Download presentation
Presentation is loading. Please wait.

1
Dr Amanda Landers Community Palliative Medicine Specialist

2
65 year old man Diagnosed with metastatic melanoma to axillary nodes and lung Presents with pain under the arm radiating down onto the anterior chest wall

3
Physiological Poor wound healing, weakness, muscle breakdown Immobilisation, increased risk of DVT/PE Splinted breathing, increased risk of chest infection Decreased gastric motility Tachycardia and hypertension

4
Psychological Anxiety Depression Insomnia Existential suffering which may lead to thoughts of euthanasia

5
Immunological Decreased natural killer cell counts ? Other effects on the immune system

6
Impending death Decreased enjoyment and quality of life Disability Suffering long-term Challenges to dignity Burden to others

7
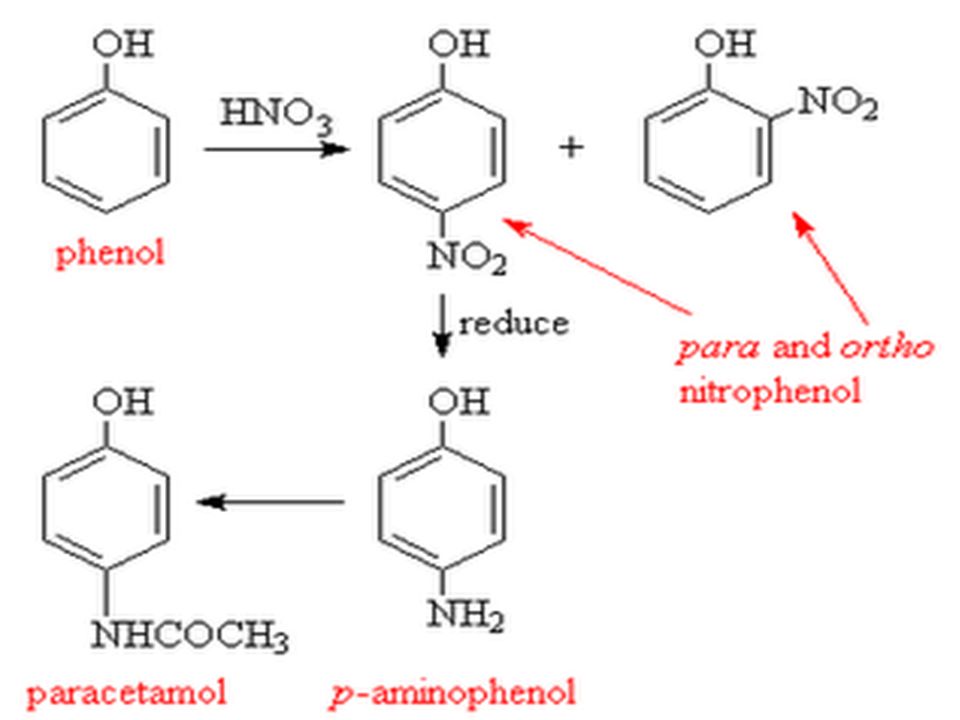
Man started on paracetamol 1gm QID Discussion on how this must be taken at breakfast, lunch, dinner and before bed Strongly encouraged to take regularly

8
paracetamol licensed by FDA 1950s dose 500mg – 1g 4 to 6 hourly for all maximum 4g in 24 hours for all

10
60kg, frail 84 year old woman1g QDS 106kg, 30 year old 1g QDS 70kg, 65 year old man1g QDS

11
maximum 4g in 24 hours

12
fit young 18 years to 30 years fit elderly > 65 years frail elderly> 65 years (+CVA or hospitalised)
")
13
fit young 18 years to 30 years CL100% fit elderly > 65 years CL70-80% frail elderly> 65 years CL50-55% (+CVA or hospitalised)
")
14
Maybe non frail elderly 1g TDS frail elderly 1g BD What about the 30 to 65 year olds?

15
Man admitted to hospital with worsening chest wall pain Oncology ward full so placed on an ‘outlying’ ward

16
Background: do differences exist in the management of cancer-related pain in patients admitted to oncology and non-oncology settings. Patients and methods: 48 Italian hospitals, 819 patients receiving analgesic therapy for cancer-related pain.

17
Results: non-opioids more frequently in non- oncology units (19.6% versus 7.0%; P < 0.0001) strong opioids are more frequently used in the oncology units (69.5% versus 51.9%; P < 0.0001). inadequate therapy was lower in oncology compared with non-oncology units Conclusion: Oncology wards provide the most adequate standard of analgesic therapy for cancer-related pain.

18
Man started on morphine regularly Switched to long-acting formulation GP mentions fentanyl patches to him in the community

19
Fentanyl Oxycodone Methadone (Hydromorphone) (Sufentanil) (Combination drugs)
 (Sufentanil) (Combination drugs)")
20
Short acting semi synthetic opioid Duration of action IV 30 to 60 mins “Clean” drug: Fewer CNS and GI side effects Routes : subcutaneous, transdermal, buccal sublingual, intrathecal Transdermal Fentanyl patches ( Durogesic ) 12, 25, 50, 75, 100mcg/hr strengths
 12, 25, 50, 75, 100mcg/hr strengths")
21
No hot water bottles on the patch or spa baths- above 40C they leach medication If skin irritated, use steroid inhaler on skin first After patch removed, medication still under the skin for 12-18 hours May need to be changed every 2 days in minority of patients

22
Semi-synthetic opioid similar to morphine More potent than morphine on mg to mg basis 1 mg oxycodone = 2 mg morphine Safe to use in mild renal impairment Clinically less CNS and GI side effects (not proven) Oral and parenteral formulations only Immediate and slow release preparations
 Oral and parenteral formulations only Immediate and slow release preparations")
23
Synthetic opioid; NMDA activity Oral to parenteral conversion usually 1:1 Still much confusion and controversy about pharmacokinetics; t1/2 varies from 12-150hrs! very potent and small doses should be prescribed “ Start low, go slow”. ?initiate in hospital setting

24
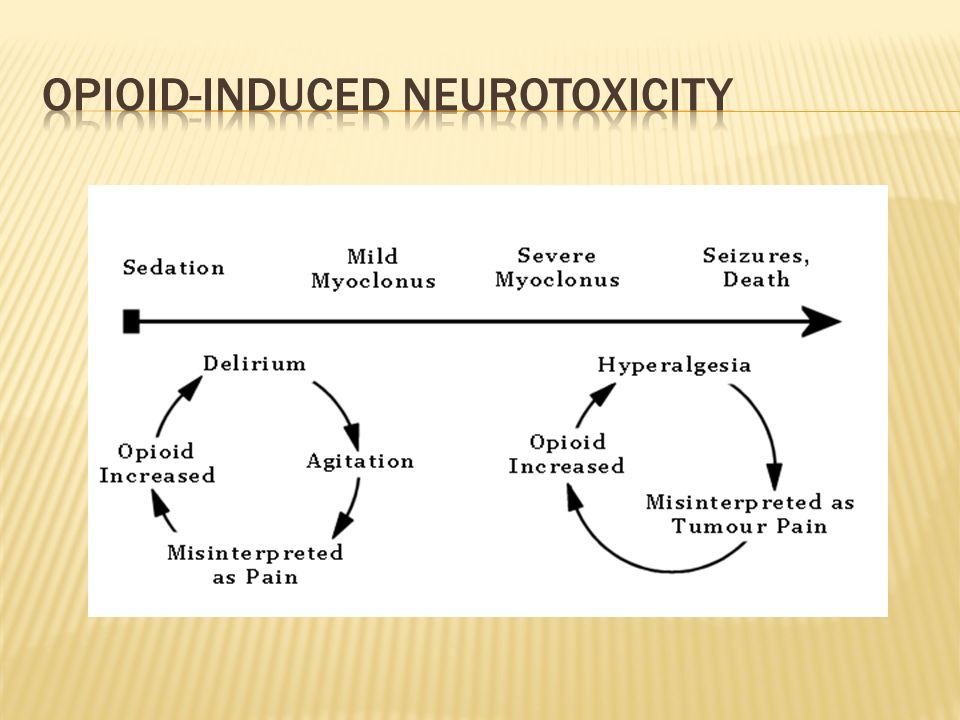
Man seen at home with severe neuropathic pain around the chest wall Was advised to take morphine elixir Q2H prn and he has had 5 breakthrough doses Sleepy, hallucinating, ‘twitchy’ Still in pain What now?

25
Indications Most common reason is inadequate pain relief with toxicity Cost Compliance Diversion concerns Rationale Incomplete cross-tolerance Differing genetic backgrounds Interdividual difference eg, GFR

27
Man rotated onto methadone in the hospice Neuropathic element to pain Co-analgesics also started

28
defined as “pain initiated or caused by a primary lesion or dysfunction in the nervous system” diverse set of syndromes changes may occur in the peripheral, central, and autonomic nervous system, and each can contribute to the development of chronic neuropathic pain.

29
Brachial plexus neuropathies Chemotherapy-induced neuropathy Cisplatin Oxaliplatin Paclitaxel Thalidomide Vincristine Vinblastine Postherpetic neuropathy Post-radiation plexopathies Surgical neuropathies Phantom pain Post-mastectomy syndrome Post-thoracotomy syndrome

30
Non-opioids Limited usefulness but may be worth a trial Opioids Co-analgesics Steroids Anti-convulsants Tricyclic antidepressants Systemic local anaesthetics Benzodiazepines

31
Used for nerve pain and depression Common side effects Dry mouth Blurred vision Urinary retention Drowsiness Lowers seizure threshold

32
Used for nerve pain Common side effects Easy bruising dizziness ataxia headache twitching peripheral oedema

33
Corticosteroid Used for raised intracranial pressure, nausea/vomiting, inflammation in a bowel obstruction, liver capsule pain with metastatic disease, appetite stimulation, fatigue Commonly causes insomnia Contraindicated in infections and GI bleeds

34
Used as an anti-epileptic In palliative care it is useful for nerve pain, anxiety, agitation, dypsnoea, hiccups Common adverse effects- fatigue, drowsiness Very potent, long-acting and its use should be closely monitored

35
SC lignocaine Affects sodium channels Contraindicated in hepatic dysfunction and severe cardiac rhythm disturbances

36
Discharged on 25mg nortriptylline, opioid and 300mg TDS gabapentin Recommended to GP that titration of gabapentin next step in pain management Close follow up in community

Similar presentations








. For CHRONIC pain, use a scheduled medication regimen. ( ex:>")




>")





