Download presentation
Presentation is loading. Please wait.

2
F.Sharifipour,Nephrologist Associate professor, Mashhad university of medical sciences.

3
Aging is characterized by progressive and broadly predictable changes that are associated with increased susceptibility to many diseases. Aging is not a homogenous process. Rather, organs in the same person age at different rates influenced by multiple factors, including genetic make-up, lifestyle choices, and environmental exposures.

4
In 1999, glomerular filtration rate (GFR)-estimating equations started to replace serum creatinine for the evaluation of kidney function. Since that time, more and more older adults have been identified as having acute or chronic kidney disease (CKD), and the prevalence of diagnosed kidney disease in this population has increased.
, and the prevalence of diagnosed kidney disease in this population has increased..")
5
About half of adults over the age of 70 years now have a measured or estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m 2, a threshold often used to diagnose CKD. Higher prevalence of diagnosed CKD is not simply due to increased recognition of diseases that tend to cluster in older adults rather it results from the normal structural and functional changes that occur in the kidney with aging.

6
The aging kidneyThe aging kidney The kidney systematically loses function (ie, GFR) with age. In addition to specific kidney diseases that are common in older adults, such as diabetic nephropathy, physiological senescence of the kidney occurs, even with healthy aging.

7
Physiologic senescence Aging as a risk factor of kidney disease Common kidney disease in elderly

8
Structural changes Functional changes

9
Micro-anatomical changes :The major micro-anatomical changes that occur with aging are nephrosclerosis and nephron hypertrophy. The total number of sclerosed and non-sclerosed glomeruli declines with age Macro-anatomical changes : The major macro- anatomical changes that occur with aging include a reduction in cortical volume and the appearance of renal cysts and tumors.

10
The aging kidney: Macroanatamical changes Kidney parenchymal volume is stable before age 50 years but declined after age 50 years. Renal mass decreases by 25 to 30 percent between the ages of 30 and 80 years, with the steepest decline after age 50. Cortical volume declined throughout the adult age spectrum in both men and women, but with an accelerated rate of decline after age 50 years. The age-related decline in kidney cortical volume is largely due to underlying nephrosclerosis Medullary volume increased with age in both men and women until age 50 years, after which it declined in women and remained static in men. Renal sinus fat increases with age; this could have masked some of the decline in kidney parenchymal volume with aging.

11
Renal parenchymal cysts become more common, more numerous, and larger with aging. Age-related diverticula in renal tubules are the precursor lesion to these renal cysts. So the diagnosis of autosomal dominant polycystic kidney disease (ADPKD) with renal ultrasound imaging requires age-specific criteria in elderly. Other renal cysts are also more common with aging, including parapelvic renal cysts (due to lymphatic dilation near the renal sinus), angiomyolipomas, and malignant cysts or tumors.
 with renal ultrasound imaging requires age-specific criteria in elderly. Other renal cysts are also more common with aging, including parapelvic renal cysts (due to lymphatic dilation near the renal sinus), angiomyolipomas, and malignant cysts or tumors..")
12
Other structural changes : Atherosclerosis of renal arteries (with or without significant stenosis) is more prevalent in older individuals. parenchymal calcifications and cortical scars BPH in men Urethral anatomical changes in women

13
Glomerular filtration rate (GFR) is the primary tool for assessing age-related functional changes in the kidney. Glomerular filtration rate (GFR) is the primary tool for assessing age-related functional changes in the kidney. Rates of GFR decline with aging follow a fairly normal distribution, suggesting that it is primarily driven by a physiological process. Rates of GFR decline with aging follow a fairly normal distribution, suggesting that it is primarily driven by a physiological process. GFR (measured by inulin clearance) declined by 10 mL/min per decade of life GFR (measured by inulin clearance) declined by 10 mL/min per decade of life
 is the primary tool for assessing age-related functional changes in the kidney. Rates of GFR decline with aging follow a fairly normal distribution, suggesting that it is primarily driven by a physiological process. Rates of GFR decline with aging follow a fairly normal distribution, suggesting that it is primarily driven by a physiological process. GFR (measured by inulin clearance) declined by 10 mL/min per decade of life GFR (measured by inulin clearance) declined by 10 mL/min per decade of life.")
14
The age-related decline in GFR that is not detected by serum creatinine alone. The age-related decline in muscle mass, causes serum creatinine remains stable with healthy aging. GFR is usually estimated from serum creatinine (eGFR creatinine ) using the Modification of Diet in Renal Disease (MDRD) or Cockcroft-Gault equation. The Cockcroft-Gault equation : (140 - age) x lean body weight [kg] ClCr (mL/min) = ——————————————————— Cr [mg/dL] x 72
 using the Modification of Diet in Renal Disease (MDRD) or Cockcroft-Gault equation. The Cockcroft-Gault equation : (140 - age) x lean body weight [kg] ClCr (mL/min) = ——————————————————— Cr [mg/dL] x 72.")
15
GFR, in mL/min per 1.73 m 2 = 186 x( Serum Cr level) -1.154 x Age - 0.203 x (0.742 if female) x (1.21 if black) Websites are also available to aid in the calculation of the GFR through these formulas. These include: www.kidney.org/professionals/KLS/gfr_calculator.cfm nephron.com/mdrd/default.html

16
The aging kidney clinical significance There are no proven therapies to halt or reverse age- related declines in glomerular filtration rate (GFR There are no proven therapies to halt or reverse age- related declines in glomerular filtration rate (GFR). Any therapy aimed at raising the GFR by causing the remaining functional nephrons to filter more may actually be harmful rather than beneficial to the kidney. This is a key difference distinguishing age-related "chronic kidney disease (CKD)" from other age-related chronic disease such as hypertension or hyperlipidemia. Age-related hypertension and hyperlipidemia can be reversed, and reducing the blood pressure and cholesterol has clinical benefit in older adult patients.
 from other age-related chronic disease such as hypertension or hyperlipidemia. Age-related hypertension and hyperlipidemia can be reversed, and reducing the blood pressure and cholesterol has clinical benefit in older adult patients..")
17
medication dose adjustments. Patients with age-related reductions in GFR require medication dose adjustments. at higher risk for acute kidney injury. The loss of functioning nephrons associated with normal aging puts older adults at higher risk for acute kidney injury. The typical age-related declines in GFR have little, if any, effect on life expectancy, and this point is important in discussions with older adult patients. Age-related declines in GFR do not typically prevent older adults from becoming living kidney donors.

18
The kidneys of older patients demonstrate impaired renal conservation of sodium in response to an acute reduction of sodium intake, as well as impaired ability to rapidly excrete a large sodium load. The reduced diluting capacity of the kidney increases the risk of hyponatremia in older patients, particularly those with a low-protein and also contributes to thiazide-associated hyponatremia, which is more common in older adults.

19
Acute kidney injury is greater with aging. It is 3.5 times more prevalent in patients older than 70 years with increased mortality and morbidity in hospitalized patients. In 28% of patients older than 65 years recovery of renal function after AKI is less. Prerenal azotemia accounts for 50% of AKI in the elderly due to : dehydration (vomiting, diarrhea, bleeding, diuretics), impaired sodium conservation and thirst, drugs such as ACEIs, ARBs, NSAIDs. Prerenal AKI is usually reversible,however evolution to ATN is more common in older than in younger patients.(23% vs. 15%)
, impaired sodium conservation and thirst, drugs such as ACEIs, ARBs, NSAIDs. Prerenal AKI is usually reversible,however evolution to ATN is more common in older than in younger patients.(23% vs. 15%).")
20
Intrinsic AKI : In hospitalized patients surgical complication(hypotension, fluid loss, dysrhythmias and MI,NSAIDs), septic complication( gram negative endotoxemia, hemodynamic instability, use of nephrotoxic drugs) account for two third of AKI. Radiocontrast agents can result in ATN. Atheroemboli to the kidney due to intra-arterial cannulation (radiologic or surgical intervention),using anticoagulant or fibrinolytic and spontaneous atheroemboli in high risk patients,causes progressive and irreversible AKI. Drugs: Antibiotics such as penicillins, B-lactams and sulfonamides(TIN), NSAIDs, ACEI, ARBs(prerenal,ATN,TIN and nephrotic syndrome)
,using anticoagulant or fibrinolytic and spontaneous atheroemboli in high risk patients,causes progressive and irreversible AKI. Drugs: Antibiotics such as penicillins, B-lactams and sulfonamides(TIN), NSAIDs, ACEI, ARBs(prerenal,ATN,TIN and nephrotic syndrome).")
21
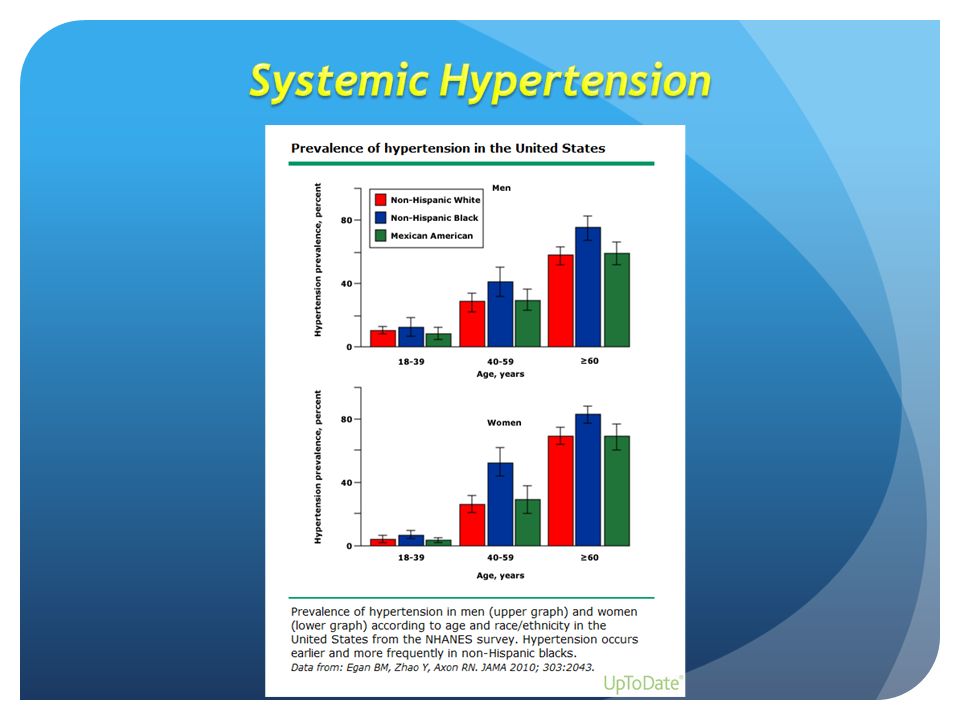
The number of patients with hypertension is likely to grow as the population ages since either isolated systolic hypertension or combined systolic and diastolic hypertension occurs in the majority of persons older than 65 years. Isolated systolic hypertension (ISH) with systolic BP>160 and diastolic BP<90mmHg is evident in nearly 75% of hypertensive elderly. ISH is a strong independent predictor risk factor for CKD in older individuals.
 with systolic BP>160 and diastolic BP<90mmHg is evident in nearly 75% of hypertensive elderly. ISH is a strong independent predictor risk factor for CKD in older individuals..")
23
Measurement of BP should be taken in standard position Periodically standing BP to screen the risk of postural hypotension should be controlled. A thorough examination to assess underlying causes and end organ involvement (including Cr to calculate GFR) is important. The goal of SBP needs to be adjusted for those with ISH and elderly patients.(150 mmHg) DBP of 60 mmHg or less in the elderly with ISH can impair tissue perfusion, increase cardiovascular risk and reduce survival.
 is important. The goal of SBP needs to be adjusted for those with ISH and elderly patients.(150 mmHg) DBP of 60 mmHg or less in the elderly with ISH can impair tissue perfusion, increase cardiovascular risk and reduce survival..")
24
Lifestyle modification remains the primary treatment with medication added as required and tailored to each patient. Various medication have been used and are tolerated in the elderly. Diuretics,CCBs, ACEIs, ARBs. The drugs should be initiated at lower dosage and titrated carefully.

25
Renovascular disease is an important cause of resistant HTN and progressive renal insufficiency in the elderly as a part of generalized atherosclerosis. Unexplained progressive azotemia, worsening or new –onset HTN, development of AKI with ACEIs or ARBs,acute pulmonary edema or unexplained heart failure should raise suspicion of renovascular disease in an elderly patient. Treatment include medical therapy with antihypertensive drugs, revascularization with angioplasty or surgery. There is no evidence that revascularization improves any outcome in asymptomatic patients.

Similar presentations



:>")













 ( National.>")

