Download presentation
Presentation is loading. Please wait.

1
Spinal evaluation in children with imperforate anus
Simone Montoya, R1 December 15, 2011

2
Objective Anorectal malformations are often associated with vertebral and/or spinal cord abnormalities Fecal incontinence/constipation may be due to anorectal and/or neurological pathology Magnetic resonance imaging is the gold standard for spinal cord imaging, but sonography is an effective screening tool before ossification has taken place … So should a spinal MRI be part of the work-up of a newborn with an anorectal malformation?

3
Case: BS Born at OSH on 12/7/2011 Imperforate anus noted upon delivery
41wk GA Imperforate anus noted upon delivery Passing meconium through small defect in perineum anterior to presumed proper location of anus “Bucket handle” deformity Physical exam also notable for LGA and sacral dimple Underwent anoplasty on DOL1 Discharged to home on POD5

4
Perineal fistula Low-lying lesion

5
Anatomic Classification of Anorectal Malformations (Wingspread)
Female Male HIGH: (blind) rectal pouch above the pubococcygeal line Anorectal agenesis with/without rectovaginal fistula Anorectal agenesis with/without rectoprostatic urethral Rectal atresia INTERMEDIATE Rectovestibular fistula Rectobulbar urethral fistula Rectovaginal fistula Anal agenesis without fistula LOW: rectal pouch below the pubococcygeal line (within the levator ani) Anovestibular fistula Anocutaneous fistula Anal stenosis Rare/Cloacal malformations
 rectal pouch above the pubococcygeal line. Anorectal agenesis with/without rectovaginal fistula. Anorectal agenesis with/without rectoprostatic urethral. Rectal atresia. INTERMEDIATE. Rectovestibular fistula. Rectobulbar urethral fistula. Rectovaginal fistula. Anal agenesis without fistula. LOW: rectal pouch below the pubococcygeal line (within the levator ani) Anovestibular fistula. Anocutaneous fistula. Anal stenosis. Rare/Cloacal malformations.")
6
VACTERL Association Anomalies not pathogenetically related, but occur together more frequently than expected by chance Vertebral anomalies Anal atresia Cardiac defects TracheoEsophageal fistula Renal malformations Limb defects VATER: 2 anomalies; VACTERL: 3 anomalies Currarino triad: anorectal malformation, sacral bony abnormality, presacral mass OEIS:Omphalocele, Exstrophy of the bladder, Imperforate anus, Spinal defects

7
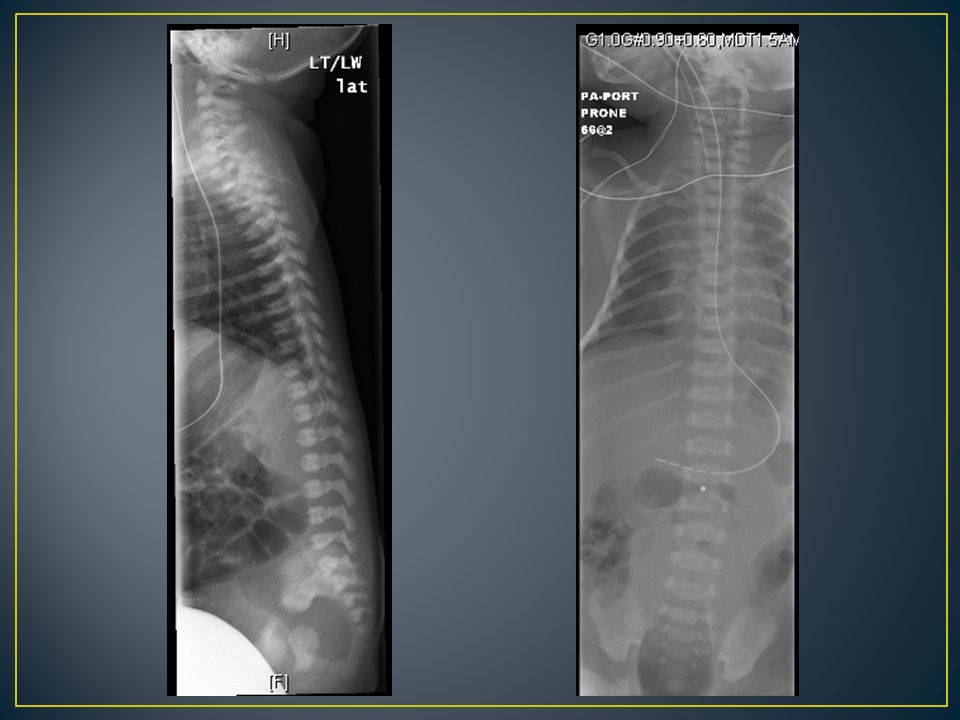
Other Investigations Renal ultrasound Echocardiogram Spinal x-rays
Essentially normal renal ultrasound save for a tiny right cortical cyst. Normal renal size. No collecting system dilatation. Echocardiogram Patent ductus arteriosus, left to right shunt, trivial. Small secundum atrial septal defect measuring 4 mm with left to right flow. Spinal x-rays 6 lumbar-type vertebrae. Sacral ultrasound The conus terminates normally at the level of L2/3. The conus and cauda equina layer dependently, without evidence of tethering or thickening of the filum. There is no intraspinous mass. There is no meningocele.

9
Tethered Spinal Cord Syndrome
Due to traction on spinal cord Occurs with spinal dysraphism Manifestations Cutaneous: birthmark, tuft, sacral dimple (not coccygeal) Orthopedic: club feet, asymmetric leg length, scoliosis Neurologic: low back/leg pain, leg weakness Urologic: incontinence, recurrent UTIs Anorectal: incontinence, constipation Radiologic criteria Low-lying conus medullaris (below L1-2) Tight/fatty filum terminale Conus at L2-3 only in ~10% even at newborn age Thickened filum >1mm
 Orthopedic: club feet, asymmetric leg length, scoliosis. Neurologic: low back/leg pain, leg weakness. Urologic: incontinence, recurrent UTIs. Anorectal: incontinence, constipation. Radiologic criteria. Low-lying conus medullaris (below L1-2) Tight/fatty filum terminale. Conus at L2-3 only in ~10% even at newborn age. Thickened filum >1mm.")
10
Tsakayannis and Shamberger, 1995
Prospective study of 45 infants with imperforate anus 6 infants (14%) found to have tethered cord No correlation with type of lesion No correlation with bony sacral abnormalities All participants had either US or MR 10 infants had both No indication of how/why imaging modality chosen Conclusion: screen all infants with imperforate anus to allow for early surgical correction of TSC
 found to have tethered cord. No correlation with type of lesion. No correlation with bony sacral abnormalities. All participants had either US or MR. 10 infants had both. No indication of how/why imaging modality chosen. Conclusion: screen all infants with imperforate anus to allow for early surgical correction of TSC.")
11
Levitt et al, 1997 Review of 934 cases of anorectal malformation
111 patients underwent spinal MRI 27 (24%) had evidence of TSC Increasing prevalence with increasing severity of malformation Not statistically significant 18 underwent surgical release 6 were asymptomatic None had significant improvement in bowel/urinary function Patients with TSC more likely to have incontinence Not able to determine causality vs coincidence Less likely to have constipation May be related to severity of anorectal malformation
 had evidence of TSC. Increasing prevalence with increasing severity of malformation. Not statistically significant. 18 underwent surgical release. 6 were asymptomatic. None had significant improvement in bowel/urinary function. Patients with TSC more likely to have incontinence. Not able to determine causality vs coincidence. Less likely to have constipation. May be related to severity of anorectal malformation.")
12
Indications for Screening
Mandatory Recommended Myelodysplasia Recto-bladder neck fistula Lateral sacral ratio <0.6 Cloaca common channel >3cm AP sacral ratio <0.4 Presacral mass Complex defect Sacral hemivertebra Cloacal exstrophy Single kidney Ectopic kidney Hypospadias Spinal hemivertebra

13
Golonka et al, 2002 Retrospective review of 79 patients with imperforate anus 63 evaluated with spinal MRI 22 had TSC 11 of 41 (26.8%) with high lesions 11 of 22 (50%) with low lesions No specific predictors All confirmed upon surgical release Conclusion: all with anorectal malformations regardless of level of lesion should undergo MRI screening Those with TSC should undergo untethering to avoid incontinence due to neurologic deficit, as surgery only halts progression (does not reverse symptoms)
 with high lesions. 11 of 22 (50%) with low lesions. No specific predictors. All confirmed upon surgical release. Conclusion: all with anorectal malformations regardless of level of lesion should undergo MRI screening. Those with TSC should undergo untethering to avoid incontinence due to neurologic deficit, as surgery only halts progression (does not reverse symptoms)")
14
O’Neill et al, 2010 Hospital policy that all neonates with VACTERL, TEF, or imperforate anus screened with echo, renal US, spinal US Abnormal spinal US followed by MRI Retrospective analysis of 112 cases 36 met criteria for VACTERL 13 (39%) had TSC All had vertebral anomaly More likely to have anal atresia 38 had non-VACTERL anal atresia 3 (7.9%) had TSC 3 of 14 (21.4%) MRI-confirmed TSC had false-negative US Conclusion: screening spinal MRI for all children with VACTERL
 had TSC. All had vertebral anomaly. More likely to have anal atresia. 38 had non-VACTERL anal atresia. 3 (7.9%) had TSC. 3 of 14 (21.4%) MRI-confirmed TSC had false-negative US. Conclusion: screening spinal MRI for all children with VACTERL.")
15
Literature Take Home Points
Anorectal malformations and spinal dysraphisms are associated, but exact relationship not established Spinal imaging in infants with imperforate anus to screen for both VACTERL and TSC Stooling issues in those with imperforate anus – difficult to determine anorectal vs neurologic causality MRI is best imaging modality for occult spinal dysraphisms

16
Considerations with BS
Conus level Supernumerary lumbar vertebra Limitation of US as screening tool Indications for surgical untethering Potential prevention of neurological progression

17
My Conclusions Given the finding of 6 lumbar vertebra and the limitations of US, I would have gotten a spinal MRI If TSC found, would recommend untethering by 6mo Institution-based (no consensus) Low morbidity, great potential benefit
 Low morbidity, great potential benefit.")
18
References Tsakayannis DE, Shamberger RC. Association of imperforate anus with occult spinal dysraphism. J Pediatr Surg Jul;30(7): Long FR, Hunter JV, Mahboubi S, Kalmus A, Templeton JM Jr. Tethered cord and associated vertebral anomalies in children and infants with imperforate anus: evaluation with MR imaging and plain radiography. Radiology Aug;200(2): Melhem ER. Tethered cord and associated anomalies in children and infants with imperforate anus: evaluation with MR imaging and plain radiography. Radiology Aug;200(2):318-9. Levitt MA, Patel M, Rodriguez G, Gaylin DS, Pena A. The tethered spinal cord in patients with anorectal malformations. J Pediatr Surg Mar;32(3):462-8. Golonka NR, Haga LJ, Keating RP, Eichelberger MR, Gilbert JC, Hartman GE, Powell DM, Vezina G, Newman KD. Routine MRI evaluation of low imperforate anus reveals unexpected high incidence of tethered spinal cord. J Pediatr Surg Jul;37(7):966-9. O'Neill BR, Yu AK, Tyler-Kabara EC. Prevalence of tethered spinal cord in infants with VACTERL. J Neurosurg Pediatr Aug;6(2): “Spinal dysraphisms.” In: Principles of Neurological Surgery. “Pediatric abdomen.” In: Greenfield’s Textbook of Surgery. “Tethered cord syndrome.” In: Greenberg;s Manual of Neurosurgery.
: Melhem ER. Tethered cord and associated anomalies in children and infants with imperforate anus: evaluation with MR imaging and plain radiography. Radiology Aug;200(2): Levitt MA, Patel M, Rodriguez G, Gaylin DS, Pena A. The tethered spinal cord in patients with anorectal malformations. J Pediatr Surg Mar;32(3): Golonka NR, Haga LJ, Keating RP, Eichelberger MR, Gilbert JC, Hartman GE, Powell DM, Vezina G, Newman KD. Routine MRI evaluation of low imperforate anus reveals unexpected high incidence of tethered spinal cord. J Pediatr Surg Jul;37(7): O Neill BR, Yu AK, Tyler-Kabara EC. Prevalence of tethered spinal cord in infants with VACTERL. J Neurosurg Pediatr Aug;6(2): Spinal dysraphisms. In: Principles of Neurological Surgery. Pediatric abdomen. In: Greenfield’s Textbook of Surgery. Tethered cord syndrome. In: Greenberg;s Manual of Neurosurgery.")
Similar presentations

















 are variable, occur in 1 of 500 newborns; predisposing to development of hypertension,>")

