Download presentation
Presentation is loading. Please wait.

1
personalized medicine in lung cancer R4 김승민

2
Personalized Medicine in Lung Cancer patients with specific types and stages of cancer should be treated according to standardized predetermined protocols the molecular characterization of tumors genome wide RNA expression, DNA copy-number and sequence analyses, and microRNA and proteomic profiling individualized selection of treatment as determined by the characteristics of the patient and the tumor. Lung cancer EGFR TKI (gefitinib, erlotinib) ALK kinase inhibitor crizotinib
 ALK kinase inhibitor crizotinib.")
3
EGFR TKI (gefitinib, erlotinib)
")
4
Incidence of EGFR gene mutations (global data from literature; n=2880) EGFR mutation (%) EthnicityGenderSmoking HxHistology Non asianasianMale FemaleNon smoker AdenoNon-adeno
 EGFR mutation (%) EthnicityGenderSmoking HxHistology Non asianasianMale FemaleNon smoker AdenoNon-adeno")
5
EGFR mutations in NSCLC

6
EGFR: First line VS second line ?

7
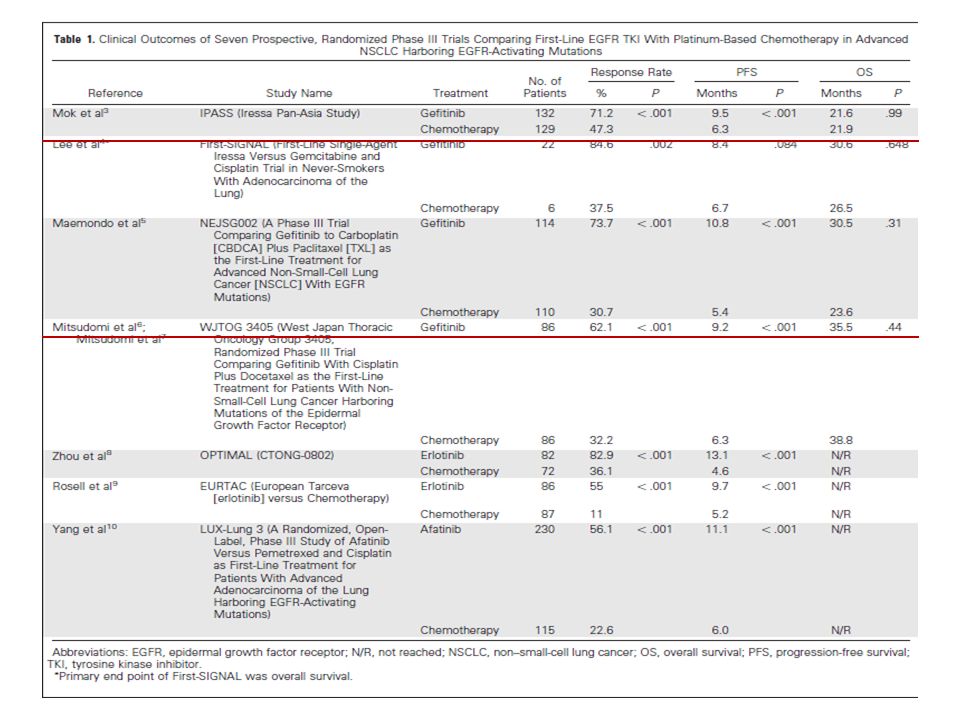
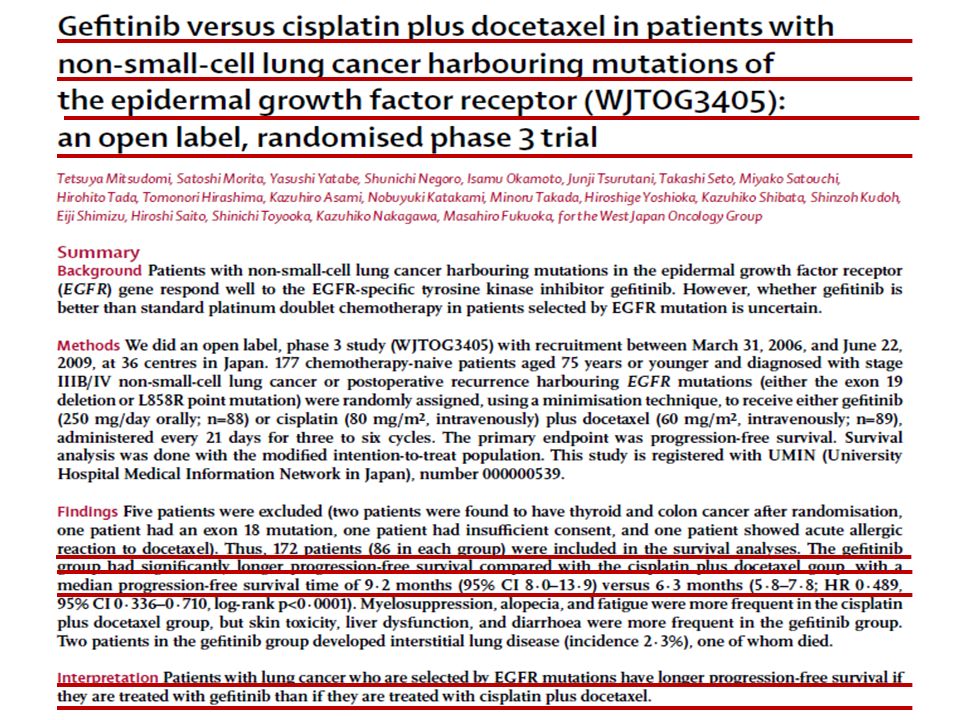
EGFR TKI is recognized as a standard first-line therapy for patients with activating EGFR mutations. All six randomized studies higher tumor response rates and longer progression-free survival none of these studies has been able to demonstrate improvement in overall survival (OS). the use of first- or second-line EGFR TKI and explore the potential differences between the two orders of administration
. the use of first- or second-line EGFR TKI and explore the potential differences between the two orders of administration.")
9
IPASS Gefitinib (250 mg / day) Carboplatin (AUC 5 or 6) / paclitaxel (200 mg / m 2 ) 3 weekly # 1:1 randomisation Patients Chemonaïve Age ≥18 years Adenocarcinoma histol ogy Never or light ex-smok ers* Life expectancy ≥12 weeks PS 0-2 Measurable stage IIIB / IV disease Primary Progression-free survival (no n-inferiority) Secondary Objective response rate Overall survival Quality of life Disease-related symptoms Safety and tolerability Exploratory Biomarkers EGFR mutation EGFR-gene-copy number EGFR protein expression Endpoints Mok et al NEJM 2009
 Carboplatin (AUC 5 or 6) / paclitaxel (200 mg / m 2 ) 3 weekly # 1:1 randomisation Patients Chemonaïve Age ≥18 years Adenocarcinoma histol ogy Never or light ex-smok ers* Life expectancy ≥12 weeks PS 0-2 Measurable stage IIIB / IV disease Primary Progression-free survival (no n-inferiority) Secondary Objective response rate Overall survival Quality of life Disease-related symptoms Safety and tolerability Exploratory Biomarkers EGFR mutation EGFR-gene-copy number EGFR protein expression Endpoints Mok et al NEJM 2009")
10
IPASS

12
second line EGFR-TKI Use of second-line and/or third-line EGFR TKI in patients with EGFR mutation multiple prospective single-arm studies, retrospective biomarker analyses of phase II studies, and limited subgroup analysis from phase III studies Current data on treatment outcomes of second- and/or third-line EGFR therapy are inconsistent, and there is a possible explanation for the lower tumor response rates

14
First-line Therapy difference in exposure to EGFR TKI difference in quality of life better tolerance by patients with poor performance status deferral of whole-brain radiation therapy for patients with brain metastasis

15
First-line Therapy difference in exposure to EGFR TKI difference in quality of life better tolerance by patients with poor performance status deferral of whole-brain radiation therapy for patients with brain metastasis

16
First-line Therapy difference in exposure to EGFR TKI difference in quality of life better tolerance by patients with poor performance status deferral of whole-brain radiation therapy for patients with brain metastasis

17
EGFR: First line VS second line ?

18
ALK in lung cancer

19
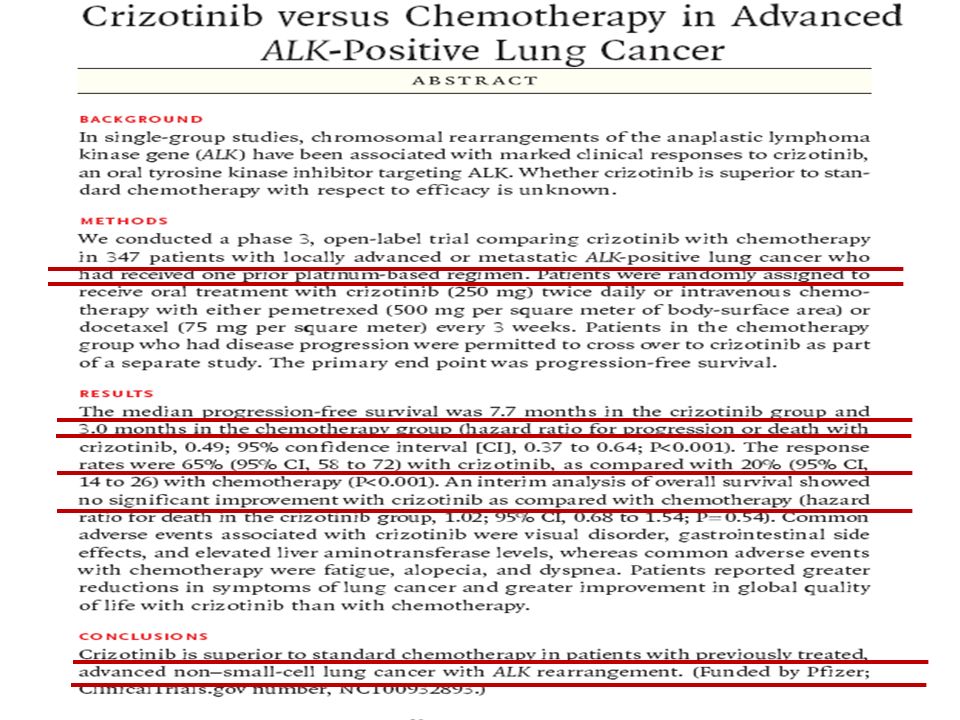
Introduction ALK rearrangement several distinctive clinicopathologic features. Absence of smoking history.. among patients with ALK-positive lung cancer, more than 90% are never- or light smokers (as 10 pack-years). younger age at diagnosis adenocarcinoma histology absence of other oncogenic drivers. study of crizotinib was in progress when EML4-ALK was reported in lung cancer.
. younger age at diagnosis adenocarcinoma histology absence of other oncogenic drivers. study of crizotinib was in progress when EML4-ALK was reported in lung cancer..")
20
Introduction NCCN Current guidelines all patients with advanced, non squamous NSCLC for both EGFR mutation and ALK rearrangement. newly diagnosed, ALK-positive patients can be prescribed crizotinib in the first-line setting. the NCCN does recommend crizotinib as first-line therapy in advanced, ALK-positive NSCLC. This recommendation to use crizotinib as first-line therapy is largely based on our experience with EGFR-mutant NSCLC

23
Bone metastases and skeletal-related events Mechanisms

24
histologic subtype is clearly an important factor in selecting among standard cytotoxic chemotherapies the presence of key oncogenic alterations predicts responsiveness to selective targeted therapies activating mutations and chromosomal rearrangements Lung cancer EGFR TKI (gefitinib, erlotinib) ALK kinase inhibitor crizotinib Personalized Medicine in Lung Cancer
 ALK kinase inhibitor crizotinib Personalized Medicine in Lung Cancer")
25
First line VS second line Six randomized studies improvement in tumor response rate and PFS over platinum-based combination chemotherapy difference in exposure to EGFR TKI difference in quality of life better tolerance by patients with poor performance status deferral of whole-brain radiation therapy for patients with brain metastasis EGFR TKI Ex: gefitinib, erlotinib

26
ALK is now a validated kinase target in lung and other cancers. ALK-positive cancers are oncogene ALK-positive lung cancer demonstrated impressive activity and clinical benefit patients with ALK-positive lung cancer invariably relapse with crizotinib as a result of the development of resistance ALK inhibitor

Similar presentations






 and N+, chemotherapy should be added.>")




 Alone or in Combination with Carboplatin/Paclitaxel (CP) in Never or Light Former Smokers with Advanced Lung.>")
 alone or in combination with carboplatin/paclitaxel (CP) in never or light former smokers with advanced lung.>")






