Download presentation
Presentation is loading. Please wait.

1
Renal cell carcinoma R4 신재령 Clinical Practice Guidelines for the Treatment of Metastatic Renal Cell Carcinoma

2
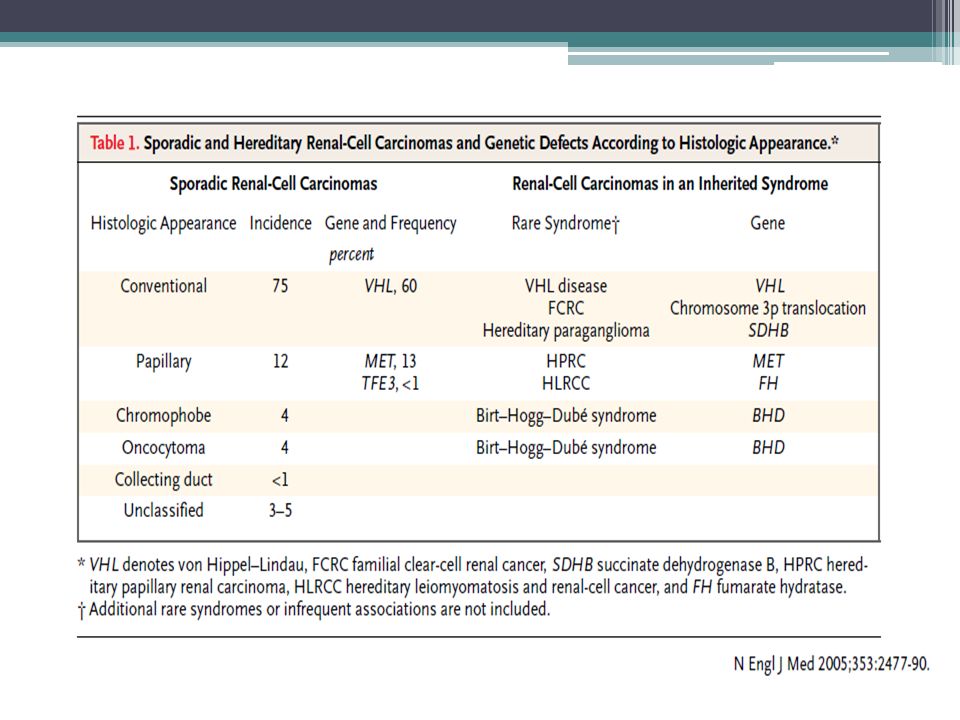
Introduction Approximately 2-3% of all malignancies Median age at diagnosis of 65 years The rate of RCC has increased by 2% per year for the past 65years 85% clear cell carcinoma, less common cell types include papillary, chromophobe and Bellini duct (collecting duct, less than 1%) tumor Smoking and obesity are among the risk factors for RCC development Several hereditary types of RCC; von Hippel-Lindau disease, caused by a mutation in the VHL gene The overall 5-year relative survival rate of patients with renal and pelvic cancers for the period between 1999-2005 from 17 SEER geographic areas was 69.4%
 tumor Smoking and obesity are among the risk factors for RCC development Several hereditary types of RCC; von Hippel-Lindau disease, caused by a mutation in the VHL gene The overall 5-year relative survival rate of patients with renal and pelvic cancers for the period between from 17 SEER geographic areas was 69.4%")
4
Initial evaluation and staging Common complaints; hematuria, flank mass and flank pain, bone pain, adenopathy, pulmonary symptoms, fever, weight loss, anemia, or a varicocele RCC in younger patients may indicate VHL disease, and these patients should be referred to a hereditary cancer clinic for further evaluation.

7
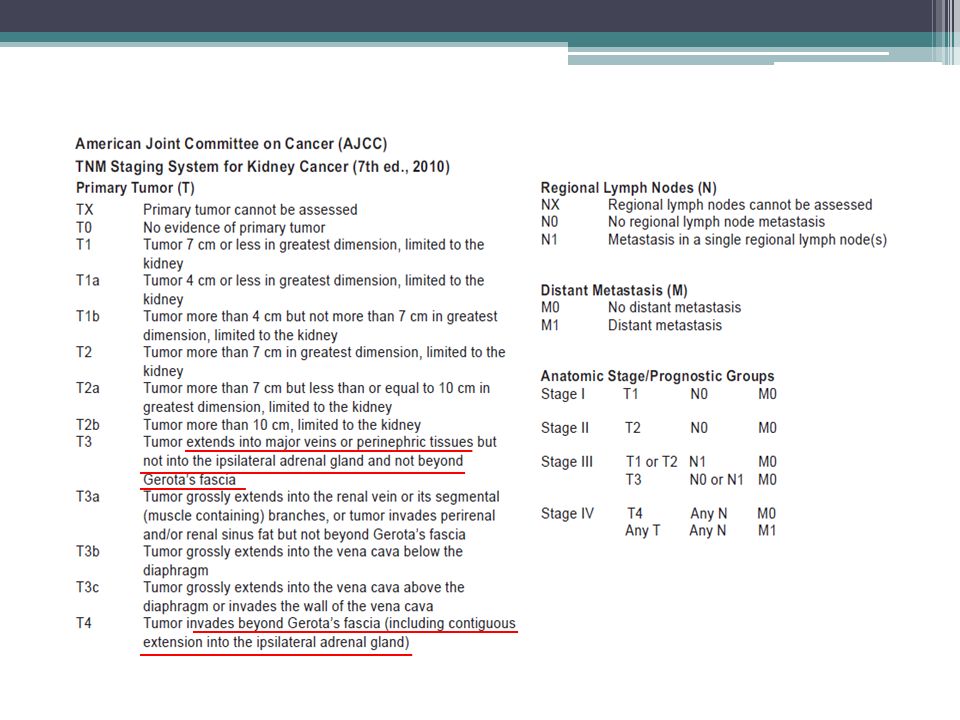
Primary treatment and staging

9
Management after surgical excision of stage I-III tumors After surgical resection, 20~30% of patients with localized tumor experience relapse ▫ Lung metastasis, 50~60% patients ▫ Median time to relapse after surgery is 1 to 2 years, with most relapses occuring within 3 years ▫ Adjuvant treatment after nephrectomy currently has no established role in patients who have undergone a complete resection of their tumor

10
Risk stratification Memorial Sloan-Kettering cancer center criteria(MSKCC) High blood LDH level >1.5 times upper limit of normal High blood calcium level (corrected ca >10mg/dL or 2.5 mmol/L) Anemia Time of less than a year from diagnosis to need for systemic treatment Low performance status (KPS < 80%) None of the above ; favorable or good risk group 1 to 2 Risk factors; intermediate group 3 or more risk factors; poor risk group
 High blood LDH level >1.5 times upper limit of normal High blood calcium level (corrected ca >10mg/dL or 2.5 mmol/L) Anemia Time of less than a year from diagnosis to need for systemic treatment Low performance status (KPS < 80%) None of the above ; favorable or good risk group 1 to 2 Risk factors; intermediate group 3 or more risk factors; poor risk group")
11
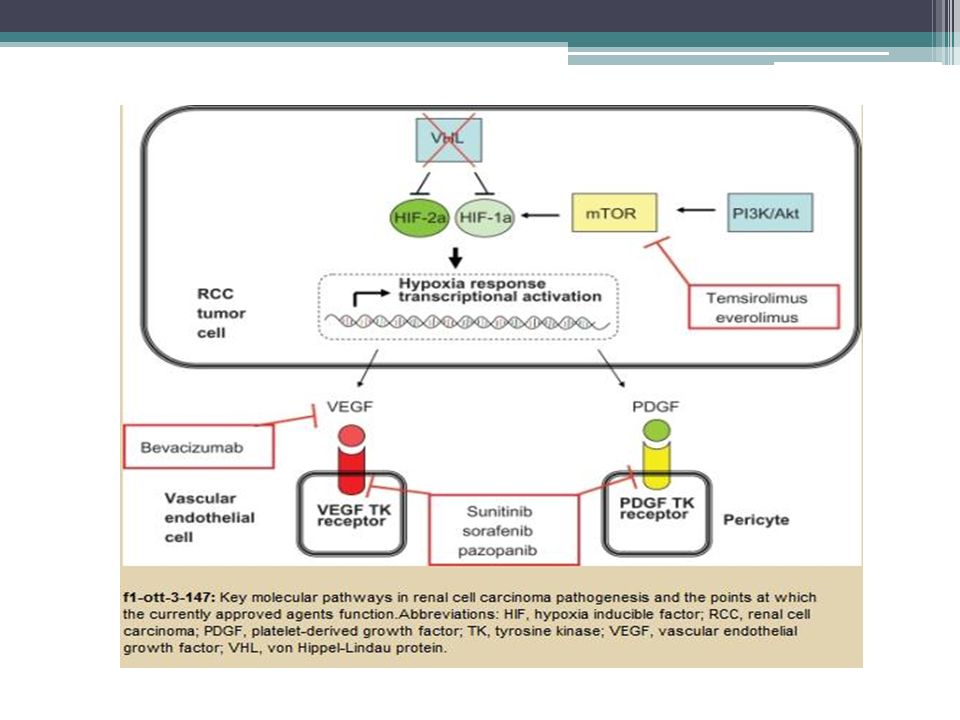
First line therapy Until recently, systemic treatment options for metastatic RCC were limited to cytokine therapy and clinical trials of novel agents Patients with a high Karnofsky perfomance status >80, low-volume or lung-predominant disease High dose IL-2 (Category2A) Recently targeted therapy utilizing tyrosine kinase inhibitors sunitinib malate, sorafenib tosylate, temsirolimus, everolimus, and recently bevacizumab in combination with interferon
 Recently targeted therapy utilizing tyrosine kinase inhibitors sunitinib malate, sorafenib tosylate, temsirolimus, everolimus, and recently bevacizumab in combination with interferon")
12
Interleukin-2 Therapy for Renal Cell Carcinoma: Treatment Option for Select Patients Potent immune stimulator, and it may have anti-angiogenic activity Since its clinical development nearly two decades ago, it remains the only therapy with a known curative potential for patients with metastatic renal carcinoma Treatment with IL-2 has substantial toxicity, priniciply secondary to capillary leak syndrome and vasodilation, which can result in serious hypotension, fluid accumulation, edema, pulmonary congestion, renal dysfunction, or other organ failure Patient selection for this form of therapy is critical. Only patients with good performance status and adequate kidney, heart, and lung function are potential candidates for IL-2 treatment

15
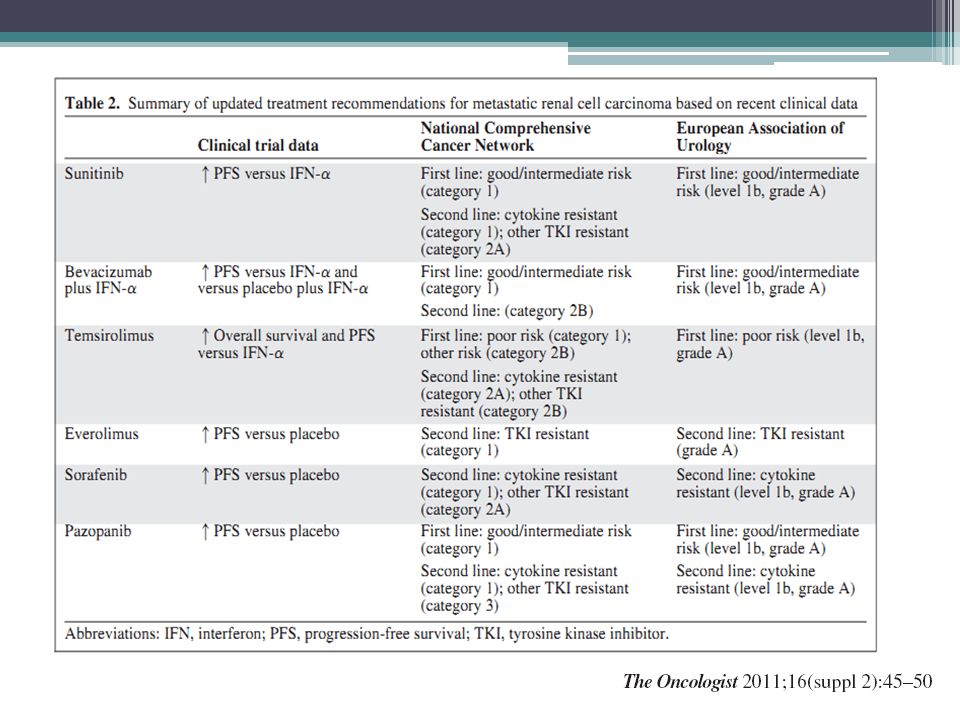
Sunitinib, Bevacizumab Plus Interferon-α, and Temsirolimus The efficacy of sunitinib, bevacizumab plus interferon(IFN)-α, and temsirolimus as first-line therapy was compared with that of IFN-α in separate randomized, phase III trials. Results showed that each of these targeted agents was superior to IFN-α in prolonging progression-free survival or overall survival times The majority of the patients in the sunitinib and bevacizumab plus IFN- trials were in the favorable or intermediate MSKCC risk groups All patients in the temsirolimus trial were classified by similar criteria as having a poor prognosis, which was equivalent to 74% of patients being classified in the MSKCC poor-risk group and 26% of patients being classified in the MSKCC intermediate- risk group

16
Sunitinib, Bevacizumab Plus Interferon-α, and Temsirolimus Sunitinib vs IFN severe adverse events (grade 3-4 toxicities) were acceptable, neutropenia(12%), thrombocytopenia(8%), hyperamylasemia(5%), diarrhea(5%), hand-foot syndrome(5%), hypertension(8%) Temsirolimus vs IFN grade 3-4 adverse adverse event seen more in temsirolimus rash, stomatitis, pain, infection, peripheral edema thrombocytopenia and neutropenia, hyperlipidemia, hypercholesteremia, hyperglycemia
 were acceptable, neutropenia(12%), thrombocytopenia(8%), hyperamylasemia(5%), diarrhea(5%), hand-foot syndrome(5%), hypertension(8%) Temsirolimus vs IFN grade 3-4 adverse adverse event seen more in temsirolimus rash, stomatitis, pain, infection, peripheral edema thrombocytopenia and neutropenia, hyperlipidemia, hypercholesteremia, hyperglycemia")
17
Pazopanib Most recently, the efficacy of pazopanib was shown to be superior to that of placebo in a phase III RCT (VEG105192) Patients with no prior treatment or 1 prior cytokine-based treatment, randomized (2:1) to pazopanib 800mg once daily or placebo. The MSKCC favorable- and intermediate-risk groups PFS was prolonged with pazopanib 9.2 mo vs 4.2 mo Adverse reactions; m/c grade 3 toxicity was hepatotoxicity grade 1 or 2 diarrhea, high BP, hair color change, nausea, loss of appetite, vomiting, fatigue, weakness

18
Everolimus The efficacy of everolimus in patients who failed treatment with sorafenib or sunitinib was superior to that of placebo and best supportive care in a recent phase III RCT (RECORD 1 trial) The majority of patients in that trial were in the MSKCC favorable- and intermediate-risk groups, and benefits of everolimus relative to placebo were observed across all risk groups The median PFS everolimus 4.0 vs placebo 1.9 months Most common adverse effect: stomatitis, rash, fatigue
 The majority of patients in that trial were in the MSKCC favorable- and intermediate-risk groups, and benefits of everolimus relative to placebo were observed across all risk groups The median PFS everolimus 4.0 vs placebo 1.9 months Most common adverse effect: stomatitis, rash, fatigue")
19
Sorafenib The efficacy of sorafenib in previously treated patients,>80% of whom had failed prior cytokine-based therapy, was superior to that of placebo, establishing a second-line therapy option. (TARGET) ▫ More than 99% of patients in that trial were of MSKCC favorable or intermediate risk
 ▫ More than 99% of patients in that trial were of MSKCC favorable or intermediate risk.")
Similar presentations









 Alone or in Combination with Carboplatin/Paclitaxel (CP) in Never or Light Former Smokers with Advanced Lung.>")




 Treated with Anti Vascular Endothelial Growth Factor (VEGF)>")


 with Newly Diagnosed Multiple Myeloma (NDMM) Receiving Lenalidomide and Low-Dose Dexamethasone.>")

>")
 in Metastatic Castration-Resistant Prostate Cancer (mCRPC): Results from a Phase II Randomized Discontinuation Trial Hussain M et.>")
 for Renal Cell Cancer Blocking VEGF in Kidney Cancer is like Blocking Estrogen in Breast Cancer.>")
