Download presentation
Presentation is loading. Please wait.

1
A UNDERSTANDING OF “THE SPECTRUM” AND THE CLINICAL IMPLICATIONS FOR THE FAMILY Understanding and Helping Families

2
Limited Family Therapy What has kept family therapy from being a common intervention with families on the spectrum?

3
Should Be A Perfect Match But few researchers, clinicians and theoreticians have established a recognized field Obvious pockets of care, but not widely available

4
But, what else is at play? Possible power versus possible powerlessness What is the impact of parental interaction on behavior?

5
Political Issue How to discuss this question without raising guilt? Understanding how family interaction can be improved must have certain advantages, even if “the patient” does not appreciably change.

6
Therapist must believe… The neurological difference may or may not be susceptible to change based on family change. True systems thinking removes blame.

7
Holding Values Slife, 2007 One does hold values, it is the abuse of values which is a problem. If one loves someone on the spectrum (parent, sibling, extended family, close friend, wonderful client, student…) they will hold a value that reflects a view.
 they will hold a value that reflects a view..")
8
Gurman and Kirshen, 1981 Is It Effective? YES MFT is efficacious and FT is often more effective or as effective an individual when the problem is attributed to a family conflict. Both behavioral and non-behavioral were superior (2/3) to no treatment
 to no treatment.")
9
Mechanisms of Change in FT 1. Multiple perspectives on the problem 2. Members were able to shift blame from one individual 3. Impasse Resolution-cases whereby the family moves from the problem state (arguing over behavior) to resolution (focus shifts to relational nature of problem)
 to resolution (focus shifts to relational nature of problem).")
10
Mechanisms of Change (cont.) 4. Therapeutic Alliance-basically a position of collaboration 5. Reduction of Within-Session Negativity (more reframing and balance). This would further result in more verbal discussions and less defensiveness. 6. Improved interactions and behavioral competency.
. This would further result in more verbal discussions and less defensiveness. 6. Improved interactions and behavioral competency..")
11
Research on This Exact Population. Virtually non-existent

12
Minor, but Intrusive Problem One’s embarrassed, one’s is public and an advocate The couple asks you, “what do we do when he is unwilling to go out to a restaurant, and I want us to still do fun things?”

13
Let Us Now Turn to the Family What is happening to them at that moment they officially hear the diagnosis?

14
Standard Responses to Diagnosis 1. Profound sadness 2. Anger 3. Defeated 4. Over-drive

15
Language Person with autism Person on the spectrum Autistic person In my view, all equal

16
Lost and gained Each family, and each member of a family must understand that which was lost and that which was gained with the birth of a autistic family member. Each person with autism is strikingly different, thus, no one can predict what particular factor is most or least difficult to accept.

17
Reponses Hear them The continued healing effect of empathy The challenge of remaining empathic to people who hold different positions The process is not identical for different people Don’t be so quick with intervention because it may appear dismissive

18
The Family with Autism While their child may meet diagnostic criteria they are likely to be looking for another perspective and a “reality check.” Will you take my son’s (daughter’s) concern seriously, and provide him (her) some comfort?
 concern seriously, and provide him (her) some comfort")
19
Three Theoretical Foci of Family Therapy All are systemic Problem-Focus The problem that brings them in Interactional Patterns of interaction that create tension Intergenerational “Bruises” caused by some past relationship, trauma or deficit

20
Possible Sequence Couple Individual on the spectrum Sibling Family Possible extended family

21
In my opinion, begin with the couple. Getting to know them Getting a very clear sense of the family, with special attention to getting a complete understanding as to the personality and style of the child or young adult with autism. Providing some education, if requested and the therapist knows the literature or multiple anecdotal cases in that area.

22
Autism is a Spectrum This we know, but what does that really mean? Each kid has: Particular Mood Sensory Specific social relatedness Anxiety Some repetition compulsion Communication (the area we can best address in order to serve all the others)
.")
23
One brief screening devise is used with the couple Three primary purposes Assist therapist in being able to best connect with young person Assess, very casually, if the view of this family member generates disagreement or mutual support This can assist in producing goals and a clinical direction for the work with the family.

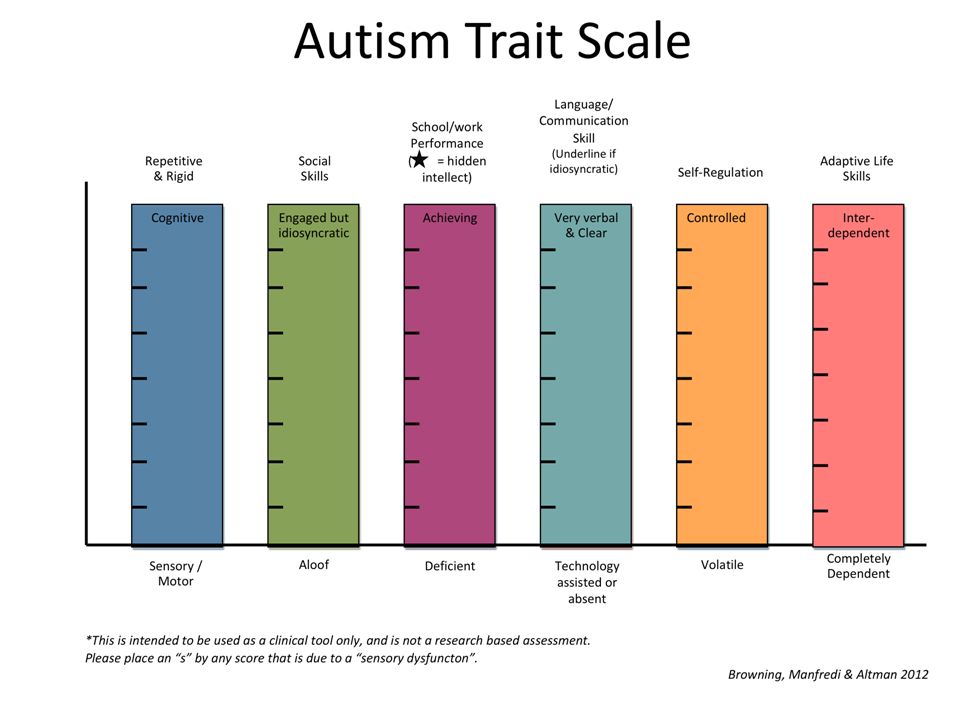
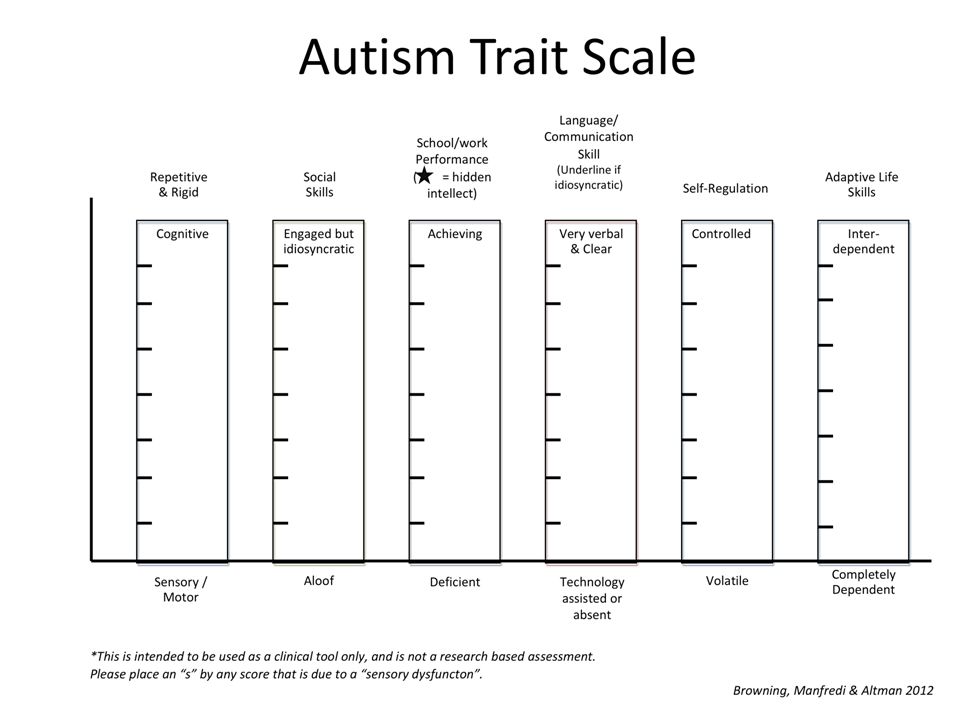
24
Autism Trait Screening Addresses six primary areas. Social Skills OCD or Repetitive Thoughts Academic/Work Skills Communication Outbursts/Emotional Regulation Level of Independence/Dependence Has three additional questions that provide important clinical information

27
Follow-up Questions How publically visible is the disorder for your child? What is the degree to which the symptom interferes with daily life? Are there other psychological conditions that merit attention? Please describe the actual behavior or thought noted in the “Repetitive & Rigid Scale.” If there are volatile incidents, do they ever become physical?

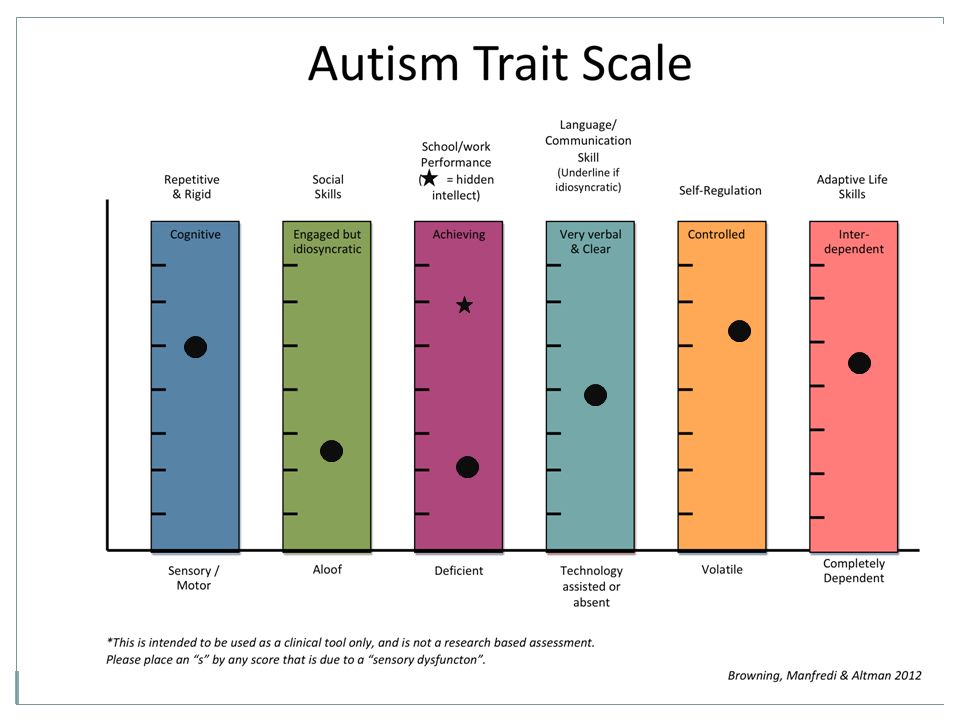
28
Matching possible parental reactions to positions on the graph This is not to label, but to normalize Differences in opinion are important, especially between family members

29
OCD/Repititions The more public the more the question is asked: “Do I need to inform this person about my child’s special needs.” “How do I react when a child innocently mentions it.” It helps to prepare (actual answer & feelings)
")
30
Social “Do I encourage friendship with kids who are more typical?” “Do we engage social skills group?” “How much do I explain to my child about their style and the effect of that style?”

31
Academic “Why don’t school personnel find a way to tap this extraordinary skill (even if the skill is remembering tons of dialogue from Disney)?” “Why can’t they understand his (her) behavior instead of only reacting to behavior.” “Why, on the occasion when they do look beyond the behavior is there idea always regarding medication?”
 Why can’t they understand his (her) behavior instead of only reacting to behavior. Why, on the occasion when they do look beyond the behavior is there idea always regarding medication")
32
Communication “How much do I interpret?” “How much, literally what percentage o his (her) verbalization is gibberish?” “How often to assist others in communicating with him or her?” “Is there some humor tucked inside there?”
 verbalization is gibberish How often to assist others in communicating with him or her Is there some humor tucked inside there")
33
Regulation/Outbursts Very tricky A real question of walking the balance of learning more or hoping for a natural calming. Safety Ross Greene, Ph.D. “The Explosive Child”

34
Level of Life Skill “How do I know when to push, and when to accept?” “Since we used books in the past that had developmental milestones to look for, how do we adjust?” “How do we agree on ‘level of independence’ when we have such different level of fear?” What is one skill that would be really helpful in the family?

35
The Session with the Parents Listen Comfort Educate About autism About systems Prioritize Reframe By understanding personal reactions Create new paradigms by using sub-systems

36
The next session is often with the autistic family member The first and foremost priority is to be fully aware of all the points the young person is making. If you are confused, carefully request clarifying details. Assess any workable problems Get permission to discuss together with parents Affirmation, Assignments or Summary

37
Siblings Research suggests generally positive findings Support groups for siblings are common until about age 13 Possible split session or separate session for the sibling

38
Next session may be with whole family Not an absolute, but if possible and there is no strong reason to leave out members. A clarity of issues and open family discussion about dealing with certain concerns. Even problems that seem peculiar, should be calmly understood and able to benefit from clinical interventions.

39
Caveat Due to some of the characteristics of the autistic member, if a meeting will simply create heightened anxiety, then the session includes only the young adult with autism and his (her) parent(s). Expressed anxiety is to be avoided, unlike in traditional family therapy.

40
The Johnson Family The Miller Family Outbursts in school Difficult to break routine Some outbursts at home Solid couple, reasonably supportive extended family Sibling tension-within normal range Parental disagreement Different agenda Non verbal, some outbursts Typical job issues (parent) Very different extended family reactions Two Cases
 Very different extended family reactions Two Cases")
41
Johnson Family Thomas x Rebecca JillJeffery

43
Therapy Session with parents confirmed the parents were a nervous, but very committed team. They wanted the best for their “sensitive kid,” but they were unsure how to trust or deal with the school. Session with Thomas and his parents emphasized efforts toward tantrum control, group therapy, and parental clarity. Session with parents and Rebecca to confirm an understanding of her issues.

44
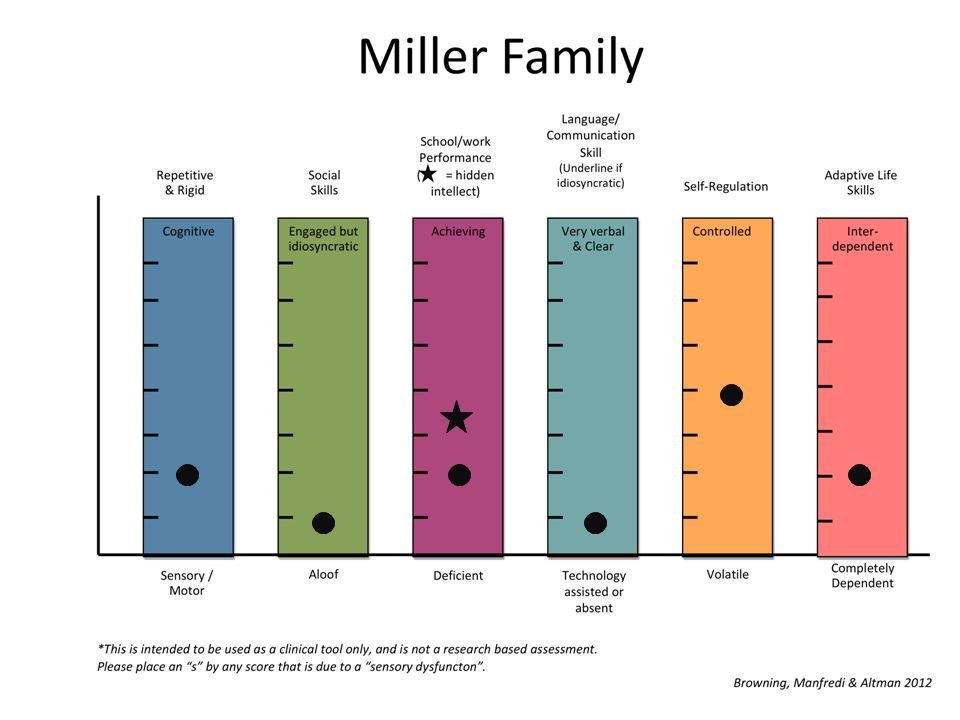
Miller Family – In College – Lives in a residential setting – No verbal skills – Goes home for weekends Bet h David

46
Therapy Sessions with parents first clarified the concern, determined a desire to stay married, agreed to slightly different parenting patterns. Session with whole family. Thomas brought his “talker” and questions included him. He does like his brother’s visits (a clear statement in session). Stress reduction
. Stress reduction.")
47
How is your role different? More of a consultant You are still doing therapy, but their needs are often unique Critical importance of being a “concerned contact.” Feel close caring people—fully understanding Advocate Look for self-cutoff which might be unnecessary

48
What is consistent with standard family therapy? IP may not be the primary issue or problem Systemic patterns are still very relevant Clarify communication and open channels where possible Increase empathic feeling throughout family Support and affirm Normalize, when appropriate and accurate Reframing, when honest and appropriate, can be extremely useful

49
Example of Common Reframe Parent is working on not being angry with the child. “Dusty is teaching you the value of patience. You know that if you blow-up, even slightly, you will be discussing it for a month. It may not be the way you intended to learn how to become calm, but you are learning how to be much more calm.” A good reframe is always true.

50
Family Therapy: Adding to a Spectrum of Options If sometimes your family life feels like “Theatre of the Absurd,” it is nice to have a non-judgmental person who can laugh with you, not at you, nor feel overwhelmed by pity. Family therapy provides a welcoming environment where the goal is to understand everyone, clarify the challenge, and provide multifaceted interventions.

51
Thank You. Questions? Scott Browning, Ph.D. Professor Department of Psychology Chestnut Hill College scobrown@chc.edu

52
Diagnostic Criteria for Autistic Disorder According to DSM IV-TR A. A total of six (or more) items from (1), (2), and (3), with at least two from (1), and one each from (2) and (3): 1. qualitative impairment in social interaction, as manifested by at least two of the following: a) marked impairment in the use of multiple nonverbal behaviors such as eye-to-eye gaze, facial expression, body postures, and gestures to regulate social interaction b) failure to develop peer relationships appropriate to developmental level c) a lack of spontaneous seeking to share enjoyment, interests, or achievements with other people (e.g., by a lack of showing, bringing, or pointing out objects of interest) d) lack of social or emotional reciprocity 2. qualitative impairments in communication as manifested by at least one of the following: a) delay in, or total lack of, the development of spoken language (not accompanied by an attempt to compensate through alternative modes of communication such as gesture or mime) b) in individuals with adequate speech, marked impairment in the ability to initiate or sustain a conversation with others c) stereotyped and repetitive use of language or idiosyncratic language d) lack of varied, spontaneous make-believe play or social imitative play appropriate to developmental level 3. restricted repetitive and stereotyped patterns of behavior, interests, and activities, as manifested by at least one of the following: a) encompassing preoccupation with one or more stereotyped and restricted patterns of interest that is abnormal either in intensity or focus b) apparently inflexible adherence to specific, nonfunctional routines or rituals c) stereotyped and repetitive motor mannerisms (e.g., hand or finger flapping or twisting, or complex whole-body movements) d) persistent preoccupation with parts of objects B. Delays or abnormal functioning in at least one of the following areas, with onset prior to age 3 years: (1) social interaction, (2) language as used in social communication, or (3) symbolic or imaginative play. C. The disturbance is not better accounted for by Rett's Disorder or Childhood Disintegrative Disorder.
 items from (1), (2), and (3), with at least two from (1), and one each from (2) and (3): 1. qualitative impairment in social interaction, as manifested by at least two of the following: a) marked impairment in the use of multiple nonverbal behaviors such as eye-to-eye gaze, facial expression, body postures, and gestures to regulate social interaction b) failure to develop peer relationships appropriate to developmental level c) a lack of spontaneous seeking to share enjoyment, interests, or achievements with other people (e.g., by a lack of showing, bringing, or pointing out objects of interest) d) lack of social or emotional reciprocity 2. qualitative impairments in communication as manifested by at least one of the following: a) delay in, or total lack of, the development of spoken language (not accompanied by an attempt to compensate through alternative modes of communication such as gesture or mime) b) in individuals with adequate speech, marked impairment in the ability to initiate or sustain a conversation with others c) stereotyped and repetitive use of language or idiosyncratic language d) lack of varied, spontaneous make-believe play or social imitative play appropriate to developmental level 3. restricted repetitive and stereotyped patterns of behavior, interests, and activities, as manifested by at least one of the following: a) encompassing preoccupation with one or more stereotyped and restricted patterns of interest that is abnormal either in intensity or focus b) apparently inflexible adherence to specific, nonfunctional routines or rituals c) stereotyped and repetitive motor mannerisms (e.g., hand or finger flapping or twisting, or complex whole-body movements) d) persistent preoccupation with parts of objects B. Delays or abnormal functioning in at least one of the following areas, with onset prior to age 3 years: (1) social interaction, (2) language as used in social communication, or (3) symbolic or imaginative play. C. The disturbance is not better accounted for by Rett s Disorder or Childhood Disintegrative Disorder..")
53
Diagnostic Criteria for Asperger’s Disorder According to DSM IV-TR A. Qualitative impairment in social interaction, as manifested by at least two of the following: 1. marked impairment in the use of multiple nonverbal behaviors such as eye-to-eye gaze, facial expression, body postures, and gestures to regulate social interaction 2. failure to develop peer relationships appropriate to developmental level 3. a lack of spontaneous seeking to share enjoyment, interests, or achievements with other people (e.g., by a lack of showing, bringing, or pointing out objects of interest to other people) 4. lack of social or emotional reciprocity B. Restricted repetitive and stereotyped patterns of behavior, interests, and activities, as manifested by at least one of the following: 1. encompassing preoccupation with one or more stereotyped and restricted patterns of interest that is abnormal either in intensity or focus 2. apparently inflexible adherence to specific, nonfunctional routines or rituals 3. stereotyped and repetitive motor mannerisms (e.g., hand or finger flapping or twisting, or complex whole-body movements) 4. persistent preoccupation with parts of objects C. The disturbance causes clinically significant impairment in social, occupational, or other important areas of functioning. D. There is no clinically significant general delay in language (e.g., single words used by age 2 years, communicative phrases used by age 3 years). E. There is no clinically significant delay in cognitive development or in the development of age- appropriate self-help skills, adaptive behavior (other than in social interaction), and curiosity about the environment in childhood. F. Criteria are not met for another specific Pervasive Developmental Disorder or Schizophrenia.
 4. lack of social or emotional reciprocity B. Restricted repetitive and stereotyped patterns of behavior, interests, and activities, as manifested by at least one of the following: 1. encompassing preoccupation with one or more stereotyped and restricted patterns of interest that is abnormal either in intensity or focus 2. apparently inflexible adherence to specific, nonfunctional routines or rituals 3. stereotyped and repetitive motor mannerisms (e.g., hand or finger flapping or twisting, or complex whole-body movements) 4. persistent preoccupation with parts of objects C. The disturbance causes clinically significant impairment in social, occupational, or other important areas of functioning. D. There is no clinically significant general delay in language (e.g., single words used by age 2 years, communicative phrases used by age 3 years). E. There is no clinically significant delay in cognitive development or in the development of age- appropriate self-help skills, adaptive behavior (other than in social interaction), and curiosity about the environment in childhood. F. Criteria are not met for another specific Pervasive Developmental Disorder or Schizophrenia..")
54
Proposed DSM-V: ASD Persistent deficits in social communication and social interaction across contexts Reciprocity Poorly integrated verbal and non-verbal, understanding, lack of expressions, gestures and abnormal body language Deficits in maintaining relationships Restrictive, repetitive patterns of behavior, interests, and activities Stereotyped, repetitive motor and speech Excessive adherence to routines, or inability to change Unusual interest, or reaction in sensory aspects of the environment

55
Proposed Level 1 (Higher Functioning) Without supports in place, deficits in social communication cause noticeable impairments. Has difficulty initiating social interactions. Clear examples of atypical responses to social overtures. RRB’s cause significant interference with functioning. Resists attempts to be redirected from fixated interest.

56
Pro The diagnosis is now too broad; a more specific, spectrum-based description. The more you fully understand the spectrum, the better you understand autism.

57
Con It may remove services due to the change in diagnostic category. Many people’s identity is now connected to the word.

Similar presentations




 Cara Kimberg, M.S.>")















