Download presentation
Presentation is loading. Please wait.

1
Dermatological disorders First Semester 2015/2016

2
Introduction An estimated 5% of population suffer from a chronic skin, hair or nail condition Many others experience acute or seasonal disorders Many skin disorders are present at early infancy and continue to appear during childhood and adulthood Patients with skin disorders typically present with rash and/or itching which might indicate dermatitis It is essential to be able to recognize, differentiate and suggest appropriate treatment for common skin conditions, and to know when to refer patients to care providers

3
Dermatitis is a non specific term describing numerous dermatological conditions that are generally characterized with erythema Eczema and dermatitis are used interchangeably to describe a group of inflammatory disorders of unknown etiology. When the cause is known, the disorder is given a specific name Known causes include allergens, irritants, infections

4
Introduction Skin Anatomy and Function 2 anatomic layers: epidermis and dermis supported by subcutaneous fat Epidermis: most superficial, avascular, stratified squamous epithelium, SC Dermis: highly vascular, nerve endings, lymphatics, collagen protein and connective tissue. Fibroblasts and macrophages Subcutaneous tissue: adipocytes, dermal blood vessels Skin function: protection, shock absorber Skin flora, acidic pH

5
Classification of Drugs Acting on the Skin According to the layer or Disease situation

6
Atopic Dermatitis Atopy is a genetically predisposed tendency to exaggerated skin and mucosal reactivity response to environmental stimuli The Atopic triad is asthma, allergic rhinitis, atopic dermatitis. AD is a chronic, relapsing skin condition that begins during childhood and often into adulthood. The most common dermatological condition of children 30 to 80% of cases also have allergic rhinitis or asthma

7
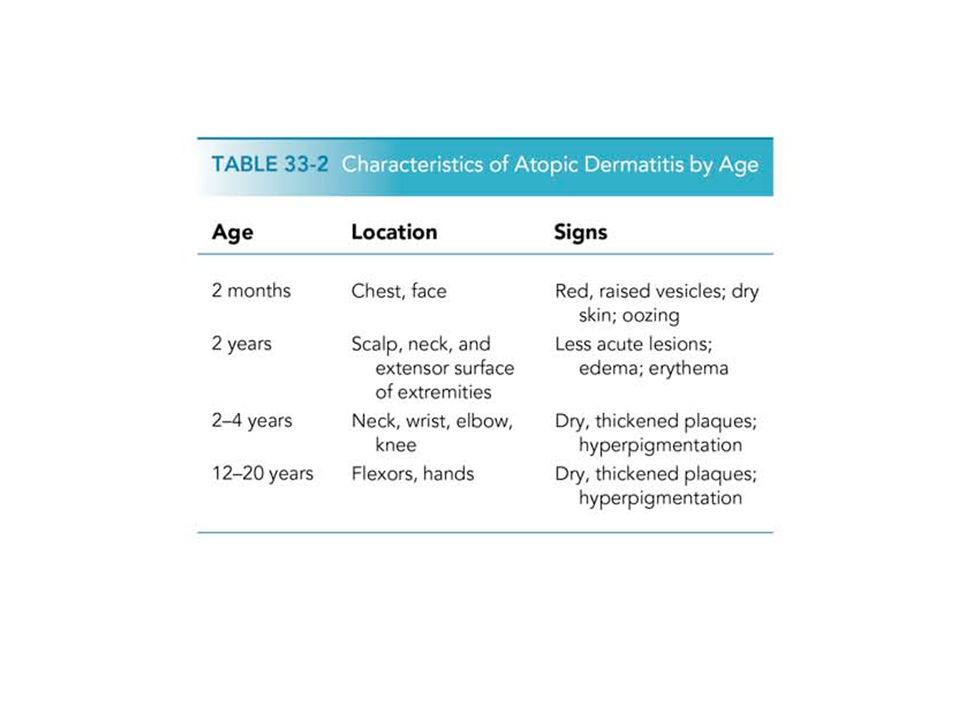
60% of case AD present in the first year of life, after 2 months of age Begin as itchy erythema of the cheeks Distribution include scalp, neck, forehead, wrist, and extensors Most cases the symptoms will disappear toward the end of the second year. The role of food allergy in infantile and childhood atopic dermatitis has been clarified Egg, peanut, milk, wheat, fish, soy, and chicken may exacerbate infantile AD

8
Pathophysiology of AD Has genetic basis: family history May be associated with allergic respiratory disease May have elevated IgE and eosinophelia Exacerbating factors include: foods, soap, detergents, fragrances, temperature and humidity changes, pollen, dust….. The role of food allergy in infantile and childhood atopic dermatitis has been clarified Egg, peanut, milk, wheat, fish, soy, and chicken may exacerbate infantile AD

9
Clinical presentation of AD Early infancy, rarely at birth Redness and chapping of infants cheeks, may continue to affect the face, neck and trunk May progress to become more generalized with crusting developed on forehead and cheeks Recurrent between 2 and 4 years of age The primary sign is intense pruritic papules and vesicles Pruritis may cause excoriation (abrasion of the epidermis by trauma)
")
11
Secondary infections, esp bacterial can be common and aggravate AD Staph aurues, or streptococci may be present Yellowish crusting of the eczematous lesions

12
TREATMENT Goals Stop the itch-scratch cycle Maintain skin hydration Avoid factors that aggravate the disorder Prevent secondary infections PATIENTS CANNOT BE CURED, SYMPTOMS CAN BE MANAGED SC in patients with AD contains less moisture than normal skin. Enhancing skin hydration can be achieved by non pharmacologic measures

14
Treatment Extensive patient education is needed Systemic long approach that includes: skin hydration, identification and elimination of flare factors, topical/systemic therapy

15
Non Pharmacologic Treatment Help patient identify irritants Bathing and moisturizing (frequency of baths, tepid water, short baths, non irritant soaps, moisturizers) Avoid occlusive clothing, moderate temperature setting, moderate humidity Treatment of topical infection (non sensitizing components) Minimize scratching
 Avoid occlusive clothing, moderate temperature setting, moderate humidity Treatment of topical infection (non sensitizing components) Minimize scratching")
16
Bath Products Bath oils Mineral or vegetable oils diluted and added to water. Lubricate the skin. Could be used as wet compresses Cleansers Should minimize dryness, glycerin soaps with high oil content, neutral pH, less drying,

17
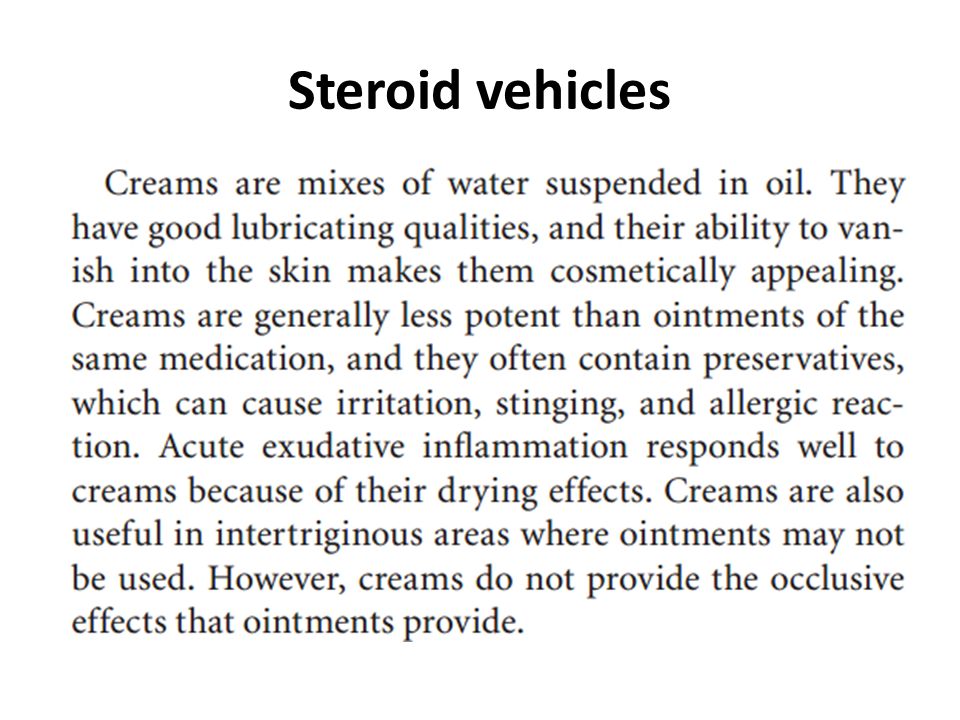
Emollients and moisturizers Generally applied 3 to 4 times daily Emollients containing petrolatum are very greasy, difficult to spread and stain. Ointments are inappropriate to oozing AD as they prevent the lesion of the crust Lactic acid Alpha hydroxy acid, used in concentrations of 2 to 5% for dry skin conditions. Acts as a modulator of epidermal karetinazation. Has good hydrating effects

18
Urea In concentrations of 10 to 30% is mild keratolytic. Increases water uptake by SC. Binds to keratin. Safe in the case of crusted tissue. Used in lotions and creams to remove the crust and in ointments to hydrate the skin

19
Pharmacologic treatment Topical Hydrocortisone The only corticosteroid that could be used as OTC for dermatitis 0.5 to 1% are considered appropriate for localized dermatitis Topical Antipruritics Topical antihistamines, local anaesthetic effect, sensitizing

22
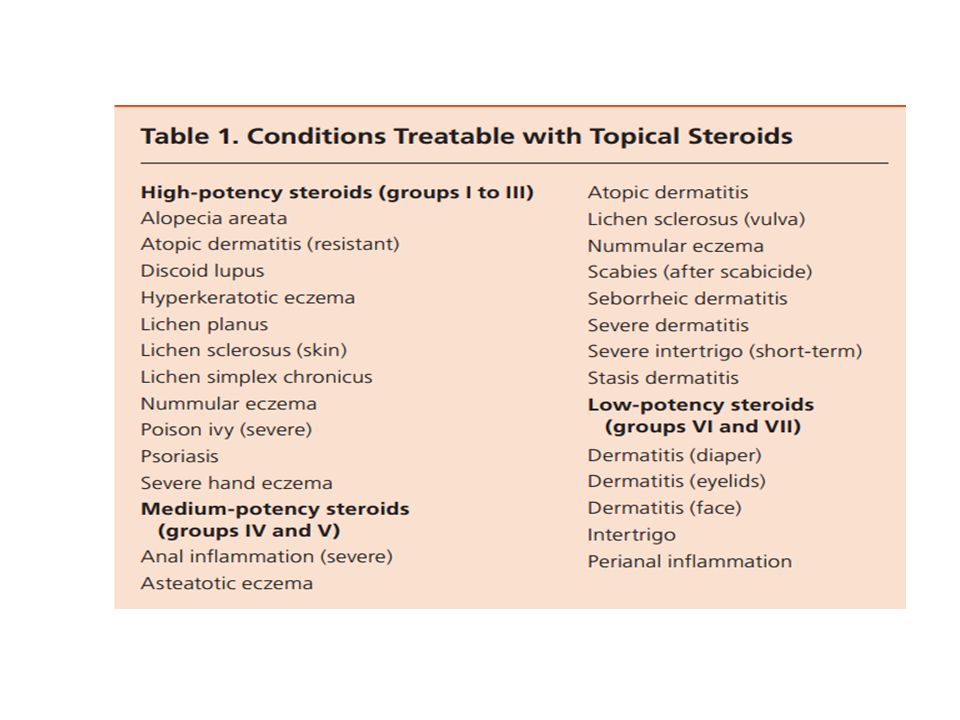
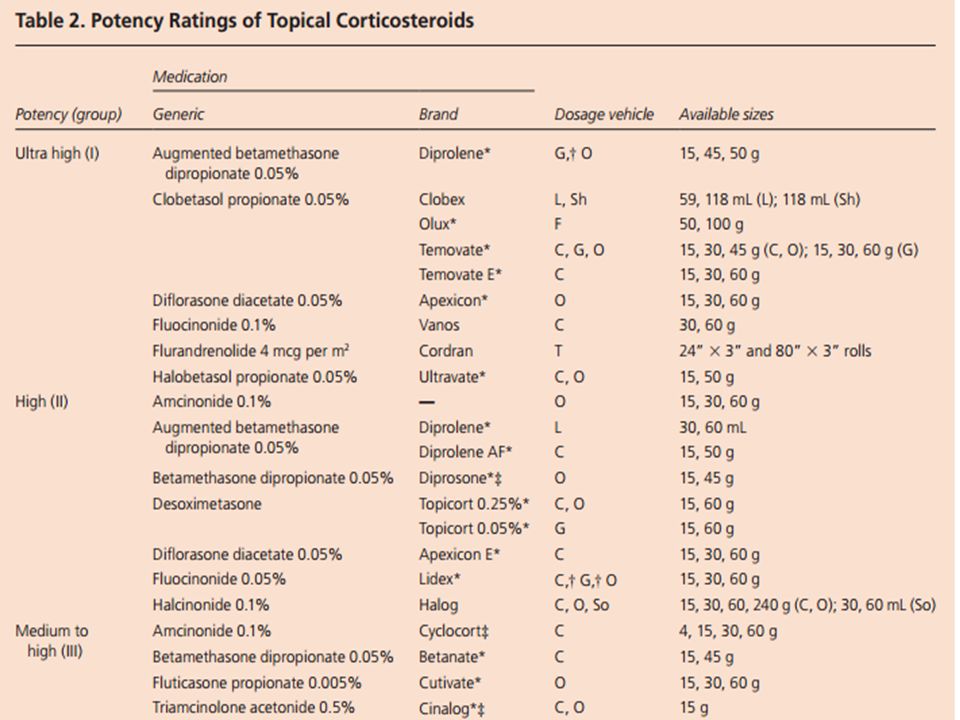
Choosing topical corticosteroids Topical corticosteroids are one of the oldest and most useful treatments for dermatologic conditions. There are many topical steroids available, and they differ in potency and formulation. Successful treatment depends on an accurate diagnosis and consideration of the steroid’s delivery vehicle, potency, frequency of application, duration of treatment, and side effects. Although use of topical steroids is common, evidence of effectiveness exists only for select conditions, such as psoriasis, eczema, atopic dermatitis, acute radiation dermatitis

24
Steroid vehicles

29
Side effects of chronic topical steroid use Rosacea Steroid atrophy Striae Talengiectasis

Similar presentations


















>")
 Prevent insensible water.>")




