Download presentation
Presentation is loading. Please wait.

1
Palliative Care and Home- Based Primary Care: An Intertwined Population Health Delivery Model Moderator: Theresa Soriano, MD MPH Panelists: Ina Li, MD Pam Miner, MD Steven Robertson, MD Mary Sayre, MSN RN Barbara Sutton MSN APRN ACHPN

2
Faculty Disclosures Li – no relevant disclosures Miner – no relevant disclosures Robertson – no relevant disclosures Sayre – no relevant disclosures Soriano – no relevant disclosures Sutton – no relevant disclosures

3
Describe the burden of chronic illness and suffering in the home-limited population, and how palliative care can address these needs Identify practical ways to effectively incorporate palliative care principles into home-based clinical practice Objectives

4
Agenda Introduction Goals of Care & Anticipatory Guidance Pain Management 101 Non-pain symptom management Delirium Panel Q&A

5
improving the experience of care, improving the health of populations, and reducing per capita costs of health care. 5 Improving the U.S. Health Care System

6
Illness, complexity and cost 50% account for 3% of total costs 6 Tier 1 Tier 2 Tier 3 10% of patients account for 64% of total costs 40% account for 31% of total costs Conwell LJ, Cohen JW. March 2005. AHRQ

7
Shifting Expectations Our population: Homebound Average age 84 Requiring assistance with ADLs, multiple comorbidities About 26% die each year. Frailty, functional dependence, cognitive impairment, symptom distress and increasing family support needs due to long-term caregiving burden. In addition to geriatric decline, specific disease progression which in our population include multiple progressive chronic diseases, add to the need to move to a palliative focus of care. Chai, E., Meier, D., Morris, J., & Goldhirsch, S. (2014).
..")
8
Medicare Definition of Palliative Care Palliative care means: patient and family-centered care that optimizes quality of life by anticipating, preventing, and treating suffering Palliative care throughout continuum of illness involves: addressing physical, intellectual, emotional, social, and spiritual needs and facilitating patient autonomy, access to information, and choice. 73 FR 32204, June 5, 2008 Medicare Hospice Conditions of Participation – Final Rule 8

9
Palliative Care – Principles vs. Specialty All clinicians should be skilled at palliative care principles of: (1) basic pain and symptom management concurrent with active disease management (2) communication with patients and loved ones about prognosis, expectations, and advance care planning Complex or late-stage conditions and situations require palliative care specialists who are: (1)Specialty trained/certified (2)Typically part of a trained interdisciplinary team (physician, an advanced practice nurse, a social worker and a chaplain) (3)Separate from, or part of, hospice benefit https://www.capc.org/payers/palliative-care-definitions/
 basic pain and symptom management concurrent with active disease management (2) communication with patients and loved ones about prognosis, expectations, and advance care planning Complex or late-stage conditions and situations require palliative care specialists who are: (1)Specialty trained/certified (2)Typically part of a trained interdisciplinary team (physician, an advanced practice nurse, a social worker and a chaplain) (3)Separate from, or part of, hospice benefit")
10
Population-Based Health Severely Ill Manage symptoms> conditions Chronically Ill Manage conditions > symptoms Well Optimize health Palliative Care Wellness Services: Wellness Diet and Nutrition Mammography Colonoscopy Mental Health Social programs Advance Directives Goals & Preferences An integrated system of services and partnerships meeting the needs of the community throughout the entire continuum of health Slide adapted from Buxton & Twaddle

11
↑ Primary care visits; ↑ Home health; ↑ Hospice High vaccination rates High rates Advance Care Planning ↑ Patient/Caregiver Satisfaction ↓ Caregiver Burden Improved symptom management including pain, anxiety, depression, fatigue, and loss of appetite 10-17% lower Medicare Costs ($8,477 savings per beneficiary; $6.1 million total savings) ↓ Hospitalizations 9-44% ↓ Emergency Department 10% Low institutionalization rate (<10% NH admission) Value of HBPPC DeJonge, et al. Effects of Home-Based Primary Care on Medicare Costs in High-Risk Elders. JAGS, Oct 2014 Edes, et al. Better Access, Quality and Cost for Clinically Complex Veterans with Home-Based Primary Care JAGS Oct 2014 Ornstein, et al. Reduction in Symptoms for Homebound Patients Receiving Home-Based Primary and Palliative Care. Journal of Palliative Medicine Sept 2013 Melnick, et al. House Calls: California Program For Homebound Patients Reduces Monthly Spending, Delivers Meaningful Care. Health Affairs Jan 2016.

12
The proof is in IAH... “…Independence at Home participants saved over $25 million in the demonstration’s first performance year – an average of $3,070 per participating beneficiary – while delivering high quality patient care in the home.” https://www.cms.gov/Newsroom/MediaReleaseDatabase/Press-releases/2015-Press-releases-items/2015-06-18.html

13
HBPC and Palliative Care are Uniquely Effective in Achieving the Triple Aim Both HBPC and Palliative Care: Treat the patient and family, not the disease Reduce symptom burden Incorporate caregivers, social factors and care preferences into care plans Advocate for appropriate care in line with above Which thereby: Creates appropriate, patient-centered plans of care Improves patient and family satisfaction Reduces costs

14
Goals of Care & Anticipatory Guidance Pam Miner, MD Mary Sayre, MSN RN Housecall Providers, Portland OR

15
Advance Care Planning involves: Exploration of values, priorities, preferences, what gives meaning to one’s life, and what defines an acceptable quality of life. Identification of personal goals of care in the event of a severe illness, and the discussions of different treatment options in the context of these goals. May include: future hospitalizations, home/homecare preferences, resuscitation, goals and expectations of comfort and symptom management, spiritual support, life-sustaining treatment (ventilator, artificial nutrition). IOM Dying in America –http://www.iom.edu/Reports/2014/Dying-In-America-Improving- Quality-and-Honoring-Individual-Preferences-Near-the-End-of-Life.aspx.
. IOM Dying in America – Quality-and-Honoring-Individual-Preferences-Near-the-End-of-Life.aspx..")
16
Case 96 yo female ischemic cardiomyopathy, aortic regurgitation, heart failure with preserved EF, atrial fibrillation with RVR and anxiety Functional status had been declining multiple hospitalizations and procedures

17
Key Points in Conversation Understanding: “What is your understanding now of where you are with your illness?” Information Preferences: “How much information about what is likely to be ahead with your illness would you like from me (or from your PCP)?” “With whom do you prefer I share this information with?” Prognosis: Share based on information preferences Goals: “If your health situation worsens, what are your most important goals?” Bernacki R, Block S JAMA Internal Medicine published online Oct 20, 2014. doi:10.1001/jamainternmed.2014.5271

18
Key Points in Conversation Fears/Worries: “What are you biggest fears and worries about the future with your health?” Function: “What abilities are so critical to your life that you can’t imagine living without them?” Trade-offs: “If you become sicker, how much are you willing to go through for the possibility of gaining more time?” Family: “How much does your family know about your priorities and wishes? Bernacki R, Block S JAMA Internal Medicine published online Oct 20, 2014. doi:10.1001/jamainternmed.2014.5271

19
Additional Language What is life like for you right now? What do you understand about your illness? You seem to understand a lot, but let me clarify some items... Given what you understand about your illness now, what do you hope for? What do you worry about? While we hope for the best response to treatments, if you do decline further despite everyone’s best efforts, it is important to understand if there are any situations that you would consider an unacceptable sort of life (give examples of realistic outcomes expected with progression of their disease process)
.")
20
Case

21
Challenges to advance care planning Designated health care agent must understand and agree to follow the patient’s wishes for care Patient and family fear of discussing health care issues Conversations may be time-consuming and require prognostication on the part of the clinician Completed documentation of patient preferences for care need to be accessible to those providing the care Chai, E., Meier, D., Morris, J., & Goldhirsch, S. (2014). Geriatric palliative care, a practical guide for clinicians. New York: Oxford University Press.
. Geriatric palliative care, a practical guide for clinicians. New York: Oxford University Press..")
22
Team Support What we’ve learned from IAH regarding episodes of care, transitions and impact of patient preferences. An integrated team approach that is patient- centered and coordinated can improve patient outcomes as well as follow patient preferences. (IOM, 2012). IOM Core Principles & Values of Effective Team-Based Health Care -2012, Discussion Paper, www.iom.edu/tbc. www.iom.edu/tbc
. IOM Core Principles & Values of Effective Team-Based Health Care -2012, Discussion Paper,")
23
Transitions of Care Key opportunities to re-clarify goals of care when a team can help: Change in medical condition when hospitalization may be warranted During a hospitalization Prior to hospital discharge After discharge How goals of care are documented in your E.H.R. can affect how they are followed.

24
Documentation Physician Orders for Life Sustaining Treatment (POLST) adopted in Oregon since 1991. Advance directives, POLST, and goals of care conversations are documented multiple places in our EHR. At the time of hospitalization the POLST is a key item of information that sent to the hospital and reinforced by our transition team members. www.polst.org

25
Case

26
Effective Goals of Care Discussion Focus on the patient’s life, goals, experience of illness, fears and concerns Allow silence and acknowledge and explore emotions Provide prognostic information in ranges, acknowledging inherent uncertainty Gets the patient or family talking more than 50% of the time Explores effective treatments that support patient goals

27
Basic Principles of End-of-Life Communication Patients want the truth about prognosis. You will not harm your patient by talking about end-of-life issues. Anxiety is normal for both patient and clinician during these discussions. Patients have goals and priorities besides living longer. Learning about patient goals and priorities empowers you to provide better care. Bernacki R, Block S JAMA Internal Medicine published online Oct 20, 2014. doi:10.1001/jamainternmed.2014.5271

28
Pain Management Steven Robertson, MD, Medical Director Kindred House Calls, Cleveland, OH Kindred at Home Hospice – Cleveland, OH

29
AAHCM Clinical Competencies

30
What is Pain? Merriam-Webster Dictionary: An unpleasant feeling occurring as a result of injury or disease, usually localized in some part of the body Bodily suffering characterized by such feelings Taber’s Medical Dictionary: Unpleasant feeling conveyed to the brain by sensory neurons More than sensation, but physical awareness of pain Includes subjective interpretation of the discomfort, including the emotional response

31
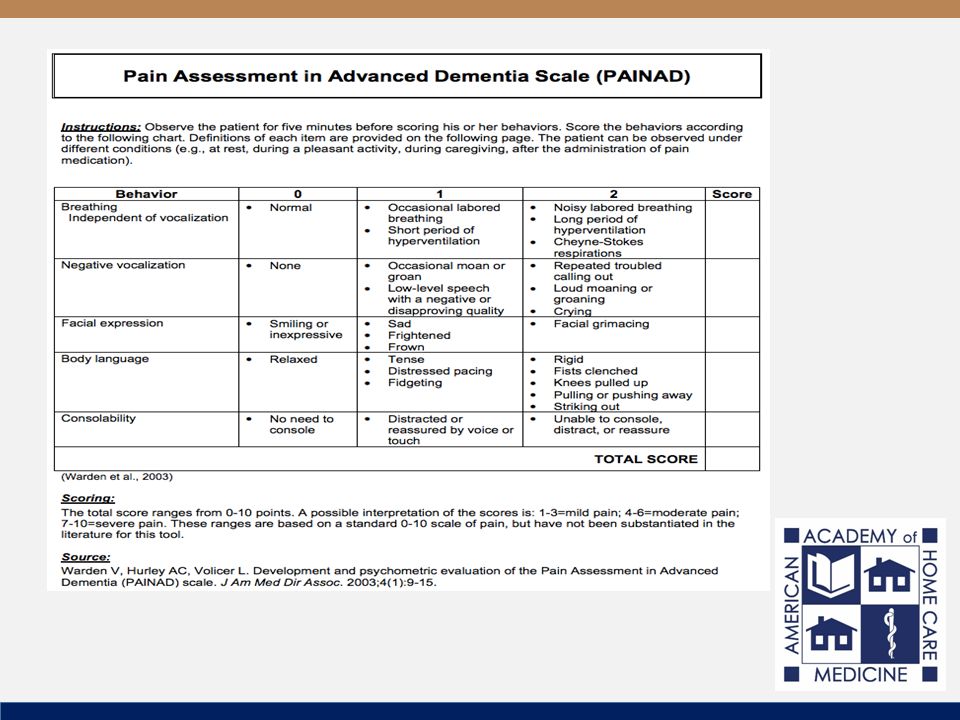
How is it described and measured? Need for Comprehensive Assessment to Identify Site & Type of Pain: Bone, soft tissue, nerve-related, smooth muscle, others Sharp, dull, achy, burning, crampy, constant, intermittent Use Pain Scales to Rate Severity and Track Changes 0-10 Numeric Rating Scale Wong Baker FACES Pain Rating Scale

33
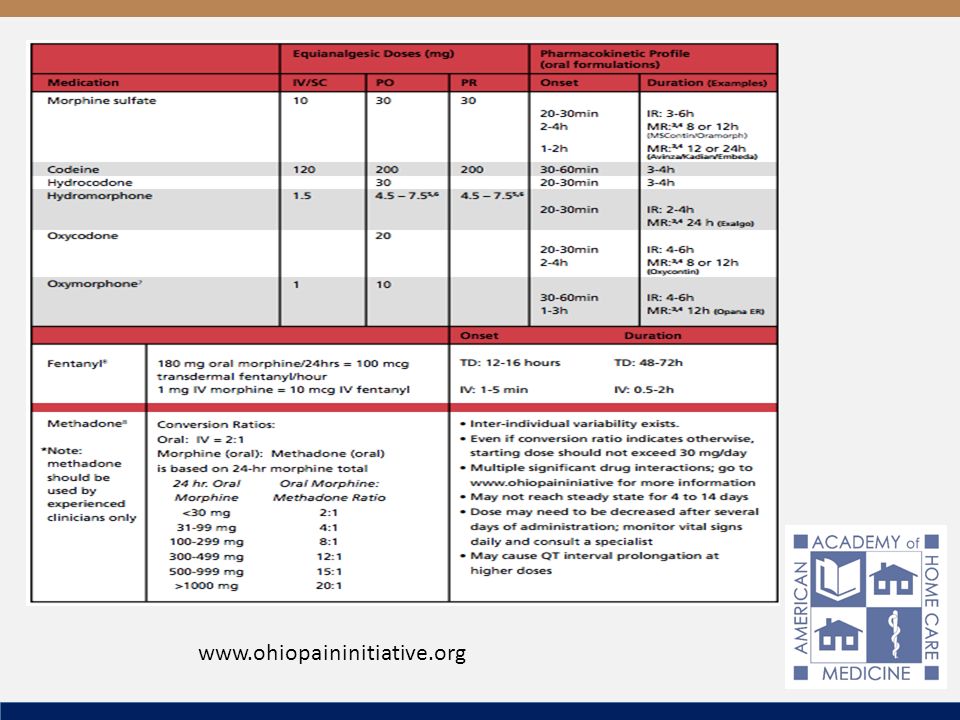
General Principles of Pain Medication 1.Three step approach: scheduled non-opioid for mild pain, low dose opioid for moderate pain, strong opioid for severe pain 2.Schedule medications based on duration of action rather than allowing pain to spiral out of control Always have Short Acting “Rescue” available for Breakthrough Pain Rescue dosage is 10-15% of the 24 hour around the clock dose 3.Always think ahead to manage known opioid side effects (expected and manageable: constipation, nausea, pruritis, sedation versus serious: anaphylaxis) 4.Plan ahead for route of administration, but understand IM, IV and SQ pumps often unnecessary, uncomfortable, problematic 5.Add Co-analgesics as indicated by type of pain to reduce need for opioid escalation and for better pain control 6.Reassess often, reduce opioids when able and when undue effects 7.Request expert help for switching between opioids, especially Methadone
 4.Plan ahead for route of administration, but understand IM, IV and SQ pumps often unnecessary, uncomfortable, problematic 5.Add Co-analgesics as indicated by type of pain to reduce need for opioid escalation and for better pain control 6.Reassess often, reduce opioids when able and when undue effects 7.Request expert help for switching between opioids, especially Methadone")
34
www.ohiopaininitiative.org
35
Non-Opioid Co-Analgesics Bone and Soft Tissue: NSAIDS (Ibuprofen, Naproxyn), COX2 (Celebrex) Steroids (Dexamethasone, Prednisone) for Metastases Anxiety: Benzodiazepine (Lorazepam, Diazepam) Butyrophenon (Haloperidol) Nerve Damage (Neuropathy, Entrapment): Anticonvulsants (Gabapentin, Pregabalin, Valproic Acid) Antidepressants (Cymbalta, even Zoloft) Smooth Muscle Spasms (Bladder, Bowel): Anticholinergic (Hyoscyamine, Dicyclomine, Oxybutinin)
, COX2 (Celebrex) Steroids (Dexamethasone, Prednisone) for Metastases Anxiety: Benzodiazepine (Lorazepam, Diazepam) Butyrophenon (Haloperidol) Nerve Damage (Neuropathy, Entrapment): Anticonvulsants (Gabapentin, Pregabalin, Valproic Acid) Antidepressants (Cymbalta, even Zoloft) Smooth Muscle Spasms (Bladder, Bowel): Anticholinergic (Hyoscyamine, Dicyclomine, Oxybutinin)")
36
The Myths of Morphine Morphine causes addiction: There is a very small chance of psychological addiction in one who is prescribed appropriate doses of opiates for the treatment of pain or dyspnea Morphine is too strong: It is exactly as strong as hydrocodone (equianalgesic) Morphine caused delirium in the hospital: Hospitalization and untreated pain more often cause delirium Morphine causes respiratory depression: Massive doses to opioid naïve patients would be required Morphine Accelerates Death and is Euthanasia: When the medication is given to ease active pain or dyspnea, that is the desired effect. It does not cause the death that is actively occurring apart from and without the Morphine

37
Opioid Induced Neurotoxicity Increasingly recognized undue effect of opioids Accumulation of Toxic Metabolic Byproducts which are actually neuroexcitants Clinical Manifestations: Myoclonus Hyperalgesia and Allodynia Seizures Misinterpreted as disease related pain, and opioid dose is often rapidly escalated, worsening symptoms Do not provide reversal agents (Naloxone) Reduce dose, rotate to another opioid, hydrate, benzodiazepines www.palliative.info/teaching_material/oin.ppt
 Reduce dose, rotate to another opioid, hydrate, benzodiazepines")
38
Not all distress is due to Physical Pain www.palliative.info/teaching_material/oin.ppt

39
Summary HBPC clinicians are the first line defense against pain, with readily available specialist backup Become familiar with Morphine Equivalent Daily Dosing, Equianalgesic tables (Fentanyl) Schedule according to half life, with breakthrough dosing available, adjust frequently based upon response Counsel patients, families, caregivers regarding the myths of pain medication, advocate for pain relief Recognize that all distress is not due to physical pain Experienced, expert interdisciplinary team are readily available for difficult cases
 Schedule according to half life, with breakthrough dosing available, adjust frequently based upon response Counsel patients, families, caregivers regarding the myths of pain medication, advocate for pain relief Recognize that all distress is not due to physical pain Experienced, expert interdisciplinary team are readily available for difficult cases")
40
Non-Pain Symptoms Barbara Sutton, MSN APRN ACHPN Amita Healthcare

41
Objectives Understand Management of Dyspnea at Home Understand pharmacologic and non- pharmacologic treatment options Brief discussion of: Nausea/vomiting Anorexia/cachexia Oxford Textbook of Palliative Medicine (5ed) Cherney, Fallon, Kaasa, Portenoy, Currow 2015 Fast Facts; Palliative Care Network of Wisconsin http://www.mypcnow.org/#!fast-facts/c6xbhttp://www.mypcnow.org/#!fast-facts/c6xb
 Cherney, Fallon, Kaasa, Portenoy, Currow 2015 Fast Facts; Palliative Care Network of Wisconsin")
42
Managing Dyspnea Dyspnea is subjective, just as pain is. Dyspnea is whatever the patient says it is.

43
Dyspnea is associated with many disease states Respiratory infection COPD/Asthma Ascites CHF Anemia Pulmonary fibrosis Tumor invasion

44
Dyspnea Assessment Acute or chronic? Does it change with position change? What are associated symptoms: anxiety, restlessness, spiritual/existential issues? Aggravating/alleviating activities Response to medications Use of Borg Scale (American Thoracic Society)
.")
45
CauseAssessmentManagement Options COPD/AsthmaWheezing, coughBronchodilators, corticosteroids, oxygen Respiratory infection Fever, cough, inspiratory crackles, secretions Expectorants, antibiotics AscitesDecreased breath sounds, fluid on palpation Diuretics, paracentesis CHFEarly inspiratory crackles, edema, anemia Diuretics, oxygen Pulmonary fibrosis Diminished breath sounds, cough, cyanosis, tachycardia, fatigue, chest pain Opioids, oxygen AnemiaDizziness, hypotension, pallor, fatigue Blood transfusions, oxygen Center to Advance Palliative Care https://www.capc.org/https://www.capc.org/

46
Non-Pharmacological Management of Dyspnea Open windows or use fan (trigeminal nerve) Position to facilitate chest expansion Pursed lip breathing Cool humidified air Relaxation/distraction Reiki Spiritual practices Energy conservation Oxygen 1-3 Liters per minute
 Position to facilitate chest expansion Pursed lip breathing Cool humidified air Relaxation/distraction Reiki Spiritual practices Energy conservation Oxygen 1-3 Liters per minute")
47
Medications Morphine is the gold standard 10-20 mg by mouth (pill or liquid) every 1-4 hours as needed may use extended release for chronic dyspnea Risks: Constipation Use with caution in bradycardia, hypotension, CO 2 retention Reduced respiratory rate Start low, go slow For tachypnea, may be beneficial
 every 1-4 hours as needed may use extended release for chronic dyspnea Risks: Constipation Use with caution in bradycardia, hypotension, CO 2 retention Reduced respiratory rate Start low, go slow For tachypnea, may be beneficial")
48
Anxiolytics Opioids Benzodiazepines Lorazepam 0.5-2 mg every 6-12 hours as needed Not first line

49
Nausea and vomiting Nausea – an uneasiness of the stomach that does not always lead to vomiting Vomiting – forcible voluntary or involuntary emptying of stomach contents

50
Causes Unrelieved pain/headaches Constipation GI stasis Bowel obstruction Anxiety Oral candidiasis Medication side effects Chemotherapy Hypercalcemia Motion sickness/dizziness Infection Dehydration/electrolyte imbalance GERD Peptic ulcer disease Gall bladder disease CAD Esophagitis – cancer or infectious Medications – NSAIDs, ASA, steroids, caffeine, alcohol Center to Advance Palliative Care https://www.capc.org/https://www.capc.org/

51
Non-pharmacologic Treatments NPO Clear liquid diet Reduce stress Small frequent meals Eat slowly Good oral hygiene Sit upright for 1 hour after eating

52
Anorexia/Cachexia Defined as lack of appetite and tissue wasting Complex pathophysiology Interventions should be addressed as part of the patient and family’s goals Often irreversible related to a terminal disease process Normalize the natural way we eat and drink less

53
Potential Causes Pain N/V Depression Medication side effects Constipation Altered mental status Fatigue Impaired gastric emptying Dyspnea Mucositis/candidiasis

54
Non-pharmacological Treatments Avoid weighing Good oral hygiene Favorite foods Different textures/temperatures Nutritional supplements Nurture non-food activities Normalize decrease in appetite Give permission to eat less/feed less

55
Delirium Ina Li, MD, Director of Clinical Geriatrics Christiana Care Health System, DE

56
Definition Is a syndrome of disturbance of consciousness, with reduced ability to focus, sustain, or shift attention, that occurs over a short period of time and fluctuates over the course of the day

57
Only 20% of cases recognized by physicians Only 50% of cases recognized by nurses Under-Recognized

58
Outcomes Delirium in elderly (>65 years) patients was associated with an increased risk of Death Institutionalization Dementia 1.Witlox J, Eurelings LS, et al. Delirium in the elderly patients and the risk of post-discharge mortality, institutionalization, and dementia: a meta-analysis. JAMA. 2010; 304(4): 443-451 2.Siddiqi N, House AO. Occurrence and outcome of delirium in medical in-patients: a systematic literature review. Age Ageing. 2006; 35(4): 350-364.
: Siddiqi N, House AO. Occurrence and outcome of delirium in medical in-patients: a systematic literature review. Age Ageing. 2006; 35(4):")
59
Precipitating Factors Mnemonic: Drugs Electrolyte Disturbances Lack of Drugs Infection Reduce sensory input or mobility Intracranial Urinary, fecal Myocardial, pulmonary Surgery

60
Confusion Assessment Method (CAM) Diagnosis Requires #1 and #2 and either # 3 or #4 1.Acute Change in Mental Status and Fluctuating Course Is there evidence of an acute change in cognition from the patient’s baseline Does the abnormal behavior fluctuate during the day? 2. Inattention: Does the patient have difficulty focusing inattention? Digit span Serial 7s “World” backwards 3.Disorganized thinking Is the patient’s thinking disorganized or incoherent? 4.Altered level of consciousness Is the patient’s mental status anything other than alert? Khan, B, Zawahiri, M, et al. Delirium in Hospitalized patient: implications of Current Evidence on Clinical Practice and Future Avenues for Research – A systematic evidence review. J of Hospital Medicine, 2012; 7(7): 580-589
:")
61
Treatment Step 1: Identify and treat reversible causes Step 2: Maintain behavioral control Step 3: Anticipate and prevent complications Step 4: Restore Function

62
Agitation Pharmacologic treatment may be necessary for behavior that is dangerous to patient or others and does not respond to other management strategies Hypoactive Delirium was the most prevalent delirium subtype Hosie, A, Davidson, P, et al. Delirium prevalence, incidence, and implications for screening in specialist palliative inpatient care settings: A systematic review. Palliative Medicine. 27(6): 486-498
:")
63
Pharmacologic Therapy AgentDosageBenefitsAdverse Events Haloperidol0.25-1 mg po, im, pr, or IV q 4 hr prn agitation Few Hemodynamic effects EPS, especially if >3 mg/day Olanzapine2.5 mg po or im q 12, max dosage 20 mg q 24 Fewer EPS than haloperidol More sedating than haloperidol Quetiapine25-50 mg po q 12 Fewer EPS than haloperidol More sedating than haloperidol; hypotension Risperidone0.25-1 mg po q 4h Similar to haloperidol Might have slightly fewer EPS Lorazepam0.25-1 mg po or IV q 8 hr Use in sedative or alcohol withdrawal More paradoxic agitation, respiratory depression than haloperidol Campbell N, Boustani M, et al. Pharmacological management of delirium in hospitalized adults: a systematic evidence review. J Gen Intern Med. 2009: 24:848-853.

64
Prevention of Complications Non-Pharmacologic Return to usual routine High-quality Sleep Avoid psychotropics, anticholinergics, Benzodiazepines, and opioids Prevent electrolyte disturbance and dehydration Adequate lighting Hearing aids Improve communication and re-orientation

65
Restore Function

66
Panel Conclusions Both HBPC and palliative care expertly address chronic illness and suffering in the home-limited population Delivering HBPC and palliative care in the home can improve patient experience, outcomes and cost Clinicians can adopt basic palliative care principles into daily HBPC practice, and should help patients access specialty palliative care, including hospice, when appropriate

67
Additional resources Hospice and Referral Criteria http://www.caringinfo.org/i4a/pages/index.cfm? pageid=1 http://www.caringinfo.org/i4a/pages/index.cfm? pageid=1 Clinical and Advocacy Resources https://getpalliativecare.org/ https://www.capc.org/ http://www.nhpco.org/resources/end-life- care--resourceshttp://www.nhpco.org/resources/end-life- care--resources http://www.epec.net/ http://aahpm.org/

68
Panel Q&A Pam Miner: PMiner@housecallproviders.orgPMiner@housecallproviders.org Mary Sayre: MSayre@housecallproviders.orgMSayre@housecallproviders.org Steven Robertson: Steven.Robertson@kindredhousecalls.comSteven.Robertson@kindredhousecalls.com Barb Sutton: Barbara.Sutton@amita.netBarbara.Sutton@amita.net Ina Li: ILi@Christianacare.orgILi@Christianacare.org Theresa Soriano: theresa.soriano@mountsinai.orgtheresa.soriano@mountsinai.org Go to: 2Shoesapp.com/AAHCM20162Shoesapp.com/AAHCM2016 1.Click on the session you are in 2.Ask and vote on questions

Similar presentations









 January 21, 2014 Delirium and Dementia.>")









 1.>")