Download presentation
Presentation is loading. Please wait.

2
Messy Inferior STEMI J. Jeffrey Marshall, MD, FSCAI December 8, 2012

3
Disclosures None pertinent to this presentation

4
Clinical Presentation 70 y/o WM with no prior cardiac history Sudden onset of chest, shoulder, and arm pressure “Transient” ST elevation in the inferior leads on 1 st 12 lead in the ambulance; 2 nd ECG with normal ST segments In route given ASA 325 mg chewed, Plavix 600 mg p.o., 60 U/kg heparin IV Hemodynamically stable in route STEMI team activated from ambulance; ETA 10 minutes

5
Clinical Presentation Chest pain had gradually subsided in route to the hospital From the paramedics, the following history and physical was obtained: PMH 30 yr h/o HTN, no hyperlipidemia SH Retired Miami fire fighter/paramedic, on vacation Wife is retired RN No TOB Physical Exam “Very fit appearing” male in NAD, but anxious 168/92 P 92 RR 16 CV, pulmonary and vascular exam were unremarkable

6
Clinical Presentation As he was being unloaded from the ambulance to go to the cath lab, he had VF arrest and CPR was initiated He was diverted to the ER where he was intubated had defibrillation, CPR and ACLS was started He was quickly resuscitated Cath team and attending arrived in the cath lab and were ready for receiving patient after resuscitation Saw him briefly in ER, spoke to wife

7
ECG in the ER

8
Clinical Presentation He was transferred to the cath lab and in the elevator he had two more VF arrest and was defibrillated X 3 in the elevator CPR was initiated as no palpable pulse was present, he briefly regained a pulse As he rolled into the cath lab he had diarrhea all over the gurney He had another VF arrest and CPR was begun as he was being transferred onto the cath table

9
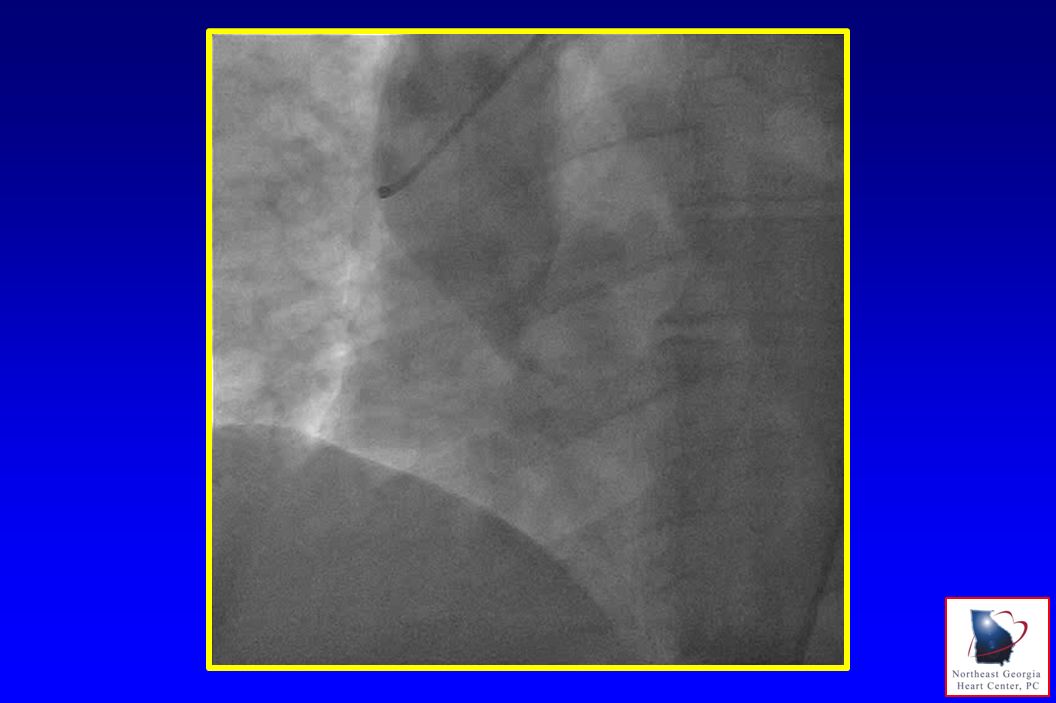
Intervention He had no palpable pulse only perfused CPR beats on the cath table Access via R FA with a 6 Fr JR 4 guide catheter After multiple attempts RCA could not be cannulated Angio of R cusp performed

11
Intervention CPR continued and access attempted in L CFA After multiple defibrillations, ACLS protocol, CPR, good ABGs, resuscitation efforts were stopped

12
Death in the Cath Lab An unexpected death,….. From an unexpected etiology Diagnosis missed in the ER CXR (even in retrospect) in the ER not suggestive of dissection Clinical history not suggestive of dissection The “fog” of the STEMI with too much focus on D2B and E2B How will you handle this as you become the attending of record?
 in the ER not suggestive of dissection Clinical history not suggestive of dissection The fog of the STEMI with too much focus on D2B and E2B How will you handle this as you become the attending of record .")
13
Medical Liability Highest risk is in patients with unexpected outcomes with whom you have little rapport Cardiologists are at high risk

14
Medical Liability Jenna AB, Seabury S, Lakdawalla D, et.al. Malpractice risk according to physician specialty. N Engl J Med 2011;365:625-36 Proportion of physicians facing malpractice claims annually by specialty

15
Medical Liability Seabury S, Chandra A, Lakdawalla D, et.al. Defense costs of medical malpractice claims. N Engl J Med 2012;369:14 Mean defense costs paid and unpaid by specialty

16
Medical Liability

17
Talking with the Wife Empathy Explain what happened – “the whole truth” Offer to help

18
Messy Inferior STEMI

Similar presentations



















 Definition of ACS Signs and symptoms of ACS Gender and age related difference in ACS Pathophysiology.>")


