Download presentation
Presentation is loading. Please wait.

1
Nutritional Support in Geriatrics Dr A Norouzy Associate Professor in Nutrition Mashad University of Medical Sciences

2
Definition of Terms OLD – usual categorization –Young Old – 65 -74 –Middle Old – 75 – 84 –Old Old - 85 and older HETEROGENEOUS POPULATION

3
Geriatric Problems What geriatric problems impact nutritional status?

4
Sensory Changes with Aging Decreased sense of smell due to decreased olfactory cells Decreased vision Hearing loss Tactile loss

5
Sensory Changes with Aging Decreased number of taste buds – Loss of sweet and salty – Less loss of bitter and sour –Dry mouth prevents adequate tasting

6
Geriatric Problems Weight Loss Sarcopenia Dehydration Swallowing Dementia Pressure Ulcers Constipation Depression

7
Optimal Weight Weight is Primary Parameter Standard Tables vs. TRENDS –Identify unintentional weight change –Attention to trends Optimal Weight –Maximize function and quality of life –Minimize disease risk

8
Usual Weight Trends Gradual Weight Gain – Middle Age Peak Weight at 75 years Gradual Weight Loss after age 75 Epidemiology

9
Unintentional Weight Loss Weight loss >5% in 30 days >7.5% in 90 days (three months) >10% in 180 days (6 months) Example: –5% 7-8# in 154# = 146# –10% 15# in 154# = 139# Long Term Care Guidelines American Healthcare Association
 >10% in 180 days (6 months) Example: –5% 7-8# in 154# = 146# –10% 15# in 154# = 139# Long Term Care Guidelines American Healthcare Association")
10
Identifying Weight Change Weight History Change in Clothing Fit Decrease in Functional Ability Dietary Intake Records These methods are readily accessible and cost effective

11
Weight and Mortality Potter, et al, 1988 Corrada, et al, 2006

12
Strategies: Calories Avoid unnecessary dietary restrictions Encourage use of nutrient dense foods Use more frequent meals plus supplements or snacks

13
Strategies: Calories Use foods that are well liked frequently Provide double portions of favorite foods Add calories by using sauces, gravies, toppings, and fats Emphasize calorie containing liquids to meet fluid needs Practical Suggestions

14
Obesity numbers reaching older age as obese (30.5% in NHANES) physical and cognitive disability risk of dependency and institutionalization health care costs, poor health outcomes, mortality Houston, et al, JADA, Nov. 2009

15
Obesity Treatment Goal: To better manage health and maintain independence longer Minimize loss of muscle mass –Adequate protein –Exercise (aerobic and resistance) Minimize loss of bone density –Adequate calcium, Vitamin D –Exercise (weight bearing) Adequate nutrient intake
 Minimize loss of bone density –Adequate calcium, Vitamin D –Exercise (weight bearing) Adequate nutrient intake")
16
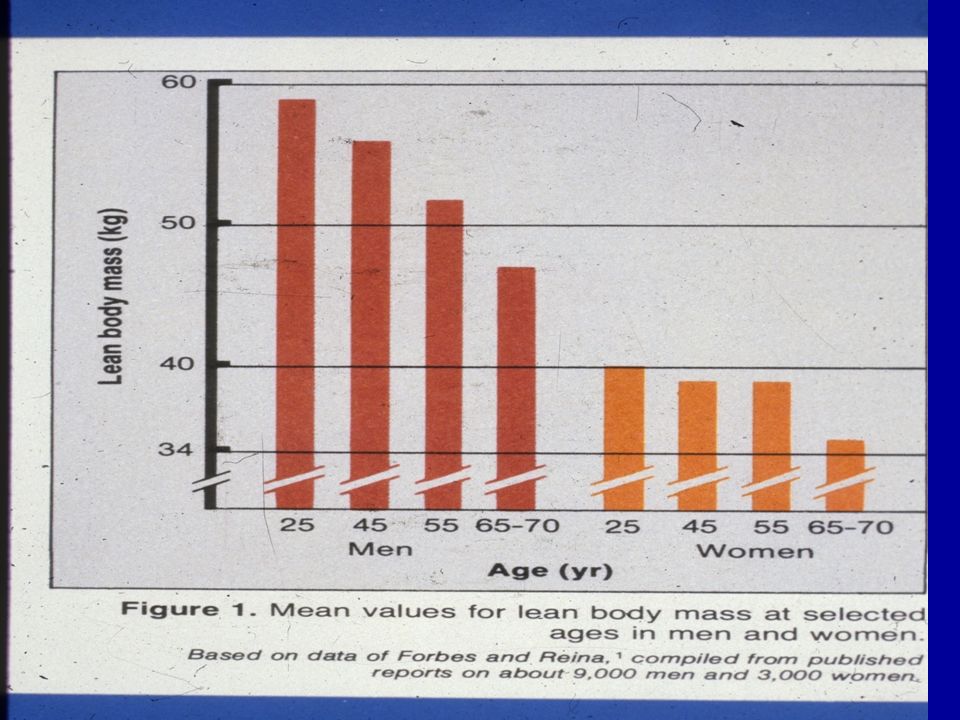
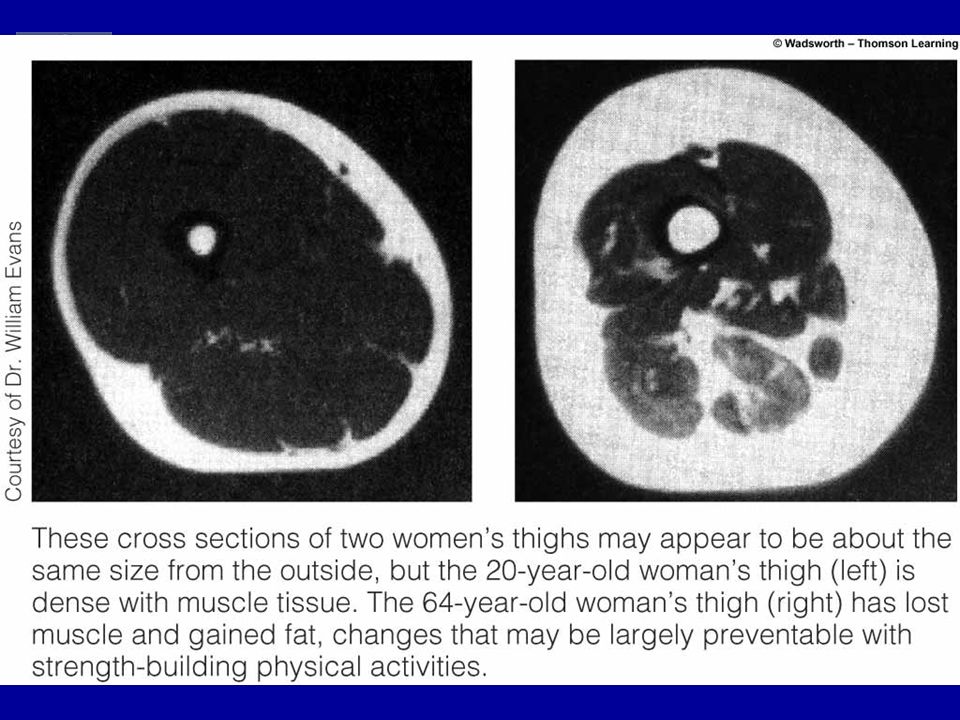
Sarcopenia Definition: Loss of muscle mass in aging. Results: Lower basal metabolic rate –Weakness -Decreased Functional Status –Reduced Activity Level –Decreased Bone Density Practical Application –Progressive Resistance Exercises –Adequate Protein

19
Protein Higher protein intake required to maintain nitrogen balance Contributors: –Lower energy intake –Impaired insulin action –Decreased efficiency of protein utilization J.Nutr.Healthy Aging, 2006

20
Protein 1.0-1.25 gm/kg/day At least one high protein food at each of three meals Physical activity to maintain muscle mass -Exercise against resistance

21
Dehydration: Causes Decreased thirst sensation with aging More dependent on others to obtain fluid Decreased ability to concentrate urine Increased incidence of incontinence with self-imposed fluid restriction Increased use of medications contributing to dehydration Increased losses: vomiting, diarrhea, fever

22
Dehydration: Symptoms Decreased Skin Turgor Dry Mouth and Mucosal Membranes Decreased Urine Volume Darker Urine Constipation Acute Weight Loss CONFUSIONCONFUSION

23
Dehydration Practical Application Treat Cause Set Fluid Goal Goal: 30 cc/kg or 1 cc/Kcal Replace Additional Fluid Losses Drink Fluid At and Between Meals Use Foods Which Have Fluid Value

24
Fluid:Nutrient Comparison FluidFree Water (cc)Calories/Protein Water240 cc (100%) 0/0 Juice (Apple)210 cc (88%) 111/0 Whole Milk214 cc (89%) 150/8 Instant Breakfast 217 cc (80%) 250/13 Fruit Beverage Supplement 191 cc (79%) 300/10
Calories/Protein Water240 cc (100%) 0/0 Juice (Apple)210 cc (88%) 111/0 Whole Milk214 cc (89%) 150/8 Instant Breakfast 217 cc (80%) 250/13 Fruit Beverage Supplement 191 cc (79%) 300/10")
25
Swallowing Problems SWALLOWING SWALLOWING Swallow is difficult or hard to initiate Wet sounding voice Aspiration pneumonia in history Loss of fluid through the nose Leakage of food or liquid out of mouth when eating Overt coughing or choking with oral intake Weight loss with inadequate nutritional intake Involve Speech Pathologist and others Nutrient Density Go for Least Restrictive

26
Dementia Weight Loss Primary Nutritional Problem Stage of Disease Important Eating Behaviors

27
Eating Behaviors: Overview Eating is NOT just food Barometer of well being Social interaction Symbolic of life

28
Pressure Ulcers Screening Tool: (Example – Braden Scale) –Sensory Perception –Moisture –Activity –Mobility –Friction and Sheer –Nutrition Cooperation and Collaboration Needed –Nutrition is only one component
 –Sensory Perception –Moisture –Activity –Mobility –Friction and Sheer –Nutrition Cooperation and Collaboration Needed –Nutrition is only one component")
29
Pressure Ulcers: Nutrition Protein: 1.25 to 2.0 gm/kg Vitamin/Mineral Supplementation –Useful with poor intake or depletion –Vitamin C: 1 to 2 gm/day –Zinc Sulfate: 220 mg/day

30
Food ItemAmountDietary Fiber Apple+Orange2 medium size8-10grams Whole Wheat Bread 2 slices 4 grams Fresh Fruit2 pieces 4 grams Vegetables2 servings 4 grams Total20-22 grams Robertson’s Rule of 2’s

31
Geriatric Problems Principle: Avoid unnecessary dietary restrictions.

32
Osteoporosis High incidence of osteoporosis –33% of women 60-70 years old –66% of women > 80 years old Less efficient absorption of calcium and Vitamin D Reduced exposure to sun = reduced conversion of inactive D to active D Supplementation essential –1200-1500 mg/day

33
Serum 25-hydroxyvitamin D <20 ng/mL Deficiency 20-29 ng/mL Insufficiency 30-80 ng/mL Optimal Level >80 ng/mL Possible Toxicity

34
Prevelance of Deficiency 40 to 100% of U.S. & European elderly men & women living in the community are deficient in D >50% of postmenopausal women taking medication for osteoporosis have suboptimal levels of D (<30 ng/mL) 65% of Iranian female adult are vit D deficient
 65% of Iranian female adult are vit D deficient.")
35
Prevention & Maintenance 1000 IU Vitamin D 3 per day Daily sun exposure 5 to 30 minutes 10 am to 3 pm

36
Treatment of Deficiency 50,000 IU of Vitamin D3 weekly for 8 weeks Repeat for another 8 weeks if 25-hydroxyvitamin D <30ng/mL

37
Oral Supplementation Cochrane Systematic Review Effectiveness of nutritional supplements in elderly at risk for malnutrition Review of 62 trials –10,187 randomized patients –Maximum duration of intervention: 18 months Milne, AC, et al, Protein and energy supplementation in elderly people at risk from malnutrition. Cochrane Database of Systematic Reviews, 2009, Issue 2.

38
Oral Supplementation Significantly improved mortality in undernourished Small, consistent weight gain in 42 trials Reduced risk of complications in 24 trials No evidence of functional improvement No reduction in Length of Stay

39
Oral Supplementation Practical Suggestions Product Acceptance Taste Fatigue Supplementation not Meal Replacement

40
Oral Supplements Carbohydrate Powder Protein Powder Carbohydrate & Protein

41
متشکرم.

Similar presentations