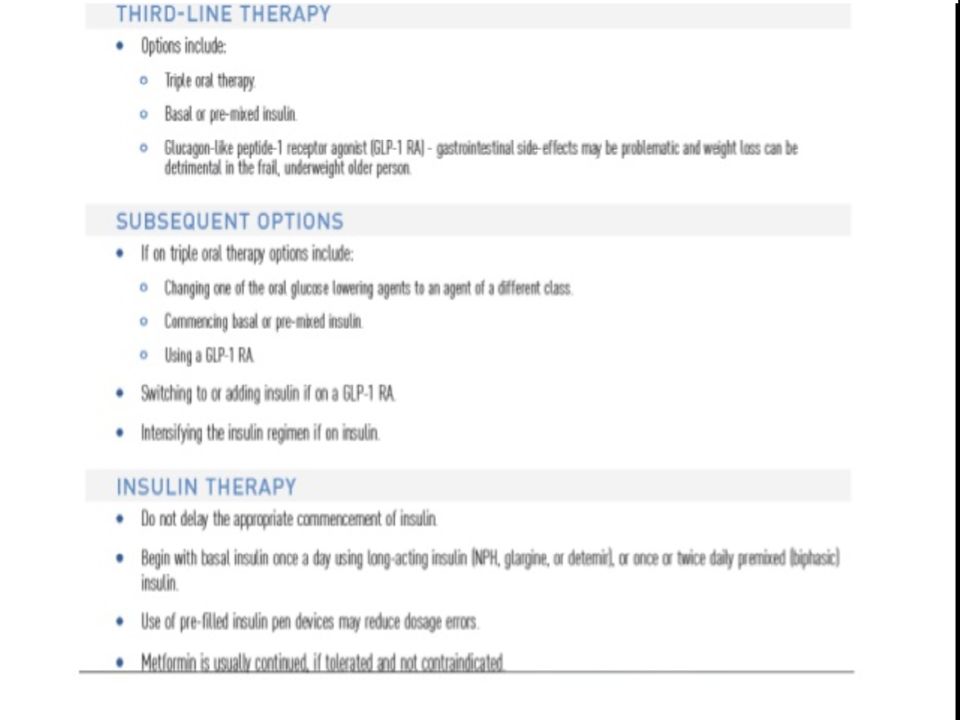
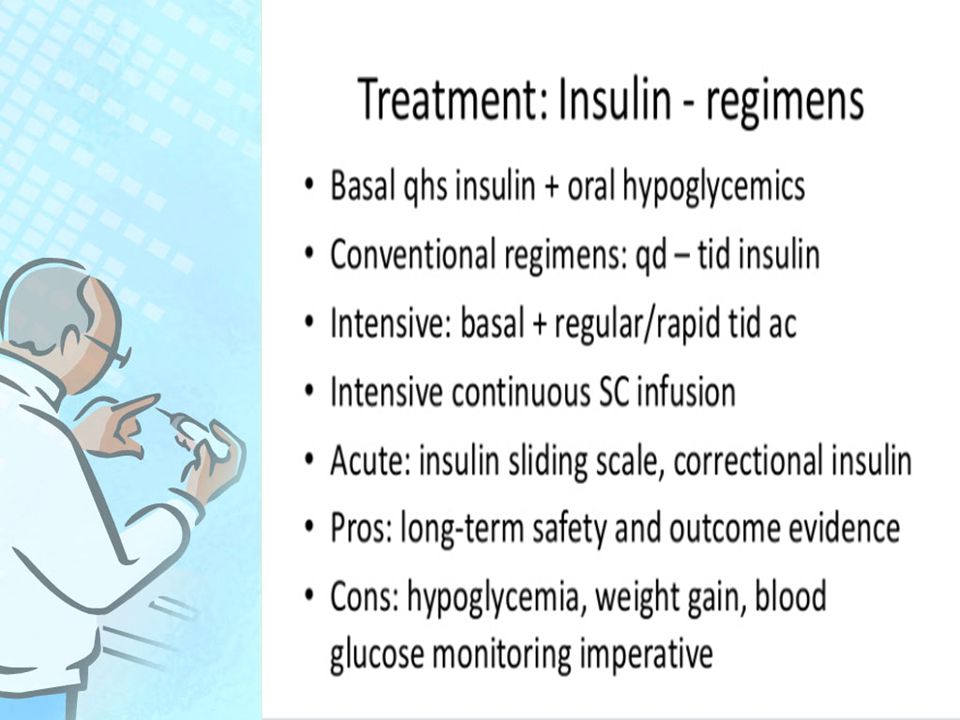
When oral agents fail to lower glucose levels adequately, insulin may be given either as monotherapy or in combination with a sulphonylurea or metformin. Use of a long – acting insulin analogue (e,g,glargin, determir ) rather than NPH- insulin should be considered in older patients
 rather than NPH- insulin should be considered in older patients.")
51
---If Choosing To Use Insulin

54
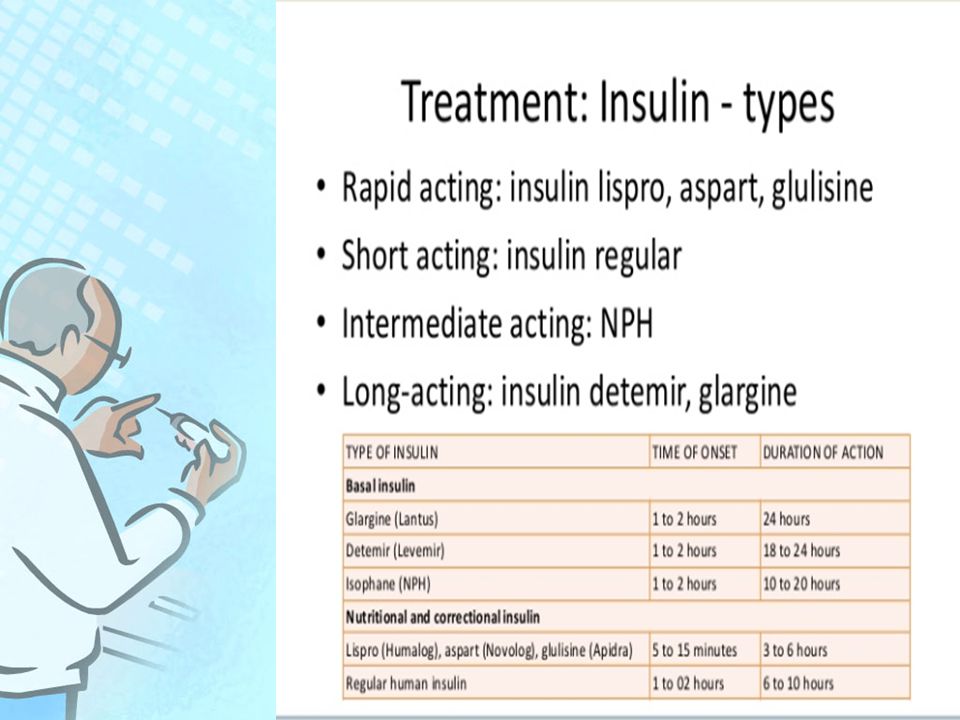
Glargine (lantus) insulin Long acting Often fear of hypoglycemia because long acting, especially in patients with renal insufficiency or unreliable po intake But studies demonstrating less risk of hypoglycemia, especially in patients with “brittle” diabetes and nocturnal hypoglycemia
 insulin Long acting Often fear of hypoglycemia because long acting, especially in patients with renal insufficiency or unreliable po intake But studies demonstrating less risk of hypoglycemia, especially in patients with brittle diabetes and nocturnal hypoglycemia")
55
Risks Of Intensive Glycemic Control Hypoglycemia Polypharmacy Drug to drug interactions Drug to disease interactions

57
In conclusion the aim in elderly people with diabetes is to Relieve symptoms of high glucose levels Avoid low glucose levels Achieve agreed blood glucose levels Monitor diabetes complications Encourage health and fitness habits Ensure older people are actively involved in setting goals for their diabetes management

Similar presentations





 Fellow of KIMS Endocrine, Diabetes and Metabolism.>")









 and Drug Therapy in Different Risk Categories Risk Category LDL Goal (mg/dL)>")




