Download presentation
Presentation is loading. Please wait.

1
HRSA’s 340B Drug Pricing Program – An Update
11th Annual PPN Conference Las Vegas, NV August 15, 2007 Christopher A. Hatwig, M.S., R.Ph.

2
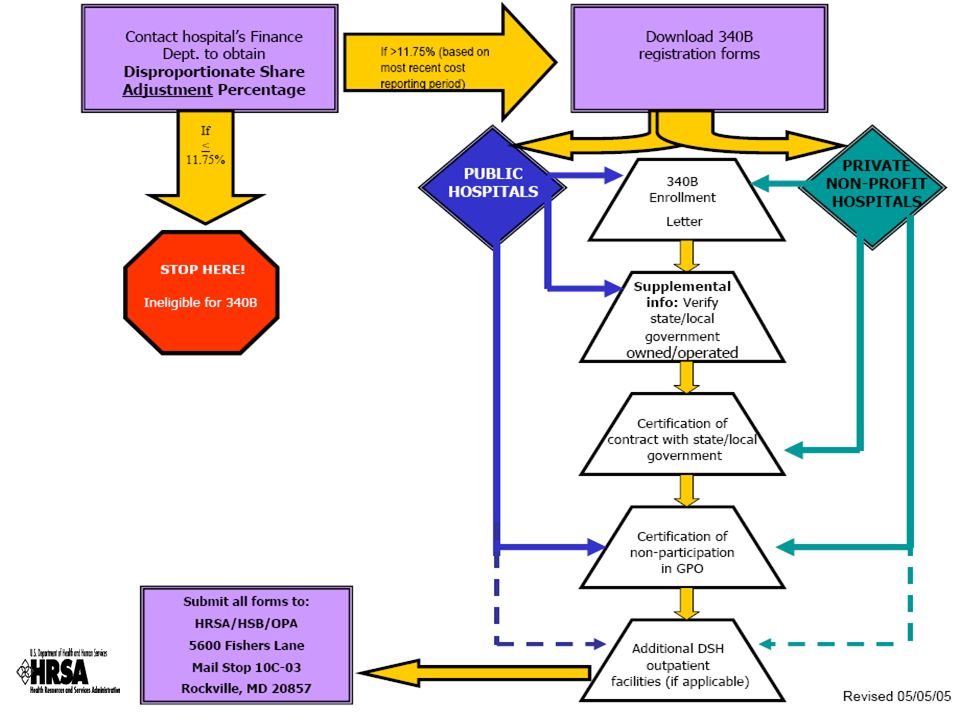
Objectives Review requirements for DSH participation in 340B
Discuss updates with the 340B Drug Pricing Program to include: The Office of Pharmacy Affairs (OPA) The Pharmacy Services Support Center (PSSC) The Prime Vendor Program (PVP) Review pending FRNs and 340B legislation
 The Pharmacy Services Support Center (PSSC) The Prime Vendor Program (PVP) Review pending FRNs and 340B legislation.")
3
Background: 340B Drug Pricing Program
1990 -Congress created Medicaid rebate law Drug manufacturers responded by increasing prices Congress passed Veteran Health Care Act (VHCA) intended to extend relief to gov’t payers of drugs Act stated that manufacturers participating in Medicaid must sign a Pricing Agreement to participate in the 340B program Provides discounts on outpatient covered drugs Required drug manufacturers to give best price to disproportionate share hospitals and certain covered entities grants Also referred to as “Section 602”, “PHS” or “340B” pricing
 intended to extend relief to gov’t payers of drugs. Act stated that manufacturers participating in Medicaid must sign a Pricing Agreement to participate in the 340B program. Provides discounts on outpatient covered drugs. Required drug manufacturers to give best price to disproportionate share hospitals and certain covered entities grants. Also referred to as Section 602 , PHS or 340B pricing.")
4
340B Covered Entities Eligible to Participate
Disproportionate Share Hospitals (DSH) FQHC LA’s HRSA Grantees: Federally Qualified Health Centers (FQHC) Hemophilia Treatment Centers Ryan White Programs (HIV programs) Sexually Transmitted Disease programs Tuberculosis Programs Title X Family Planning Clinics Urban 638 Tribal Programs
 FQHC LA’s. HRSA Grantees: Federally Qualified Health Centers (FQHC) Hemophilia Treatment Centers. Ryan White Programs (HIV programs) Sexually Transmitted Disease programs. Tuberculosis Programs. Title X Family Planning Clinics. Urban 638 Tribal Programs.")
6
What Drugs Are Covered? Non-covered drugs: Covered drugs:
Outpatient Prescription drugs Over-the-counter drugs (if accompanied by a written prescription) Clinic administered drugs within eligible facilities ER drugs Drugs in other amb care settings (e.g. day surgery) Non-covered drugs: *Vaccines Drugs given to the patient in inpatient care settings *Aggressive discounts have been negotiated for vaccines and other non-covered by the Prime Vendor Program
 Clinic administered drugs within eligible facilities. ER drugs. Drugs in other amb care settings (e.g. day surgery) Non-covered drugs: *Vaccines. Drugs given to the patient in inpatient care settings. *Aggressive discounts have been negotiated for vaccines and other non-covered. by the Prime Vendor Program.")
7
Current Patient Definition Requirements for 340B Hospitals
Three criteria to meet: 1. The covered entity must maintain records of health care services for the individual; 2. The individual must receive care from a health care professional who is employed by or under contract or other arrangements with the covered entity; and 3. Responsibility for the care provided must remain with the covered entity.

8
Inventory Management To ensure compliance and to optimize 340B savings, Most DSH will need to utilize 340B pricing within mixed (inpt/outpt) patient care settings Two options in meeting program guidelines: Separate physical inventories Virtual inventory management using split billing software Requirements to avoid diversion of 340B product: Retrospective replenishment program NDC to NDC match (11 digit match) Reports/subject to audit Create NDC-to-CDM crosswalk Identify charge unit conversions (CDM units versus purchase units) Match procurement data to utilization data via common NDC code Identify the appropriate sources of utilization data based on the process flows and the mechanism in which data will be obtained Track & validate service entities to Medicare cost report Identify covered patients Identify qualified points of service Create reports or use software to track data, create order reports, and merge wholesaler procurement reports to maintain qualified units balance Use actual utilization data and wholesaler reports to test for errors in order quantities, unit-conversions, NDC’s, etc.
 patient care settings. Two options in meeting program guidelines: Separate physical inventories. Virtual inventory management using split billing software. Requirements to avoid diversion of 340B product: Retrospective replenishment program. NDC to NDC match (11 digit match) Reports/subject to audit. Create NDC-to-CDM crosswalk. Identify charge unit conversions (CDM units versus purchase units) Match procurement data to utilization data via common NDC code. Identify the appropriate sources of utilization data based on the process flows and the mechanism in which data will be obtained. Track & validate service entities to Medicare cost report. Identify covered patients. Identify qualified points of service. Create reports or use software to track data, create order reports, and merge wholesaler procurement reports to maintain qualified units balance. Use actual utilization data and wholesaler reports to test for errors in order quantities, unit-conversions, NDC’s, etc.")
9
340B Service Options In-House Pharmacy Contracted Pharmacy
Traditional Telepharmacy Management company operated Contracted Pharmacy Community retail Mail order Prescriber Dispensing

10
Current Contract Pharmacy Guidelines
Each covered entity may use only one pharmacy to provide all pharmacy services The entity has the choice of using either an in-house pharmacy or a contract pharmacy for site There are no limits on how many in-house pharmacies a covered entity can operate Larger DSH facilities typically manage their own in-house outpatient pharmacy. Contract model more prevalent in smaller DSH and community health centers “Ship to, bill to” arrangement

11
Typical 340B Chain of Distribution
AWP $100 WAC $84 Non-340B $70 340B $51 MANUFACTURER No Medicaid Rebate WAC Chargeback 340B + Non-340B Acc’ts WHOLESALER Non-340B 340B Payment MEDICAID FEE-FOR- SERVICE Bill AAC COVERED ENTITY CONTRACT PHARMACY Dispensing Fee Bill U+C Co-pay (if applicable) Dispensed or Administered OTHER PAYERS Dispensed Co-pay ELIGIBLE PATIENT Powers Pyles Sutter & Verville, PC Bill von Oehsen (202)
 Dispensed or. Administered. OTHER. PAYERS. Dispensed. Co-pay. ELIGIBLE PATIENT. Powers Pyles Sutter & Verville, PC Bill von Oehsen. (202)")
12
The Value of 340B Savings Discounts range from 25 to 50%
DSH see savings in the range of 22 to 40% below GPO prices A Mathematica study commissioned by HRSA documented an average of 27% savings Other HRSA grantees see even great savings The 340B Prime Vendor Program also negotiates sub-ceiling discounts Although covered entities are entitled to a ceiling price that averages 51 percent of AWP, they may negotiate “sub-ceiling” discounts Additionally value may be available on inpatient drugs (more later on this)
")
13
Program Administration
Three Legs of the 340B Program Office of Pharmacy Affairs (OPA) Pharmacy Services Support Center (PSSC) 340B Prime Vendor Program (PVP) 340B Program Harry Hagel and Chris Hatwig (PVP) will discuss their respective roles immediately after my presentation. New competitive solicitation April, 2004 Five-year agreement signed September 10, 2004 1st option year (3rd full year) approved by Government May 2006 HealthCare Purchasing Partners International (HPPI) Drug price negotiation services Multiple wholesale distributor agreements Other value added products/services American Pharmacists Association (APhA) (Harry Hagel, Sr. Dir.May 2006) American Association of Colleges of Pharmacy, American Society of Health-systems Pharmacists and other partners Services to OPA and 340B covered entities (States) Information and analysis Relationships and networking Program development/Technical Assistance Partner with schools of pharmacy to encourage students to develop projects in 340B Safety-net organizations that promote access to clinically and cost effective pharmacy services. 2006/ 6 Projects 2005/ 10 Projects 2004/ 5 Projects OPA PVP PSSC
 Pharmacy Services. Support Center. (PSSC) 340B Prime Vendor. Program (PVP) 340B Program. Harry Hagel and Chris Hatwig (PVP) will discuss their respective roles immediately after my presentation. New competitive solicitation April, Five-year agreement signed September 10, st option year (3rd full year) approved by Government May HealthCare Purchasing Partners International (HPPI) Drug price negotiation services. Multiple wholesale distributor agreements. Other value added products/services. American Pharmacists Association (APhA) (Harry Hagel, Sr. Dir.May 2006) American Association of Colleges of Pharmacy, American Society of Health-systems Pharmacists and other partners. Services to OPA and 340B covered entities (States) Information and analysis. Relationships and networking. Program development/Technical Assistance. Partner with schools of pharmacy to encourage students to develop projects in 340B Safety-net organizations that promote access to clinically and cost effective pharmacy services. 2006/ 6 Projects. 2005/ 10 Projects. 2004/ 5 Projects. OPA. PVP. PSSC.")
14
Office of Pharmacy Affairs (OPA) Mission and Function Federal Register 9/21/2004
Responsible for management and oversight of the 340B Programs Manage pharmaceutical pricing agreements (PPA’s) with industry Manage covered entity eligibility and enrollment Promote access to clinically and cost-effective pharmacy services through: Maximizing the value of participation in 340B Developing innovative pharmacy services Being a Federal resource for pharmacy practice
 with industry. Manage covered entity eligibility and enrollment. Promote access to clinically and cost-effective pharmacy services through: Maximizing the value of participation in 340B. Developing innovative pharmacy services. Being a Federal resource for pharmacy practice.")
15
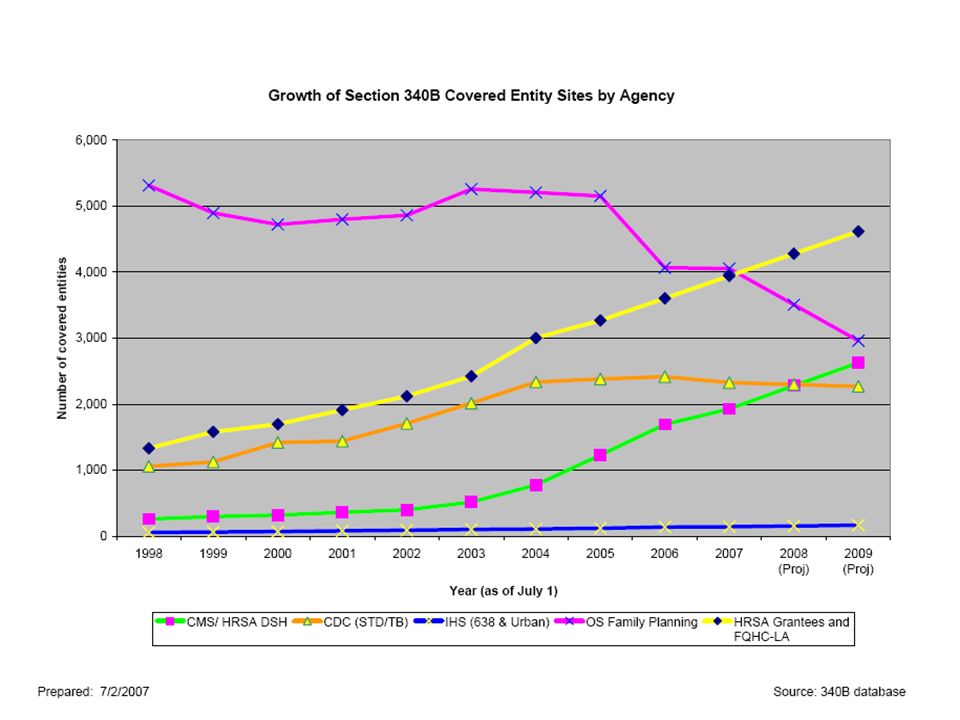
First quarter FY ,469 covered entities currently participating in the 340B Drug Pricing Program. The program has grown more than 50 percent since January 2000 and a 4.7 percent growth since January 2005. 10

17
12

18
340B Program Integrity Concerns
Office of the Inspector General (OIG Reports) Industry Covered entity compliance Diversion Patient definition Duplicate discounts Covered Entities Industry compliance Overcharges Restrictive pricing practices (specialty distributors, IVIG, etc.) Pricing transparency This is just a representative example of some of the higher profile issues, you may have others. Most manufacturer’s focus on diversion, but the for the most part it is inadvertent. Duplicate discounts occur with some frequency. Congress is focused on pricing transparency to address incorrect prices. The next OIG report (if accurate) will drive congressional action.
 Industry. Covered entity compliance. Diversion. Patient definition. Duplicate discounts. Covered Entities. Industry compliance. Overcharges. Restrictive pricing practices (specialty distributors, IVIG, etc.) Pricing transparency. This is just a representative example of some of the higher profile issues, you may have others. Most manufacturer’s focus on diversion, but the for the most part it is inadvertent. Duplicate discounts occur with some frequency. Congress is focused on pricing transparency to address incorrect prices. The next OIG report (if accurate) will drive congressional action.")
19
340B “Program Integrity Pilot Project”
Recommended by the OIG and certain drug manufacturers Test collaboration of OPA/Manufacturers to jointly publish verified price file to marketplace via the Prime Vendor Program to wholesale distributors Possible benefits: Increased pricing integrity and transparency Six manufacturers and one wholesaler currently participating; others encouraged to participate Project period: April 1, 2007 through March 30, 3008 Manufacturers Amylin Daiichi Sankyo Eli Lilly Genentech GlaxoSmithKline Schering Plough Wholesalers AmerisourceBergen McKesson Cardinal OPA Pricing Errors: Rounding error: System rounded down data above numeral five at the 6th digit URA calculation: System erroneously calculated OTC and generics as AMP -15.1% rather than AMP- 11%. _ Package size: Manufacturer reported data and the data purchased from First Data Bank (FDB) do not always agree. Exploring resolution with the manufacturers and with FDB. _ No finding of manufacturer pricing error
 do not always agree. Exploring resolution with the manufacturers and with FDB. _ No finding of manufacturer pricing error.")
20
340B Basics: Regulation and Policy
Policy issued via Federal Register Notice publication. Process - OPA drafts guidance - notice published in federal register - public comment requested/received - comments reviewed/considered - notice finalized HRSA’s OPA currently has three FRN’s pending comment and final publication

21
Proposed Guidance: Definition of Patient –72 FR 1543
Clarifies previous FRN of October 1996 A clear and enforceable definition to help ensure against diversion and support 340B program integrity Clarifies requirement to keep records of the patient’s health care Clarifies relationship between covered entity and medical provider who generates prescription of 340B drugs Provides guidance for DSHs as to which its clinics may participate in 340B Status Comment Period 1/12/07 – 03/13/07 Comments being reviewed and final publication being developed Through CE networking, contracting, and other arrangements questions about definition of CE patient have arisen. HRSA believes current definition of patient provides sufficient guidance for many situations. It is possible that some CE may have intrepreted the definition too broadly with results of potential for diversion; therefore HRSA issued Notice for comment hat includes several examples that provide CE further guidance regarding the relationship of the CE and an individual that makes that individual a patient of the CE. HRSA sought comments on elements of contract between private non-profit hospital and state/local government and different situations where private non-profit hospitals are granted governmental powers. 1.Clarifies requirement that covered entity must maintain ownership, control, maintenance, and possession of records of the patient’s health care. 2. Clarifies relationship between the covered entity and medical provider who generates prescription of 340B drugs. 3. Provides additional guidance for disproportionate share hospitals (DSHs) as to which affiliated clinics may participate in 340B. 4. Certain case management administrative activities are construed as health care 5. Loosely affiliated networks with no appropriate contractual relationship to eligible entity 6. Extension to facilities not an integrated part of the eligible DSH 7. 340B drugs are provided to employees of health facilities 8. Indian Tribes and Tribal Organizations providing unauthorized services to non-Indians 9. Sub-grantees and/or subcontractors providing services beyond the scope of the sub-grant or subcontract Some have augured that if implemented these proposed changes could significantly narrow the patient populations eligible for the 340b program. I would argue that the intent of the proposed guidelines is to clarify with greater certainty who is and who is not a “patient” of a CE for purposes of 340B. In publishing the FRN, my intent was to use the process to clarify who a patient is. The purpose of the Administrative Procedures Act is to create public dialogue on proposed rules/guidance. Through public dialogue, better rules and guidance is suppose to result.
 as to which affiliated clinics may participate in 340B. 4. Certain case management administrative activities are construed as health care. 5. Loosely affiliated networks with no appropriate contractual relationship to eligible entity. 6. Extension to facilities not an integrated part of the eligible DSH B drugs are provided to employees of health facilities. 8. Indian Tribes and Tribal Organizations providing unauthorized services to non-Indians. 9. Sub-grantees and/or subcontractors providing services beyond the scope of the sub-grant or subcontract. Some have augured that if implemented these proposed changes could significantly narrow the patient populations eligible for the 340b program. I would argue that the intent of the proposed guidelines is to clarify with greater certainty who is and who is not a patient of a CE for purposes of 340B. In publishing the FRN, my intent was to use the process to clarify who a patient is. The purpose of the Administrative Procedures Act is to create public dialogue on proposed rules/guidance. Through public dialogue, better rules and guidance is suppose to result.")
22
Proposed Guidance: Contract Pharmacy –72 FR 1540
Updates previous FR Notice of August,1996 Builds upon experience with Demonstration Projects Incorporates multiple pharmacies as standard option Network model arrangements would still require Alternative Methods Demonstration Projects (AMDPs) approval Status Comment Period 1/12/07 – 03/13/07 Comments being reviewed and final publication being developed Through CE networking, contracting, and other arrangements questions about definition of CE patient have arisen. HRSA believes current definition of patient provides sufficient guidance for many situations. It is possible that some CE may have intrepreted the definition too broadly with results of potential for diversion; therefore HRSA issued Notice for comment hat includes several examples that provide CE further guidance regarding the relationship of the CE and an individual that makes that individual a patient of the CE. HRSA sought comments on elements of contract between private non-profit hospital and state/local government and different situations where private non-profit hospitals are granted governmental powers. 1.Clarifies requirement that covered entity must maintain ownership, control, maintenance, and possession of records of the patient’s health care. 2. Clarifies relationship between the covered entity and medical provider who generates prescription of 340B drugs. 3. Provides additional guidance for disproportionate share hospitals (DSHs) as to which affiliated clinics may participate in 340B. 4. Certain case management administrative activities are construed as health care 5. Loosely affiliated networks with no appropriate contractual relationship to eligible entity 6. Extension to facilities not an integrated part of the eligible DSH 7. 340B drugs are provided to employees of health facilities 8. Indian Tribes and Tribal Organizations providing unauthorized services to non-Indians 9. Sub-grantees and/or subcontractors providing services beyond the scope of the sub-grant or subcontract Some have augured that if implemented these proposed changes could significantly narrow the patient populations eligible for the 340b program. I would argue that the intent of the proposed guidelines is to clarify with greater certainty who is and who is not a “patient” of a CE for purposes of 340B. In publishing the FRN, my intent was to use the process to clarify who a patient is. The purpose of the Administrative Procedures Act is to create public dialogue on proposed rules/guidance. Through public dialogue, better rules and guidance is suppose to result.
 approval. Status. Comment Period 1/12/07 – 03/13/07. Comments being reviewed and final publication being developed. Through CE networking, contracting, and other arrangements questions about definition of CE patient have arisen. HRSA believes current definition of patient provides sufficient guidance for many situations. It is possible that some CE may have intrepreted the definition too broadly with results of potential for diversion; therefore HRSA issued Notice for comment hat includes several examples that provide CE further guidance regarding the relationship of the CE and an individual that makes that individual a patient of the CE. HRSA sought comments on elements of contract between private non-profit hospital and state/local government and different situations where private non-profit hospitals are granted governmental powers. 1.Clarifies requirement that covered entity must maintain ownership, control, maintenance, and possession of records of the patient’s health care. 2. Clarifies relationship between the covered entity and medical provider who generates prescription of 340B drugs. 3. Provides additional guidance for disproportionate share hospitals (DSHs) as to which affiliated clinics may participate in 340B. 4. Certain case management administrative activities are construed as health care. 5. Loosely affiliated networks with no appropriate contractual relationship to eligible entity. 6. Extension to facilities not an integrated part of the eligible DSH B drugs are provided to employees of health facilities. 8. Indian Tribes and Tribal Organizations providing unauthorized services to non-Indians. 9. Sub-grantees and/or subcontractors providing services beyond the scope of the sub-grant or subcontract. Some have augured that if implemented these proposed changes could significantly narrow the patient populations eligible for the 340b program. I would argue that the intent of the proposed guidelines is to clarify with greater certainty who is and who is not a patient of a CE for purposes of 340B. In publishing the FRN, my intent was to use the process to clarify who a patient is. The purpose of the Administrative Procedures Act is to create public dialogue on proposed rules/guidance. Through public dialogue, better rules and guidance is suppose to result.")
23
Proposed Guidance: Children’s Hospitals (new FRN)
References section 6004 of the DRA Clarifies that children’s hospitals are subject to the same 340B responsibilities as other covered entities Describes application procedures for children’s hospitals Reaffirms drug manufacturers’ responsibility to furnish discounts under Pharmaceutical Pricing Agreement (PPA). Feasibility of an independent auditor to verify eligibility Status Published in Federal Register July 9, 2007 Sixty day comment period closes September 7, 2007
. Feasibility of an independent auditor to verify eligibility. Status. Published in Federal Register July 9, Sixty day comment period closes September 7,")
24
Patient Safety/Clinical Pharmacy Initiative
Patient Safety Problem: IOM reports medication errors injure 1.5 Million people and cost billions annually. Pharmacy services in HRSA programs & safety-net partners growing rapidly. HRSA desires these programs to be the best and safest in the United States. FY 2007 and FY 2008 Senate Appropriations Committee Reports Collaboration with external and internal stakeholders Major pharmacy organizations, 340B Coalition members and others Contract with Mathmatica Policy Inc. Collaborate with HRSA Quality Center; HRSA programs, ARQH, NQF and others to identify safety-net best practice models of safe and effective clinical pharmacy services Improve patient safety and improve outcomes encourage win-win relationships with colleges and schools of pharmacy sustainable and reproducible Use “collaborative care model” to transfer to other safety-net providers Celebrate what’s working Figure out what caused it to work Provide opportunity for other safety-net providers to commit to implement model that works If you think your organization excels in patient safety/ clinical pharmacy, we want to hear from you. Contact me, I want to follow up with you. Problem: IOM says Medication Errors Injure 1.5 Million People and Cost Billions Annually. Pharmacy services in HRSA programs & Safety Net partners growing rapidly. Initiative Purpose & Methods: Learn best practices from high performing Safety Net providers with low error rates and great health care outcomes Systematically apply best practices across the Safety Net, at bold national scale Generate Results: safer practices, lower error rates, more and better pharmacy services, improved health outcomes on chronic diseases, lower costs

25
FY 2008 $2.94 Million Budget Request for OPA
House & Senate Appropriations Committees Funds will enable OPA to begin to Improve Program Integrity Increase compliance with 340B pricing requirements Publish Federal Register Notices to clarify 340B guidance Improve OPA-IS and begin annual verification of covered entity data Increase stakeholder training and technical assistance Improve Program Transparency Evaluate collaborative 340B Pricing “Pilot” and possibly expand it Encourage voluntary manufacturer posting of pricing files to the 340B Prime Vendor secure Web site

26
HRSA Pharmacy Services Support Center at APhA

27
About PSSC Established through a contract between APhA and HRSA, signed September 27, 2002. Enhances Office of Pharmacy Affairs (OPA) resources to optimize the value of the 340B program in order to provide affordable, comprehensive pharmacy services that improve medication use and advance patient care and patient access to affordable drugs.
 resources to optimize the value of the 340B program in order to provide affordable, comprehensive pharmacy services that improve medication use and advance patient care and patient access to affordable drugs.")
28
Pharmacy Services Support Center
Information management Organizing pharmacy expertise and resources Responding to 340B inquiries Providing technical assistance Policy analysis Monitoring pertinent policy developments Communication and education on policy issues impacting 340B and pharmacy services. Networking Communication and education Project development

29
Learning Management System

30
PSSC PharmTA Free technical assistance for 340B-eligible entities interested in setting up or enhancing clinically and cost-effective pharmacy services To request TA: Call

31
Optimization Resources
Program Assessment financial operational compliance/integrity Implementation Plans Financial Analysis Formulary Management

32
340B Action Plans

33
Interactive Financial Analysis

34
Formulary Management

35
HRSA’s 340B Prime Vendor Program

36
The Prime Vendor Program
In addition to the cost savings available through the 340B Program, its Prime Vendor Program (PVP) provides additional savings to DSH’s and HRSA grantees The mission of the PVP is to improve access to affordable medications for all 340B covered entities by: Lowering participants’ supply costs by expanding the current PVP portfolio of sub-340B priced products Providing covered entities with access to efficient drug distribution solutions to meet their patients’ needs Providing access to other value added products and services meeting covered entities’ unique needs Participation is free and voluntary for all 340B eligible participants
 provides additional savings to DSH’s and HRSA grantees. The mission of the PVP is to improve access to affordable medications for all 340B covered entities by: Lowering participants’ supply costs by expanding the current PVP portfolio of sub-340B priced products. Providing covered entities with access to efficient drug distribution solutions to meet their patients’ needs. Providing access to other value added products and services meeting covered entities’ unique needs. Participation is free and voluntary for all 340B eligible participants.")
37
Estimated Prices For Selected Public Purchasers, as Percent AWP von Oehsen; Pharmaceutical Discounts Under Federal Law: State Program Opportunities 0% 20% 40% 60% 80% 100% AWP 100.0% AMP 80.0% Medicaid (Min.) 67.9% Medicaid Net 60.5% FSS 51.7% Private Sector Pricing 340B 49.0% FCP 47.9% VA Contract 34.6% Stephen Schondelmeyer, PRIME Institute, University of Minnesota (2001)
 67.9% Medicaid Net. 60.5% FSS. 51.7% Private Sector Pricing. 340B. 49.0% FCP. 47.9% VA Contract. 34.6% Stephen Schondelmeyer, PRIME Institute, University of Minnesota (2001)")
38
HPPI’s History as the PVP
Late AmerisourceBergen (ABC) subcontracted the responsibilities of Prime Vendor Program to HPPI Sept – HPPI awarded PVP contract by HRSA Jan/Feb – HPPI met or exceeded all 26 performance criteria within the contract. HRSA granted contract extension through 2008 July to Sept., 2007 – Program transitions to new non-profit company named Apexus
 subcontracted the responsibilities of Prime Vendor Program to HPPI. Sept – HPPI awarded PVP contract by HRSA. Jan/Feb – HPPI met or exceeded all 26 performance criteria within the contract. HRSA granted contract extension through July to Sept., 2007 – Program transitions to new non-profit company named Apexus.")
39
Apexus Non-profit subsidiary corporation - June 18, 2007
HRSA fully supported Dedicated to managing the PVP with HRSA BODs will include representation from the PVP’s participants Transition will be seamless for HRSA and PVP participants Minimal change to PVP logo

40
340B PVP Updates Contracted from a single national distributor to 13 national, regional, and specialty distributors Expanded to over 5,200 participants Contracted with 50 suppliers representing over 2,800 products and services Major MIS Related Projects: New contract management system software being implemented Major modifications to PVP participant databases Building interface to HRSA’s database for eligibility Expanding demographic data to include multiple contract pharmacy relationship and unique identifiers for participants

41
340B PVP Updates (cont.) Two additional FTE’s (Analyst, Pharmacy Director), plus Pharmacy Intern Three participant councils provide program guidance (DSH, CHC, and Title X Family Planning) Average sub-340B savings on PVP contract sales across all participants for 2006 was 17% Lilly, Wyeth, X-Gen added to list of companies posting ceiling prices Partnered with national organizations representing covered entities to conduct 340B-related education and compliance programs
 Average sub-340B savings on PVP contract sales across all participants for 2006 was 17% Lilly, Wyeth, X-Gen added to list of companies posting ceiling prices. Partnered with national organizations representing covered entities to conduct 340B-related education and compliance programs.")
42
PVP Participants by Entity Type (as of 7/19/07 – 5231 participants)
")
43
Supplier Agreements Source: 340B PVP website
Allendale Pharmaceutical Alliant Pharmaceuticals Astra-Zeneca Pharmaceuticals Abraxis Pharmaceutical Akorn Inc. ASD (flu vaccine) Bayer Diagnostics Bedford Labs Can-am Care LLC Caraco Pharmaceutical Labs Cytogen (pending) FFF (flu vaccine) G&W Laboratories Geritrex Corporation GlaxoSmithKline Hawthorne Pharmaceuticals, Inc Home Diagnostics Inc. Early Detect Lilly & Company Major Pharmaceuticals Medicure Morton Grove Pharm Inc. NitroMed Inc. Novartis Vaccines Novo Nordisk Okomoto USA Inc. Organon USA, Inc. Paddock Labs RD Plastics Co Inc. Rx Elite Holdings, Inc. Sandoz Pharmaceutical Sciele Pharma Teva Health Systems Total Pharmacy Supply Tri State Distribution Stratus Pharmaceuticals Trinity Biotech X-Gen Pharmaceuticals Watson Pharma Inc. Wyeth Pharmaceuticals
 Bayer Diagnostics. Bedford Labs. Can-am Care LLC. Caraco Pharmaceutical Labs. Cytogen (pending) FFF (flu vaccine) G&W Laboratories. Geritrex Corporation. GlaxoSmithKline. Hawthorne Pharmaceuticals, Inc. Home Diagnostics Inc. Early Detect. Lilly & Company. Major Pharmaceuticals. Medicure. Morton Grove Pharm Inc. NitroMed Inc. Novartis Vaccines. Novo Nordisk. Okomoto USA Inc. Organon USA, Inc. Paddock Labs. RD Plastics Co Inc. Rx Elite Holdings, Inc. Sandoz Pharmaceutical. Sciele Pharma. Teva Health Systems. Total Pharmacy Supply. Tri State Distribution. Stratus Pharmaceuticals. Trinity Biotech. X-Gen Pharmaceuticals. Watson Pharma Inc. Wyeth Pharmaceuticals.")
44
PVP Sub-ceiling $avings by Quarter

45
DSH Inpatient Program

46
DSH Inpatient Pricing Section 1002 of MMA: Amended Medicaid Rebate Law to exclude inpatient prices from best price reporting by drug manufacturers Program is voluntary for manufacturers Exeption to “GPO exclusion” for inpatient - Contracts can be negotiated by GPO or by DSH independently Complete and accurate lists of eligible members must be maintained by GPOs and pricing is restricted to DSH members only Some hospitals report 10% or greater in added savings over typical GPO prices

47
SNHPA Survey Results: DSH Inpatient Discounts
SNHPA survey indicates hospitals have received post-MMA inpatient discounts on only 12 percent of their most commonly used brand name drugs 70 percent of the discounts were contingent on hospitals guaranteeing a certain market share Small and rural hospitals are the least likely to receive inpatient discounts under Section 1002 because of requirements placed on contracts SNHPA has advocated for legislation to address the inpatient pricing. Members of Congress have introduced legislation that would mandate 340B pricing on DSH inpatient drugs – see S.1376 and H.R.2606

48
Safety Net Inpatient Drug Affordability Act S 1376/ HR 2606
Expands 340B program to new entities Permits GPO within inpatient Extends discounts to inpatient Credit paid to Medicaid for inpatient discounts based on formula Modifies AMP Increases OPA authority and resources for enforcement and improves pricing integrity Permits multiple contract pharmacies January 1, 2008

49
Contact Information Office of Pharmacy Affairs Phone: or Web: Pharmacy Services Support Center Phone: Web: Prime Vendor Program Phone: Web:

Similar presentations







 The.>")



 NASTAD NATIONAL ADAP TA MEETING WASHINGTON, DC JULY 30, 2014 The.>")





 Javier Menendez, RPh Pharmacy Manager Department of Medical Assistance.>")

