Download presentation
Presentation is loading. Please wait.

1
Acute Appendicitis: What I didn’t know before Jennifer Newberger, MD General Surgery R3 May 19, 2011

2
Overview Case presentation History Epidemiology Pathophysiology Clinical manifestations and diagnosis Literature review to answer my questions

3
Case Presentation RD is a 2y/o M who presented to OSH with 4 day h/o emesis, 3 day h/o abdominal pain, and 2 day h/o fever and diarrhea WBC 12 with left shift U/S confirmed acute appendicitis I was called to examine the pt urgently, as the ER was waiting to administer morphine until I examined him He was lethargic, cried with palpation, diffusely tender with involuntary guarding He underwent laparoscopic appendectomy and was found to be perforated at the appendiceal base

4
Postoperative Course He was kept NPO with an NGT to LIS He was started on zosyn POD#5 his WBC elevated at 22, cont on zosyn By POD#7 he had no sign of return of bowel function, continued to be intermittently febrile and complained of significant abdominal pain He underwent CT scan that revealed a pelvic abscess POD#8 he underwent CT guided drainage

5
Questions Did he really need the u/s Did they really need to wait to give him morphine Should we done an open appendectomy Do patients with perforated appendicitis do better on multiple abx How long should patients with perforated appendicitis get IV abx Why did we wait until POD#7 to get the CT scan

6
History Leonardo da Vinci first depicted appendix in drawings in 1492 Berengario Da Carpi is credited for the first description in 1521 Lorenz Heister MD first to recognize the appendix as site for acute primary inflammation in 1711 In 1735 Claudius Amyand incision and drained a scrotal abscess, identified, tied off and removed a perforated appendix through scrotal incision

7
History continued In 1827 Francois Melier described the characteristic signs and symptoms of appendicitis In 1839 Bright and Addison provided first textbook description of acute appendicitis Successful appendectomies performed in 1880 by Lawson Tait in Britain and 1883 by Canadian Abraham Groves. First successful appendectomy in US by Thomas G Morton in 1887

8
History continued In 1886 Reginald Fitz presented “Perforative Inflammation of the Vermiform Appendix with Special Reference to Early Diagnosis and Treatment” to the Association of American Physicians 1889 Charles McBurney published his first paper on appendicitis describing the most likely location to be 1.5-2 inchest toward the umbilicus from the superior iliac crest

9
Epidemiology Most common acute surgical condition in children Mean age at presentation is 11-12yrs Lifetime risk 7% Fewer than 5% patients are under 5 yrs Males outnumber females by 55-65% Risk of perforation 30-45% >5yrs, 60% < 5yrs and 95% <2yrs

10
Pathophysiology Luminal obstruction of appendix most commonly from fecalith or lymphoid hyperplasia The mucosa continues to secrete mucus causing increased intraluminal pressure Venous drainage is impaired The wall becomes edematous and mucosal ischemia ensues Bacterial invasion of the wall -> acute appendicitis, gangrene and eventually perforation

11
Clinical Manifestation Textbook presentation – periumbilical pain migrating to RLQ, emesis, diarrhea, annorexia, fever PE findings include RLQ pain, rebound guarding, rovsing sign, psoas sign, obturator sign Neonates – abdominal distension, emesis, irritability - PE distention, mass, cellulitis, hypothermia, hypotension Infants (<2yrs) – emesis, fever, diarrhea, irritability, pain - PE diffusely TTP, guarding, <50% have RLQ pain Preshool (2-5yrs) – emesis followed by pain, fever and annorexia - PE RLQ pain, guarding
 – emesis, fever, diarrhea, irritability, pain - PE diffusely TTP, guarding, <50% have RLQ pain Preshool (2-5yrs) – emesis followed by pain, fever and annorexia - PE RLQ pain, guarding")
12
Diagnosis History and physical CBC UA Imaging?

13
Pediatric Appendicitis Score (PAS) Low risk < 2 1-2.4% chance of appendicitis High risk > 7 78-96% chance of appendicitis ItemPoints Annorexia1 Nausea and emesis1 Migration of pain1 Fever > 381 Pain with cough, percussion or hopping2 RLQ pain2 WBC > 10,0001 Neutrophils plus band forms > 75001 Total10
 Low risk < 2 1-2.4% chance of appendicitis High risk > 7 78-96% chance of appendicitis ItemPoints Annorexia1 Nausea and emesis1 Migration of pain1 Fever > 381 Pain with cough, percussion or hopping2 RLQ pain2 WBC > 10,0001 Neutrophils plus band forms > Total10")
14
Analgesia? 5-16 yrs, admitted to ER with acute abdominal pain Randomized to either morphine (52) or normal saline (56) Primary endpoints were difference in pain, the diagnosis of appendicitis and laparotomy after observation No difference in diagnosis of appendicitis and no difference in rate of laparotomy after observation Significantly better pain controlled in morphine group
 or normal saline (56) Primary endpoints were difference in pain, the diagnosis of appendicitis and laparotomy after observation No difference in diagnosis of appendicitis and no difference in rate of laparotomy after observation Significantly better pain controlled in morphine group.")
15
Analgesia? 8-18yrs, admitted to ED with RLQ pain Randomized to morphine (45) or placebo (42) Primary outcomes were difference in pain and time from arrival in ED to surgical decision No significant difference in pain or in time to surgical decision
 or placebo (42) Primary outcomes were difference in pain and time from arrival in ED to surgical decision No significant difference in pain or in time to surgical decision.")
16
Imaging? Reviewed children undergoing appendectomy from 1997 to 2001 Diagnostic workup (CT, US, or no imaging) was recorded as were the final pathology results. 616 appendectomies performed. Mean age was 10.4 +/- 4.1 years, and 60% were boys. 184 children (30%) underwent CT 104 (17%) had US 310 (50%) had no imaging
 was recorded as were the final pathology results. 616 appendectomies performed. Mean age was /- 4.1 years, and 60% were boys. 184 children (30%) underwent CT 104 (17%) had US 310 (50%) had no imaging.")
17
Imaging A pathologically normal appendix was removed in 7% of CT patients, 11% of US patients, and 8% of patients without a study. CT scanning increased from 1.3% of all children in 1997 to 58% in 2001 US decreased from 40% to 7% Over the same period, the overall negative appendectomy rate did not change significantly from 8% to 7%. Increased CT scanning has not changed negative appendectomy rate H&P by an experienced surgeon is as accurate as both US and CT in diagnosing acute appendicitis

18
Imaging Ultrasound has advantage of being inexpensive and safe, disadvantage of being dependent on skills CT has advantage of being readily available and not operator dependent, disadvantage of radiation exposure Meta-analysis of 26 studies that evaluated the diagnostic performance of US and CT

19
Imaging US pooled sensitivities and specificities were 88% (95% CI 86-90) and 94% (95% CI 92-95), respectively Inaccurate exams were significantly associated with high BMI (>85 th percentile) CT pooled sensitivities and specificities were 94% (95% CI 92-97) and 95% (95% CI 94-97), respectively
 and 94% (95% CI 92-95), respectively Inaccurate exams were significantly associated with high BMI (>85 th percentile) CT pooled sensitivities and specificities were 94% (95% CI 92-97) and 95% (95% CI 94-97), respectively")
20
Laparoscopic versus open Comparison of outcomes after laparoscopic (LA) versus open appendectomy (OA) for acute appendictis at 222 ACS NSQIP hospitals Patients identified who underwent appendectomy from 2005 to 2008 Association between surgical approach and risk-adjusted overall morbidity, SSI, serious morbidity/mortality Individual complications in patients with acute appendicitis and complicated appendicitis Relationships between operative approach, operative duration, and extended duration of stay with hospital academic affiliation 32,683 patients - 24,969 (76.4%) underwent LA and 7,714 (23.6%) underwent OA
 versus open appendectomy (OA) for acute appendictis at 222 ACS NSQIP hospitals Patients identified who underwent appendectomy from 2005 to 2008 Association between surgical approach and risk-adjusted overall morbidity, SSI, serious morbidity/mortality Individual complications in patients with acute appendicitis and complicated appendicitis Relationships between operative approach, operative duration, and extended duration of stay with hospital academic affiliation 32,683 patients - 24,969 (76.4%) underwent LA and 7,714 (23.6%) underwent OA")
21
Laparoscopic versus open Patients who underwent OA were significantly older with more comorbidities LA less likely to experience an overall morbidity (4.5% vs 8.8%; OR 0.60 [0.54-0.68] LA less likely to have SSI (3.3% vs 6.7%; OR 0.57 [0.50-0.65] No significant difference in serious morbidity/mortality LA less likely to develop individual infectious complications except for organ space SSI – pts with complicated appendicitis, organ space SSI was significantly more common after LA (6.3% vs 4.8%; OR 1.35 [1.05-1.73] For all patients with acute appendicitis, those treated at academic- affiliated versus community hospitals were equally likely to undergo LA versus OA Operative duration at academic centers was significantly longer for both LA and OA
![Laparoscopic versus open Patients who underwent OA were significantly older with more comorbidities LA less likely to experience an overall morbidity (4.5% vs 8.8%; OR 0.60 [ ] LA less likely to have SSI (3.3% vs 6.7%; OR 0.57 [ ] No significant difference in serious morbidity/mortality LA less likely to develop individual infectious complications except for organ space SSI – pts with complicated appendicitis, organ space SSI was significantly more common after LA (6.3% vs 4.8%; OR 1.35 [ ] For all patients with acute appendicitis, those treated at academic- affiliated versus community hospitals were equally likely to undergo LA versus OA Operative duration at academic centers was significantly longer for both LA and OA](http://images.slideplayer.com/35/10313356/slides/slide_21.jpg "Laparoscopic versus open Patients who underwent OA were significantly older with more comorbidities LA less likely to experience an overall morbidity (4.5% vs 8.8%; OR 0.60 [ ] LA less likely to have SSI (3.3% vs 6.7%; OR 0.57 [ ] No significant difference in serious morbidity/mortality LA less likely to develop individual infectious complications except for organ space SSI – pts with complicated appendicitis, organ space SSI was significantly more common after LA (6.3% vs 4.8%; OR 1.35 [ ] For all patients with acute appendicitis, those treated at academic- affiliated versus community hospitals were equally likely to undergo LA versus OA Operative duration at academic centers was significantly longer for both LA and OA")
22
Laparoscopy in Complicated Appendicitis Several retrospective studies, 1 RCT A total of 102 children with suspected acute appendicitis were selected randomly to undergo either a laparoscopic or an open appendectomy The outcomes of 25 children with complicated appendicitis, 13 in the laparoscopic group and 12 in the open appendectomy group, were analyzed Children, their parents, and research nurses were blinded to which procedure had been performed and remained blinded until the control visit 7 days after the operation All 25 children completed a 30-day follow-up

23
Laparoscopy Cont’d The mean operating time was 63 minutes in the laparoscopic group and 37 minutes in the open appendectomy group (mean difference 26 minutes, 95% CI 5 to 47 minutes, P =.02). 2 major complications in the laparoscopic – one had entero- cutaneous fistula of the residual appendiceal tip that needed open reoperation and another had a pelvic abscess that resolved with antibiotic treatment Superficial wound infections were encountered in 2 patients in the open appendectomy group, no other complications Conslusion was that laparoscopy was a good alternative to open operation

24
Postoperative Abx Single agent vs multiple agents - Retrospective review of 94 children admitted over 3 year period with perforated appendicitis - Demographic data, duration of presenting symptoms, initial WBC, length of stay, and infectious complications were abstracted - 51 pts in zosyn group, 43 pts in multidrug group - No significant difference in complications - Significantly higher cost in multidrug group

25
Postoperative Abx Evidence regarding the optimum duration of antibiotic therapy is limited A systematic review of postoperative antibiotic duration for children Twenty-eight studies were selected that included 2,284 patients No consistency among the protocols regarding length of antibiotic use, discharge criteria, or use of home antibiotics following discharge.

26
Postoperative Abx A survey sent to all practicing pediatric surgeons in North America in April 2000 who were members of the American Pediatric Surgical Association for 1999-2000. Survey questions pertained to preoperative, perioperative, and postoperative practice patterns, particularly those issues related to use of antibiotic therapy 80.2% completed the survey Only 17% of surgeons used a formal clinical practice guideline to direct care. Responses varied substantially in the duration of postoperative antibiotic therapy, the use of intravenous or oral agents or both, and the duration of hospitalization. There is little apparent consensus

27
Antibiotics? RCT with pts >18y/o with suspected acute appy. Primary outcome: Major and minor complications. Secondary outcome: LOS and readmission rates. 3 RCT included, total 661 patients. Diagnosis based on H&P with positive labs. Some patients US/CT.

28
Antibiotics? Abx group: 350 pts. 238 (65%) successful therapy, with 38 (15%) recurrences. 112 patients crossed over to surgery group. Surgery group: 394 pts. 357 successful therapy (histologically confirmed appendicitis) Conclusion: Abx therapy is safe to use in non- complicated acute appy. Associated with 68% success rate and trend toward less complications - Appendectomy remains the gold standard
 Conclusion: Abx therapy is safe to use in non- complicated acute appy. Associated with 68% success rate and trend toward less complications - Appendectomy remains the gold standard.")
29
Postoperative CT scan Retrospective review of all CT scans obtained for suspicion of abscess 3-30 days after abdominal or pelvic operation from Jan 2000 to Dec 2002 at single institution. Divided into early (3-7 days) and late (>7 days) Examined type of operation, interval from operation to CT, CT results and subsequent treatment 262 CT scans performed for suspected abscess, 106 early and 156 late 4500 abdominal or pelvic operations - ~5% had CT for suspected abscess
 and late (>7 days) Examined type of operation, interval from operation to CT, CT results and subsequent treatment 262 CT scans performed for suspected abscess, 106 early and 156 late 4500 abdominal or pelvic operations - ~5% had CT for suspected abscess.")
30
Postoperative CT ProcedureNo. Appendectomy51 (22%) Colorectal50 (22%) Hysterectomy/Gynecological27 (12%) Small bowel LOA21 (9%) Gastric/esophageal17 (7%) Cesarean section14 (6%) Gallbladder/biliary tract14 (6%) Genitourinary9 (4%) Pancreatic8 (4%) Hernia5 (2%) Other11 (5%)
 Colorectal50 (22%) Hysterectomy/Gynecological27 (12%) Small bowel LOA21 (9%) Gastric/esophageal17 (7%) Cesarean section14 (6%) Gallbladder/biliary tract14 (6%) Genitourinary9 (4%) Pancreatic8 (4%) Hernia5 (2%) Other11 (5%).")
31
Postoperative CT scan

32
Postoperative CT Most common time for CT was POD#7 No significant difference in diagnosis of abscess or abscess drainage between groups In 26 patients CT was repeated for suspected abscess after initial CT negative - 15 remained negative, of the other 11, 6 had there initial CT after 7 days Conclusion – Contrary to historical dogma, CT scan for intraabdominal abscess early in postoperative period can be diagnostic

33
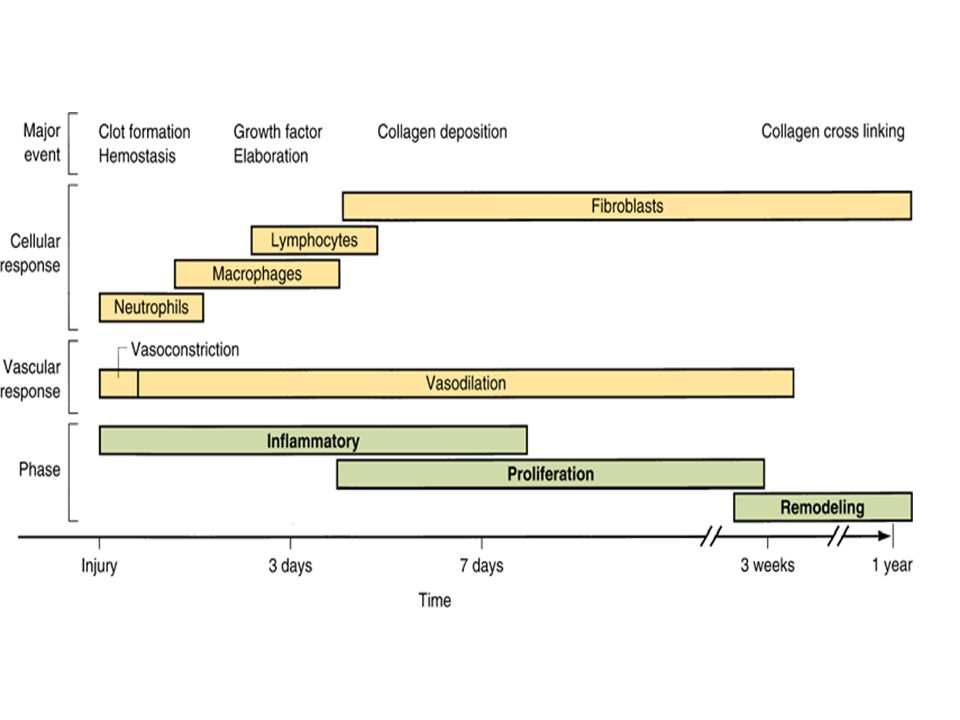
Abscess formation Abdominal cavity lined by the peritoneum that consists of a single layer of mesothelial cells, supported by a basement membrane and an underlying sheet of connective tissue. Peritoneal trauma results in mesothelial damage and is accompanied by inflammation. Production and release of a broad spectrum of biologically active proteins and exudation of protein-rich fluid that contains large amounts of fibrinogen The coagulation cascade is activated resulting in the formation of thrombin that triggers conversion of fibrinogen into fibrin Fibrin forms deposits that are a matrix for the ingrowth of fibrocollagenous tissue capsule Fibrin clots protect bacteria against the immunological defenses of the abdominal cavity.

35
Summary Perforated appendicitis can be challenging to manage Dr. Ricca is wrong

Similar presentations