Download presentation
Presentation is loading. Please wait.

1
Dementia Made Easier: Tools for working with physicians & clinics Terry R Barclay, PhD Director, HealthPartners Neuropsychology

2
Outline Epidemiology and base rates Challenges to diagnosis Risks/benefits of early detection Why screen? Assessment and management tools Easy and efficient screening tools ACT on Alzheimer’s guidelines Working with physicians

4
Alzheimer’s Epidemic Epidemiological Concerns 5.2M Americans with AD in 2013 Growing epidemic expected to impact 13M Americans by 2050 and consume 1.1 trillion in healthcare spending AD Diagnostic Challenges Only 50% of pts receive formal dx Diagnosis delayed on average by 6+ Years Sig. impairment in function by time it is recognized

5
Base Rates 1 in 9 people 65+ (11%) 1 in 3 people 85+ (32%) Of those with Alzheimer’s disease: 4% <65 13% 65 -74 44% 75-84 38% 85+
 1 in 3 people 85+ (32%) Of those with Alzheimer’s disease: 4% <65 13% % % 85+")
6
Base Rates Almost 2/3 are women (longer life expectancy) Minority populations at higher risk (health/lifestyle factors) Older African Americans (2x as whites) Older Hispanics (1.5x as whites) AD 6 th leading cause of death in 2013 If disease could be detected earlier (pre-clinical stages) incidence would be much higher
 Minority populations at higher risk (health/lifestyle factors) Older African Americans (2x as whites) Older Hispanics (1.5x as whites) AD 6 th leading cause of death in 2013 If disease could be detected earlier (pre-clinical stages) incidence would be much higher")
7
Alzheimer’s Epidemic Numbers in Minnesota 201094,000 2025110,000 projected Projected % increase in AD between 2000-2025 is 25%

8
Today, Alzheimer’s Disease Is … Prevalent Expensive Fatal Misunderstood Under-diagnosed Under-treated Poorly Managed Stigmatized On the rise

9
Diagnostic Challenges

10
Cultural Ageism and defining “normal” aging MD will bring health problems to my attention Associated stigma Medical Heterogeneous baseline Many patients unaware of problem Time No lab test (only rule outs) Treatment options/efficacy Wrong diagnosis? Fear of delivering bad news Implications for physician/patient relationship

11
Fact: Most Americans want advanced notice Surveys of US adults Myth: Most people don’t want to know if they have Alzheimer’s disease %

12
Diagnostic Challenges Systemic/Institutional Low priority Few incentives Lack of procedural support Few specialists available (neurology, neuropsychology) Few community resources
 Few community resources")
13
Diagnostic Challenges International Alzheimer’s Disease Physician Survey Lack of definitive tests (65%, top barrier) Lack of communication between patients / caregiver and physicians 75% reported discussion initiated by patients/caregivers 44% “after they suspect the disease has been present for a while” 40% said patients/caregivers did not provide enough information to help them make a diagnosis Patient / Family denial (65%) & social stigma (59%) International Alzheimer’s Disease Physician Survey, 2012
 Lack of communication between patients / caregiver and physicians 75% reported discussion initiated by patients/caregivers 44% after they suspect the disease has been present for a while 40% said patients/caregivers did not provide enough information to help them make a diagnosis Patient / Family denial (65%) & social stigma (59%) International Alzheimer’s Disease Physician Survey, 2012")
14
“Beyond mountains, there are mountains.” Haitian Proverb

15
Why Screen?

16
Does Screening Make Sense? Money Time Patient care / outcomes

17
Money Cost effectiveness of early assessment and treatment? Large scale studies ongoing Getsios et al (2012) Projections based on clinical trial and follow-up registry data Compared to no assessment / no treatment: Reduction in healthcare costs by $5,300 /pp Reduction in societal costs by $11,400 / pp
 Projections based on clinical trial and follow-up registry data Compared to no assessment / no treatment: Reduction in healthcare costs by $5,300 /pp Reduction in societal costs by $11,400 / pp.")
18
Time Physician does not administer screen Rooming nurse Length of screen varies Recommended tool takes 1.5 – 3 minutes Only conducted annually Mini-Cog does not disrupt workflow & increases capture rate of cognitive impairment in primary care Borson JGIM 2007

19
Patient Outcomes: Rationale for Early Detection 1. Improve quality of life Early treatment is more effective Stabilization vs. improvement Delay functional decline Patients can make decisions regarding care Decrease burden on family and caregivers 2. Connection to services that promote independent (supported) living as long as possible RTC support/counseling intervention (Mittelman et al. Neurology 2006) Non-pharm interventions reduce NH placement by 30% and delay placement for others by 18+ months
 living as long as possible RTC support/counseling intervention (Mittelman et al. Neurology 2006) Non-pharm interventions reduce NH placement by 30% and delay placement for others by 18+ months.")
20
Patient Outcomes: Rationale for Early Detection 3. Treat reversible causes NPH, TSH, B12, hypoglycemia, depression 4. Improve management of co-morbid conditions Underlying dementia = primary risk factor of poor compliance in the elderly Affects management of ALL chronic diseases (diabetes, hypertension, anticoagulation) Brain as 6 th Vital Sign
 Brain as 6 th Vital Sign.")
21
Patient Outcomes: Rationale for Early Detection 5. Reduce ineffective and expensive crisis-driven use of healthcare resources “good” vs. “bad” healthcare Prevent diagnosis during crises (wandering, hospitalization, car accidents, bankruptcy) 6. More time to participate in clinical trials and important scientific studies Knowledge gap re: earlier stages Find a cure
 6. More time to participate in clinical trials and important scientific studies Knowledge gap re: earlier stages Find a cure.")
23
National Priorities

24
Annual Wellness Visit: Medicare Took effect January 1, 2011 Affordable Care Act Medicare will cover an annual wellness visit which will include the creation of a personalized prevention plan For first time, “detection of cognitive impairment” is core feature of the exam However, no guidance regarding: What screening tools to use What to do if patient fails screening

25
National Alzheimer’s Project Act (NAPA) Law signed into effect January 4, 2011 US Dept of Health and Human Services responsible for: Creating national plan to address Alzheimer’s disease epidemic Improve early diagnosis, care coordination and treatment Recommendations include: Physician education Dissemination of assessment tools Collaboration at state and local level to advance awareness and readiness across public and private sectors
 Law signed into effect January 4, 2011 US Dept of Health and Human Services responsible for: Creating national plan to address Alzheimer’s disease epidemic Improve early diagnosis, care coordination and treatment Recommendations include: Physician education Dissemination of assessment tools Collaboration at state and local level to advance awareness and readiness across public and private sectors")
26
Local Health Systems Numerous systems already screening HealthPartners Annual Wellness Visit Pilot Neurology, Ophthalmology, Pharmacy Allina 30,000+ screens to date Essentia Health (Duluth) Piloting with plans to roll out across entire system ACMC Piloting in one clinic with plans for expansion
 Piloting with plans to roll out across entire system ACMC Piloting in one clinic with plans for expansion")
27
Easy Practice Tips

28
Practice Tips Raise your expectation of the older patient Clinical interview Let patient answer questions without help Remember: Social skills remain intact Easy to be fooled by a sense of humor, irritability, reliance on old memories, or quiet/affable demeanor Subjective interviews FAIL to detect dementia in early stages

29
Practice Tips Red flags Repetition (not normal in 7-10 min conversation) Tangential, circumstantial responses Losing track of conversation Frequently deferring to family Over reliance on old information/memories Inattentive to appearance Unexplained weight loss or “failure to thrive”
 Tangential, circumstantial responses Losing track of conversation Frequently deferring to family Over reliance on old information/memories Inattentive to appearance Unexplained weight loss or failure to thrive")
30
Practice Tips Family observations: ANY instances whatsoever of getting lost while driving, trouble following a recipe, asking same question repeatedly, mistakes paying bills Ask: “Let’s suppose your family member was alone on a domestic flight across the country and the trip required a layover with a gate change. Would he/she be able to manage that kind of mental task on his/her own?”

31
Practice Tips Intact older adult should be able to: Describe 2 current events in some detail Describe what happened on 9/11, New Orleans disaster Name the current President and 2 immediate predecessors Describe medical history and names of some medications

32
Cognitive Screening Tools

33
Screening Initial considerations Research findings re: early detection Balance b/w time and sensitivity/specificity How will your practice incorporate screening? Who will administer tests? MDs, nurses, social workers, allied health professionals What happens when screen is positive?

34
Screening Measures Wide range of options Mini-Cog (MC) Mini-Mental State Exam (MMSE) St. Louis University Mental Status Exam (SLUMS) Montreal Cognitive Assessment (MoCA) All but MMSE free online in public domain
 Montreal Cognitive Assessment (MoCA) All but MMSE free online in public domain.")
35
Screening Measures Do NOT Allow patient to give up prematurely or skip questions Deviate from standardized instructions Offer multiple choice answers Bias score by coaching Be soft on scoring Score ranges already padded for normal errors Deduct points where necessary – be strict

36
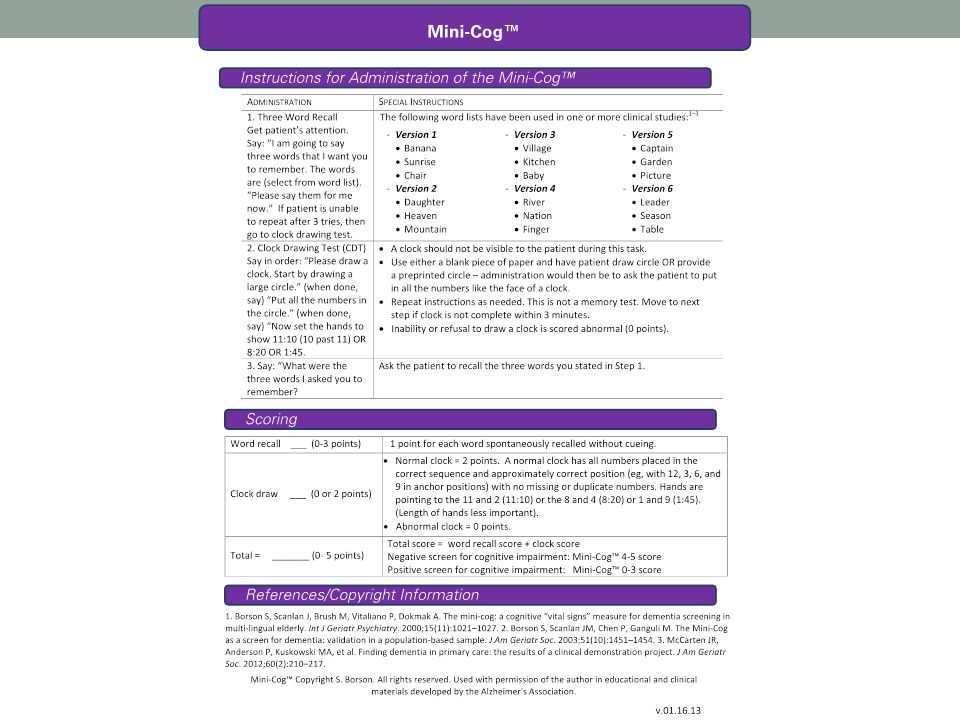
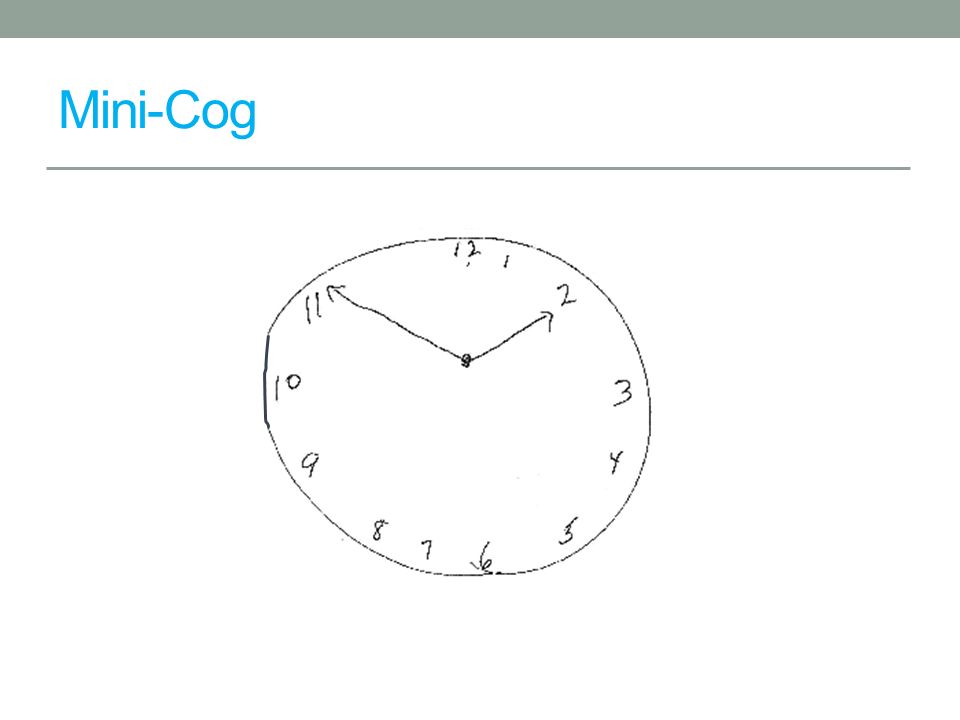
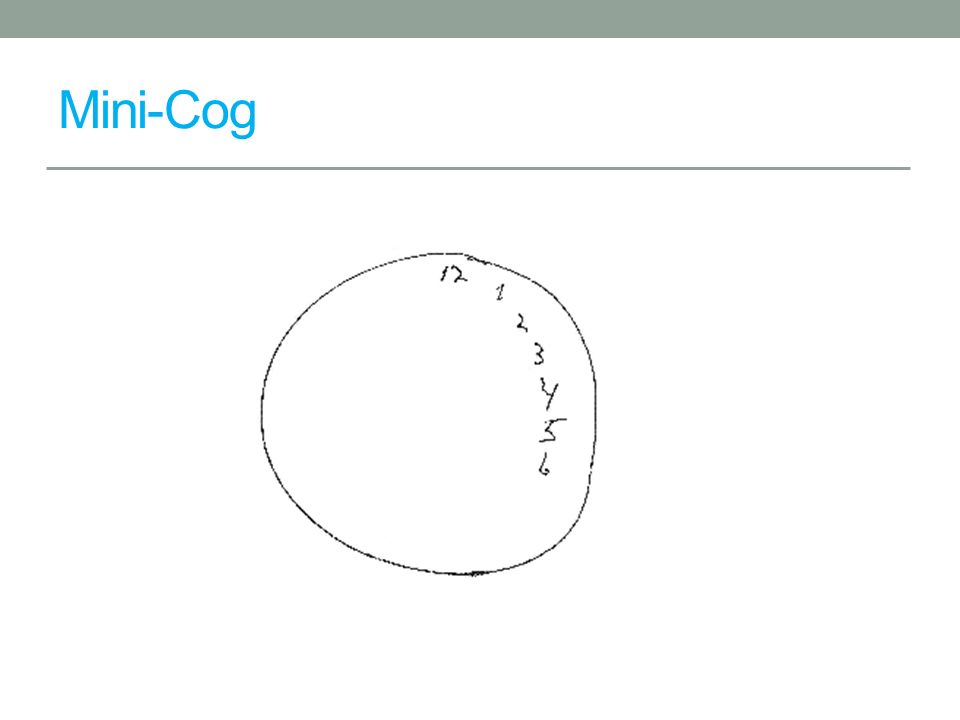
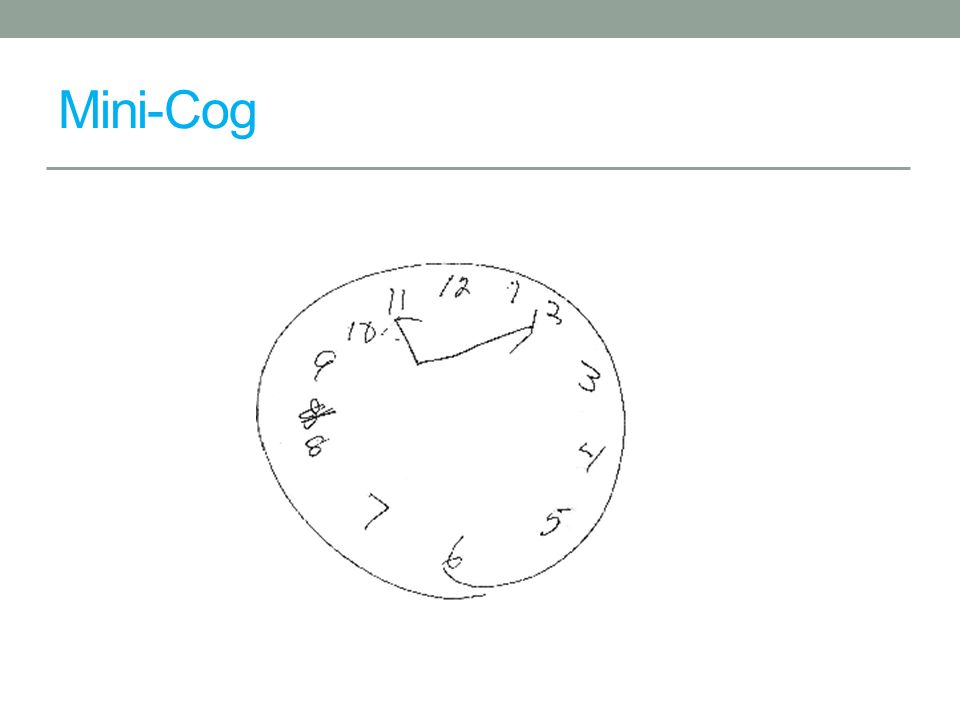
Mini-Cog Contents Verbal Recall (3 points) Clock Draw (2 points) Advantages Quick (2-3 min) Easy High yield (executive fx, memory, visuospatial) Subject asked to recall 3 words Leader, Season, Table Subject asked to draw clock, set hands to 10 past 11 +3 +2
 Clock Draw (2 points) Advantages Quick (2-3 min) Easy High yield (executive fx, memory, visuospatial) Subject asked to recall 3 words Leader, Season, Table Subject asked to draw clock, set hands to 10 past")
38
Mini-Cog Pass > 4 Fail 3 or less Borson S., Scanlan J, Brush M et al. 2000. The Mini-Cog: A cognitive “vital signs” measure for dementia screening in multi-lingual elderly. Int J Geriatr Psychiatry, 15, 1021-1027.

39
Mini-Cog Pros Easy to administer Minimal time commitment Clock sensitive to visuospatial & executive dysfunction Simple scoring and interpretation Cons Not as sensitive for MCI or early dementia when compared to longer screens Brevity means less information to interpret

40
Mini-Cog

46
Performance unaffected by education or language Borson Int J Geriatr Psychiatry 2000 Sensitivity and Specificity similar to MMSE (76% vs. 79%; 89% vs. 88%) Borson JAGS 2003 Does not disrupt workflow & increases rate of diagnosis in primary care Borson JGIM 2007 Failure associated with inability to fill pillbox Anderson et al Am Soc Consult Pharmacists 2008
 Borson JAGS 2003 Does not disrupt workflow & increases rate of diagnosis in primary care Borson JGIM 2007 Failure associated with inability to fill pillbox Anderson et al Am Soc Consult Pharmacists")
47
Screen Failure MiniCog = <4 OR memory complaints by patient/family Schedule follow-up appt Insist on family collateral Perform more complex test (MOCA, SLUMS, MMSE)
")
48
MMSE

49
Pass > 26 Fail 25 or less

50
Pros Widely accepted and validated for dementia screening 30-point scale well known and score easily interpretable Measures orientation, working memory, recall, language, praxis Cons Scale developed 40 years ago, before MCI criteria and when early dementia less well understood Lacks sensitivity to MCI and early dementia Takes 7+ min. to administer Copyright issues MMSE

51
SLUMS

52
Pass > 26 Fail 25 or less

53
Pros More measures of executive functioning Good balance between easy and difficult items More sensitive than MMSE in detecting MCI and early dementia 30-point scale similar to MMSE Score range for MCI and dementia Free online Cons Takes 10 min. to administer Slightly more complex directions than MMSE Less name recognition than MMSE SLUMS

54
MoCA

55
Pass > 26 Fail 25 or less

56
Pros Much more sensitive than MMSE for MCI and early dementia More content tapping higher level executive fx 30-point scale similar to MMSE Translations available in 35+ languages Free online Cons Takes 10-14 min. to administer More complex administration and directions than MMSE MoCA

57
Screening Tool Selection Montreal Cognitive Assessment (MoCA) Sensitivity: 90% for MCI, 100% for dementia Specificity: 87% St. Louis University Mental Status (SLUMS) Sensitivity: 92% for MCI, 100% for dementia Specificity: 81% Mini-Mental Status Exam (MMSE) Sensitivity: 18% for MCI, 78% for dementia Specificity: 100% Larner et al Int Psychogeriatr 2012; Nasreddine et al J Am Geriatr Soc 2005; Tariq et al Am J Geriatr Psychiatry 2006; Ismail et al Int J Geriatr Psychiatry 2010
 Sensitivity: 92% for MCI, 100% for dementia Specificity: 81% Mini-Mental Status Exam (MMSE) Sensitivity: 18% for MCI, 78% for dementia Specificity: 100% Larner et al Int Psychogeriatr 2012; Nasreddine et al J Am Geriatr Soc 2005; Tariq et al Am J Geriatr Psychiatry 2006; Ismail et al Int J Geriatr Psychiatry")
58
ACT on Alzheimer’s Tools Provider Toolkit

59
What is ACT on Alzheimer’s? statewide collaborative voluntary 50+ ORGANIZATIONS 150+ INDIVIDUALS Impacts of Alzheimer’s BUDGETARYSOCIAL PERSONAL

60
Genesis of ACT on Alzheimer’s 2009 Legislative Mandate for Alzheimer’s Disease Working Group (ADWG) Legislative Report Filed in January 2011 ACT on Alzheimer’s is second generation of work focusing on implementation
 Legislative Report Filed in January 2011 ACT on Alzheimer’s is second generation of work focusing on implementation")
61
sustain caregivers raise awareness & reduce stigma Goals of ACT on Alzheimer’s identify & invest in promising approaches increase detection & improve care equip communities

62
www.actonalzheimers.org

63
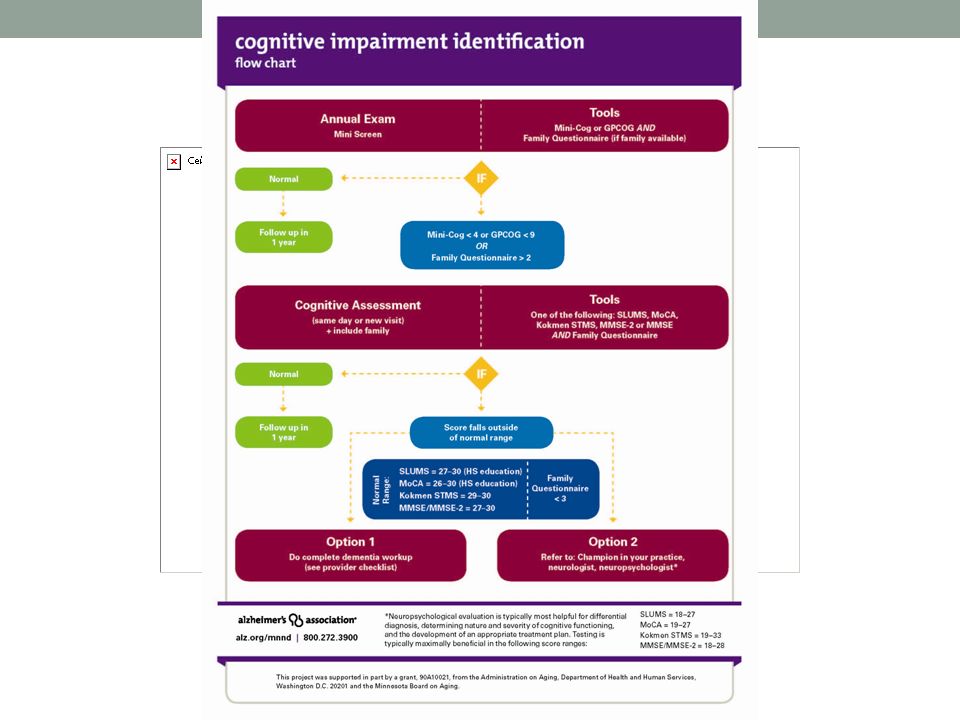
Provider Practice Tools Cognitive screening flow chart Dementia work-up Intervention Checklist

66
Diagnostic Workup History & physical Objective cognitive measurement Diagnostics Labs Imaging ? More specific testing (e.g., neuropsychological exam)? Diagnosis Family meeting
. Diagnosis Family meeting.")
67
Diagnosis Alzheimer’s disease: 60-80 % Includes mixed AD + VD Lewy Body Dementia: 10-25 % Parkinson spectrum Vascular Dementia: 6-10 % Stroke related Frontotemporal Dementia: 2-5 % Personality or language problems

69
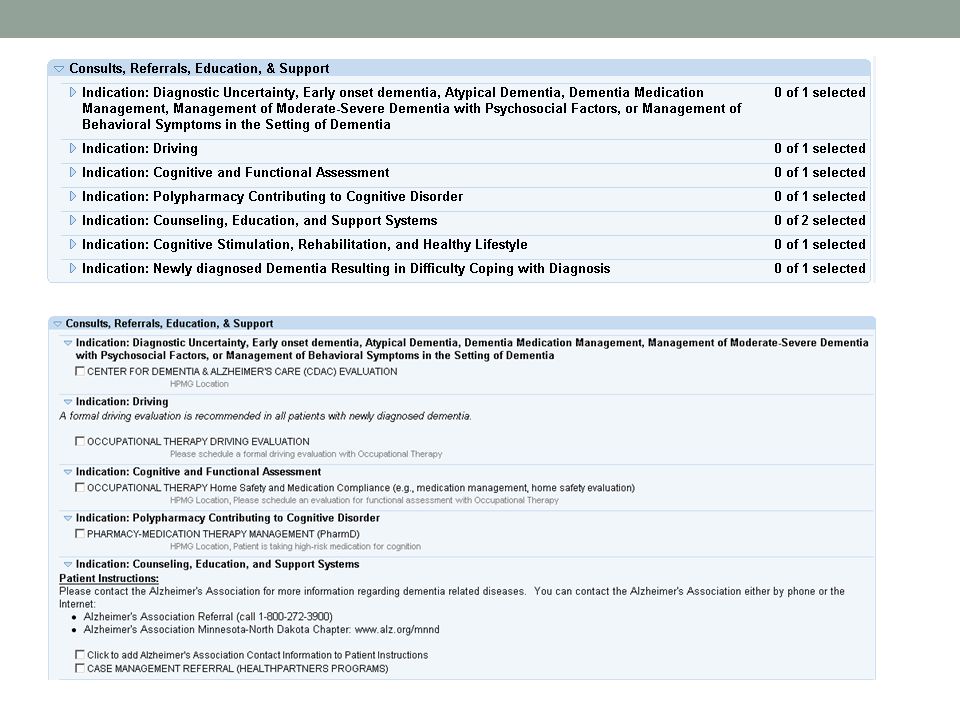
Intervention / Management Medication treatment Small component of care plan Referrals Senior LinkAge Line ® the 1-stop shop for MN Seniors Alzheimer’s Association and other community organizations Goals Provide education Connect to programs and services Increase dementia competence For patient AND family

70
ACT on Alzheimer’s Tools Care Coordination Toolkit

71
Care Coordination Tools Care Coordinators in Health Care Homes Care Coordination Checklist Cognitive Status / Dx ID Care Partner Care Plan Checklist Disease Stages

72
ACT on Alzheimer’s Tools EMR Tools

74
Use EMR to automate: Screening Work-up AVS with dementia education Internal orders and referrals Community supports

75
Partnering with Physicians & Clinics

76
Barriers to Community Connection 1. Under-diagnosis 2. Lack of understanding about benefits of non-drug treatment 3. Lack of knowledge about available resources 4. Missed / delayed connection to resources 5. Unprepared communities 76

77
Partnering with Physicians Doctors are motivated by things/people who: Help them improve patient care / outcomes Show me the data Save them time Reduce their stress Improve reimbursement Enhance recognition and appreciation YOU CAN DO ALL OF THESE THINGS

78
Building Relationships Talk to all who will listen You never know how your information will be passed on Be AUTHENTIC Be yourself and talk about what you know Build trust and credibility Return calls Do what you say and in a timely manner They will remember if you don’t

79
Real World Objections Many objections revolve around these issues: Cost: “My patients can’t afford your fee for care / time with a consultant.” Fear of Change: “I’ve been using this screening tool for years, and I know it like the back of my hand” or, “I don’t have time for new screens and processes.” Complacency: “There aren’t any really good medications, why should I diagnose?” and, “You can’t diagnose dementias properly with just these screens.” “What is the point of diagnosis? There is little that can be done.” Timing: “We are going through a big change (EMR, management) here right now; I don’t have time to make more changes.”
 here right now; I don’t have time to make more changes. .")
80
Real World Objections External input: “I need to talk to the clinic manager/my colleagues/nurse before I can move forward.” Personal/Office politics: “We have our own way of doing things with dementia patients. You’ll need to talk to our clinic manager.” Trust: “It sounds like you have something to offer but I’m not sure I have the time to make this work” and “If my clinic gives you all of our patients, how can you keep up?”

81
OBJECTIONS: Be Prepared Whatever organization you represent, you will get objections. You are asking for change. Most will resist. If you are asked a tough question, you can always say “I’m not sure about that answer; may I find out and email/call you with an answer when I have it?” Sometimes, objections are red herrings to distract you or put you off…then they don’t have to consider what you have to offer any more.

82
How Can I Get Clinicians to ACT? Find out what is causing them PAIN/distress/frustration regarding their geriatric/dementia patients They will not REALLY listen to you until you have uncovered or acknowledged the challenges that are causing them pain.

83
Partnering with Physicians Patient Doctor Care Partner

84
Partnership Goals Strengthen physician/agency relationship Encourage earlier diagnosis of dementia Increase referrals to agency

85
Making Headway Work on your “Elevator Speech”…10-30 seconds Walk in to the clinic…don’t be afraid Get name and number of contact person from front desk staff, and follow up Early mornings might be best for MD contact Always wear a name tag Have business cards ready Be prepared Try not to get frustrated, Don’t take it personally. Ask, “Are physicians my best target audience?”

86
Making Headway Ask patients / families for the name and number of their physician Communicate the patient’s care plan back to the provider Call the clinic, ask for the doctor’s nurse Ask nurse how to get the patient’s care plan to the doctor and in the patient chart / record Coach patient / family on how to partner with physicians Give the plan to the family and ask them to share with doctor Feedback loop Specific, concrete, brief, bullet points

87
651-254-7900 www.healthpartners.com/memoryloss
Similar presentations








 American Association of Geriatric Psychiatry (AAGP) March 2, 2007 J. Wesson Ashford, M.D., Ph.D. Stanford / VA Aging.>")



 Training Program>")





: The Role of Cognitive Assessment in Improving Health Outcomes Dr. William Mansbach October 25, 2011.>")






